Rev. Bras. Ginecol. Obstet. vol.39 número8
Texto
Imagem



Documentos relacionados
The purpose of the present study was to compare the negative impacts of oral conditions in OHRQoL in pregnant women receiving or not comprehensive periodontal treatment,
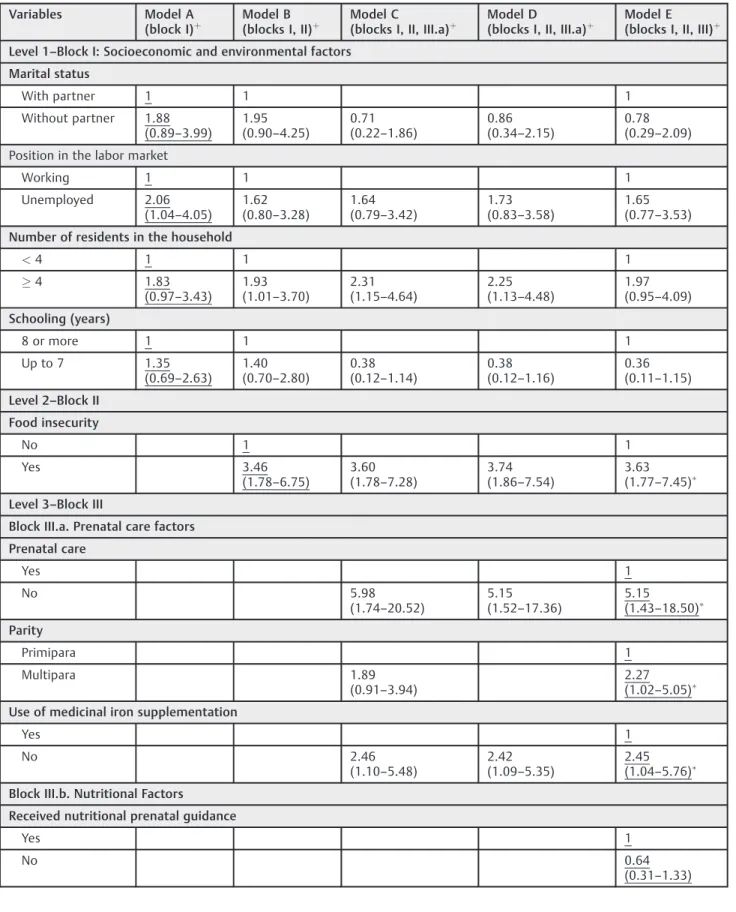
Conclusions In the present study, the chance of occurrence of anemia in pregnant women was signi fi cantly higher, mainly among women: in situations of food insecurity, not
The total volume and length of blood vessels were signi fi cantly increased in the LV, and the total blood vessel surface area was signi fi cantly higher in the RA of infected
As evidências empíricas apontam no sentido de que as crenças de autoeficácia estão enraizadas nas experiências de sucesso anteriores (Bandura, 1997, 2001),
A cross-sectional study was carried out with pregnant women cared for in the public health system in the city of Maceió , Brazil, in 2014, including 385 pregnant women and
Com relação aos dados flortsticos obtidos pelos levantamentos em questão, pode-se observar o se- guinte: o Botanal realizado em maio de 1986 (quar- to) foi o que atingiu maior
In the case of SLAM the map is built with collected data by the observation sensors and this data is arranged in the map according to the displacement of the robot measured by
Para isso, são utilizadas como base de trabalho duas fases de execução das obras: a organização do estaleiro e o arranque de obra, cuja eficiência dos
