Arq. Bras. Cardiol. vol.95 número3
Texto
Imagem

Documentos relacionados
Muitas hipóteses são levantadas, para que barreiras sejam criadas em torno da adoção por um casal gay, tais como: “A criança terá mais probabilidade de ter doenças mentais como
In our population, older age ( 55 years), hypertension and dyslipidemia were independent predictors of CAD in this subset of patients without calcium, and in the presence of
Com efeito, o objeto da estratégia não é um conjunto de unidades, mas um opo- nente recalcitrante (Brodie, 1965, p. A estratégia trata assim da conflitualidade hostil num
Prevalence of resistant hypertension in non-elderly adults: prospective study in a clinical setting. Arq
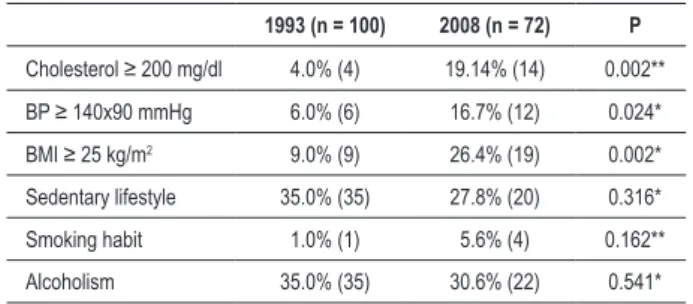
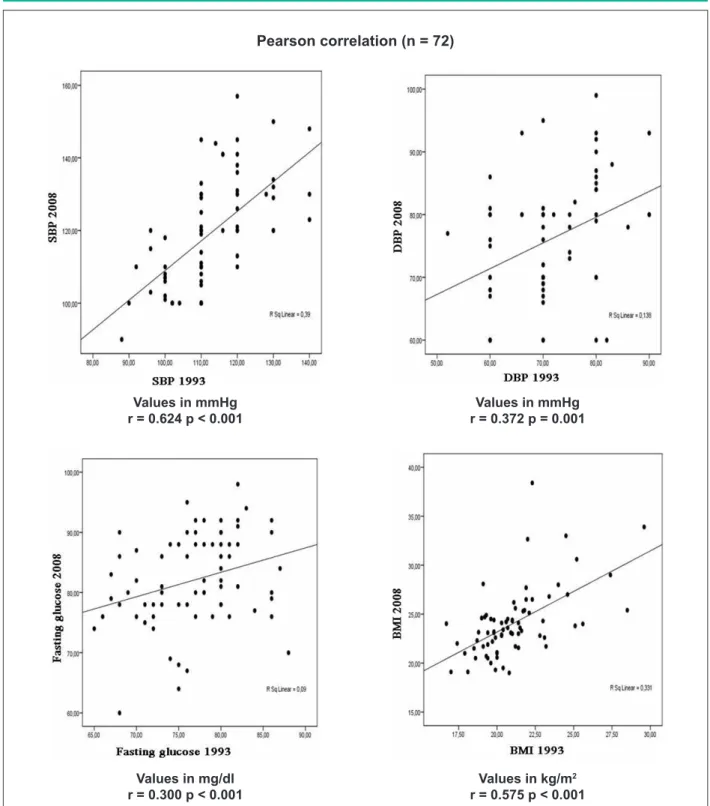
To report the prevalence of cardiovascular risk factors, particu- larly of systemic arterial hypertension, in the adult population of the Brazilian state of Rio Grande do Sul,
This study was designed to estimate cardiovascular risk factor prevalence in the adult population of Luzerna, state of Santa
A cannabis permanece como a substância ilícita mais consumida no mundo. Defendida por uns e “diabolizada” por outros, constitui uma das substâncias
estos extremos son los que en su día se recogieron en el catálogo de circunstancias a las que principalmente debía atenderse para establecer si la
