h ttp : / / w w w . b j m i c r o b i o l . c o m . b r /
Clinical
Microbiology
Efficacy
and
safety
of
a
four-drug
fixed-dose
combination
regimen
versus
separate
drugs
for
treatment
of
pulmonary
tuberculosis:
a
systematic
review
and
meta-analysis
Glaura
C.
Lima
a,∗,
Emilia
V.
Silva
b,1,
Pérola
de
O.
Magalhães
c,1,
Janeth
S.
Naves
c,1,2aLaboratórioCentraldeSaúdePública(LACEN)-Brasília,DepartamentodeBiologiaMédica,Sec¸ãoMicobaterial,Brasília,DF,Brazil bUniversidadedeBrasília,FaculdadedeCeilândia,Brasília,DF,Brazil
cUniversidadedeBrasília,DepartamentodeFarmácia,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received22May2015 Accepted20June2016
Availableonline23December2016 AssociateEditor:AgnesMarieSá Figueiredo
a
b
s
t
r
a
c
t
Introduction:Tuberculosis,particularlymulti-drug-resistanttuberculosis,isamajorcauseof morbidityandmortalityworldwide.Tothebestofourknowledge,however,nostudytodate hasassessedthecombineduseofthefouravailabledrugsfortuberculosistreatment,which isanissueofgreatclinicalrelevance.
Objective:Todeterminewhetherthefour-drugfixed-dosecombinationissaferormore effec-tivethanseparatedrugsfortreatmentofpulmonarytuberculosis.
Methods:AsystematicreviewoftheliteraturewasperformedinaccordancewithPreferred ReportingItemsforSystematicReviewsandMeta-Analysesguidelines.
Results:Inpooledresultsfromfiverandomizedcontrolledtrialswith3502patientsacross Africa,Asia,andLatinAmerica,four-drugfixed-dosecombinationtherapywasnobetter thanseparatedrugstherapyintermsofcultureconversionafter2and6monthsof treat-ment.Therewerenosignificantdifferencesbetweenthegroupsinoverallincidenceof adverseeffects.However,themeta-analyticmeasure(logoddsratio)revealedthatseparate drugstreatmenthada1.65[exp(0.5)=1.65]increasedchanceofgastrointestinaladverse effectscomparedtofour-drugfixed-dosecombinationtreatment.
Conclusions:Thereviewedstudiesshowedthatfour-drugfixed-dosecombinationtherapy providesgreaterpatient comfortbyreducingthe numberof pillsandthe incidenceof gastrointestinaladverseeffects,aswellassimplifyingpharmaceuticalmanagementatall levels.
©2016SociedadeBrasileiradeMicrobiologia.PublishedbyElsevierEditoraLtda.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](G.C.Lima).
1 Theseauthorscontributedequallytothiswork.
2 Presentaddress:DepartmentofPharmacy,HealthScienceSchoolUniversityofBrasilia,CampusDarcyRibeiro,AsaNorte–Brasilia,
FederalDistrict70910-900,Brazil.
http://dx.doi.org/10.1016/j.bjm.2016.12.003
1517-8382/©2016SociedadeBrasileiradeMicrobiologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Tuberculosis(TB)continuestobeamajorcauseof morbid-ityandmortalityworldwide,with9millionnewcasesofTB diagnosedand1.5millionTB-related deathsrecorded glob-allyin2013.Approximately95%oftheestimatednumbersof TBcasesoccur inlow-income countries, with82% ofthese casesbeingconcentratedin22countries,amongwhichBrazil ranks17th.1ThisTBburdenisincreasedbyhuman
immuno-deficiencyvirus(HIV) infection,whichimpairstheimmune systemand allowsprogressiontoactiveTBdiseaseinlarge numbersofpeople.2
Furthermore, the global burden of drug-resistant TB is growing.In2010,anestimated650,000casesofdrug-resistant TBwerereportedworldwide.3Incidenceofdrug-resistantTB
hasbeenontheriseinBrazil,accordingtodataobtainedinthe SecondBrazilianNationalSurveyonAnti-TBDrugResistance 2007–2008.4In2014,theBrazilianMinistryofHealthdelivered
148GeneXpert instrument systemsto all92 municipalities thatcomprisethe RapidTB-TestNetwork,whichcovers all Brazilian states. These instrument systems are capable of diagnosing TBin 2h, while simultaneously identifying the sensitivityprofiletorifampicin,oneofthemaindrugsforTB treatment.5Alongsidetherisingprevalenceofdrug-resistant TB,therehasbeenanincreaseinthespreadofcasesdueto directcontactwithdrug-resistantTBpatients.Consequently, drug-resistantTBhasbecomeanepidemicitself,especially inhigh-burden settings.6,7 Multidrugresistanceisafurther
threatto TB control. Development of drug- or multi-drug-resistant(MDR) TBiscausedbyinadequaciesintreatment, suchasinthenumberofdrugsintheregimentowhichthe bacilliaresusceptible,thedoseordosingfrequency,thedrug quality,orthetreatmentadherence.3,8,9
Fixed-dosecombinations(FDCs)ofdrugsforTBtreatment have been advocated internationally to prevent the emer-gence ofdrugresistanceattributableto inappropriatedrug intake.10,11 Use of FDCs can reduce the risk of an
incor-rectdosage,simplifydrugprocurement,andaidinensuring adherencewithoutchangingthedrugdosage.In2010,Brazil’s NationalTBProgramaltered theirtraditionalanti-TB treat-ment (2RHZ/RH regimen), which comprised rifampicin (R), isoniazid (H), and pyrazinamide (Z) for 2 monthsfollowed byRand Hfor4months.Thechangefollowed areportby theSecondBrazilianNationalSurveyonAnti-TBDrug Resis-tance(2007–2008),whichshowedthatprimaryresistanceto HorH+Rhadincreasedfrom4.4%to6.0%andfrom1.1%to 1.4%,respectively,comparedtodatafromtheFirstBrazilian Survey(1995–1997).Inthenew2RHZE/4RHregimen,afourth drug,ethambutol(E),wasaddedtotheintensivephase(first2 months)ofTBtreatment.CapsulescontainingRandH, admin-isteredwithZtablets,werereplacedbyFDCtabletscontaining R,H,Z,andE.Inthenewformulation,HandZwere admin-isteredatlowerdosescomparedtothetraditional2RHZ/RH regimen.Pharmacological presentationofthis scheme is a tabletcontainingaFDCoffourdrugs:150mgofR,75mgof H,400mgofZ,and275mgofE.The2RHZE/RHschemeisstill recommendedforchildrenunder10yearsofage.4
ThebasictreatmentofTBwithfourdrugsisused world-wide, showing excellent effectiveness, particularly among
patientswithgoodtreatmentadherence.Withtheaddition ofafourthdrug, it isexpectedthattreatmentsuccesswill improve, preventing any further increase in resistance to H with or without R. FDC regimens have advantagessuch as improved patient comfortand treatment adherence (by reducingthenumberofpills)andsimplifiedpharmaceutical management atalllevels.4 Theaimsofthis newapproach
were to increase treatment adherence and prevent drug resistance.12
Overtheyears,problemshavebeenfoundwiththequality ofthe2RHZE/4RHregimen,suchasareducedbioavailabilityof R,instabilityoftheformulation,toxic/allergicAEs,and devel-opmentofresistance.Severalstudies havebeenconducted toassessthebioavailability,acceptability,and microbiologi-calefficacy ofRand H,withorwithout Z,administeredas aFDCfordailyorintermittentuse.13–17However,inpatients
withnewly diagnosedTB,theuse offour drugsina fixed-dosecombination(4-FDC)inthefirst2monthsoftreatment hasnotbeenassessedforsafetyandefficiencyrelativetothe administrationofseparatedrugs(SDs).
Toframerecentstudieswithinthebroaderevidencebase, wesystematicallyreviewedrandomizedclinicaltrials(RCTs) thatprovidedclinicaldataregardingtheefficacyandsafety of4-FDCdrugsinthetreatmentofpulmonaryTB.Thisstudy aimedtodeterminewhethertheadministrationof4-FDCis saferormoreeffectivethanSDregimensforthetreatmentof pulmonaryTB.
Methods
A systematic review was conducted in accordance with PreferredReportingItemsforSystematicReviewsand Meta-Analyses(PRISMA)guidelines.18Theprotocolforthisreview
wasrecordedon23May2013intheInternationalRegisterof Prospective SystematicReviews(PROSPERO)under registra-tionno.CRD42013003217.
Searchstrategyandselectioncriteria
Articleswere searchedinthefollowingdatabases: Cumula-tiveIndex toNursingandAllied HealthLiterature (CINAHL
– http://www.cinahl.com), Cochrane Library (http://www.
update-software.com/cochrane), Latin American and
Caribbean Literature in Health Sciences (LILACS; http://
lilacs.bvsalud.org/), MEDLINE (http://www.nlm.nih.gov),
Sci-entificElectronicLibraryOnline(SciELO;http://www.scielo.br), Scopus(http://www.scopus.com),WebofScience(http://www.
webofknowledge.com), Science Direct (http://www.
sciencedirect.com), ExcerptaMedica Database (EMBASE;
http://www.embase.com), CAPES Theses Database, and
public domain internet databases (http://www.periodicos.
capes.gov.br). All databases were searched from inception
through10September2013forarticlesinEnglish,French,and Spanish.WesoughttocompareresultsfromRCTsinvolving patientswithnewlydiagnosedTBwhowereadministereda 4-FDCorSDregimeninthefirst2monthsoftreatmentfor pulmonaryTB.Therefore,asearchstrategywasdevelopedby combiningthefollowingsearchterms:tuberculosis;treatment;
andnotHIV,asexplodedMedicalSubjectHeadings(MeSH) andfree-textterms.Additionally,abstractsfromthe follow-ingconferencesuntilSeptember2013weresearched:Union WorldConferenceonLungHealth,InterscienceConferenceon AntimicrobialAgentsandChemotherapy,SocietyofGeneral Microbiology,BritishThoracicSociety,EuropeanRespiratory Society,andtheAmericanThoracicSociety.Bibliographiesof allrelevantarticleswerealsoreviewed.
Dataextractionandmanagement
Twoindependentreviewers(GCLandEVS)andathirdreviewer (JSN)resolvedanydisagreementsonselectedstudies.Efficacy andsafetyofthetreatmentweretheprimaryandsecondary outcomes,respectively. Treatmentoutcomes were recorded accordingto definitionsadaptedfrom those giveninWHO guidelines.19 Briefly, treatment success was definedas the
numberofpatientswhowerecuredorwhocompleted com-binedtreatment.Defaultwasdefinedasfailureofthepatient toattendthehealthcareserviceforover30consecutivedays afterthe scheduledreturn date.Safety wasdefined asthe numberofAEs.
ThequalityofstudieswasassessedwiththeJadadscale.20
A predefined dataextraction form (in EXCEL) was used to extractdatafromeachstudyselectedforreview.The follow-inginformationwasrecorded:studycharacteristics,including authors, setting,study design, and hospitalization; patient characteristics,includingage,population,availabilityofdrug susceptibilitytesting,sputumconversionanddefaultratesat thebeginningandendoftreatment,observedAEs,previousTB regimens,HIVstatus,andothercomorbidities;andtreatment characteristics,includingthenumberofpatientsreceiving 4-FDCandSDregimens,andtreatmentoutcomes.
Dataanalysis
Whenpossible,statisticalcalculationswereperformedwith theRsoftwarepackage,version3.1.1.21Becauseallevaluated
outcomemeasuresweredichotomous,oddsratios(ORs)were calculated,withthe uncertainty oftheresultexpressed by theestimateofthe95%confidenceinterval(CI)aroundthis measure.Individualstudiesweregroupedbyeitherthe fixed-orrandom-effectsmethod,depending ontheresultsofthe testforhomogeneity.Homogeneityamongstudieswas evalu-atedbytheCochranQtest,withp>0.05indicatingstatistically significantdatahomogeneity.
Results
Studyselectionresults
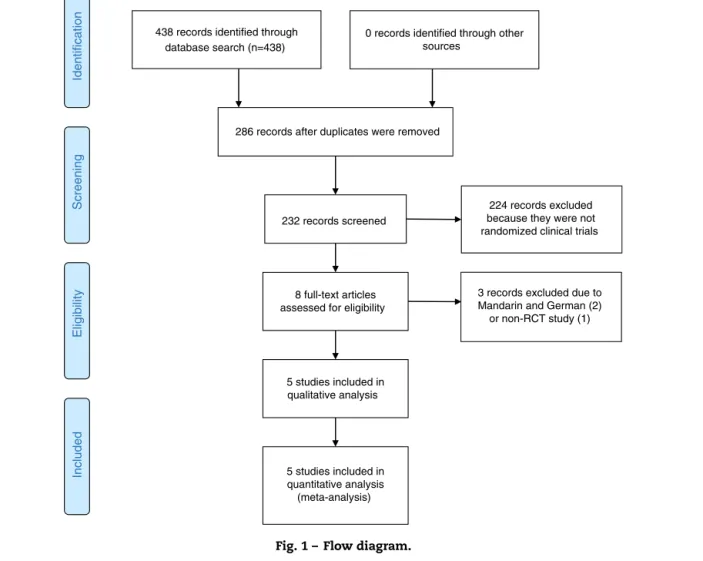
Thesearch strategy retrieved438 potential articles(Fig. 1). Twoarticles,onepublishedinMandarinandoneinGerman, were excluded due to language. One article was excluded forfailuretomeetthecriteriaofanRCT.Eightarticleswere screened as full-text articles, and five articles were sub-sequentlyanalyzed.14,22–25 All studies were conducted and
published in countries with a high incidence of TB. The
fivestudiesthatwereconsideredforanalysisincluded3502 patientsacrossAfrica,AsiaandLatinAmerica.
Studyandpatientcharacteristics
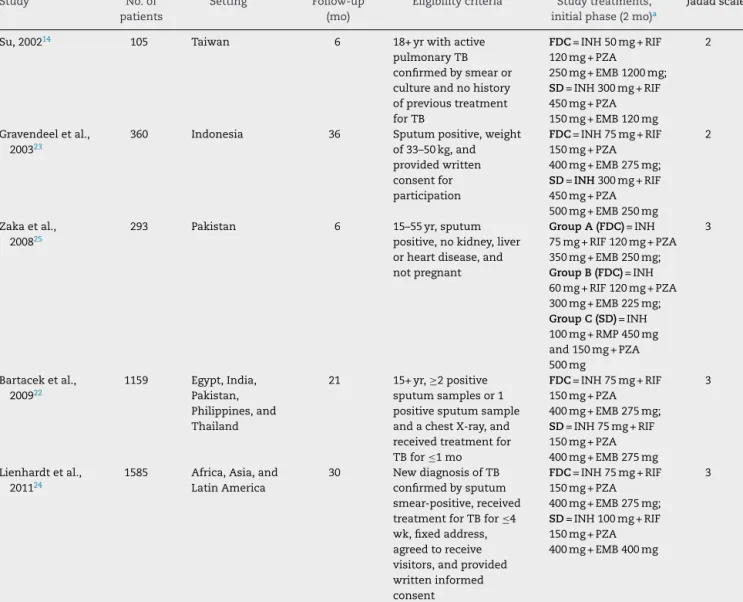
Study and treatment characteristics are summarized in
Table1.AllstudieswereRCTs.Ofthe3502includedpatients,
2072weremen(59.2%).Onlythreestudiesdetailedthemean patientage, withtheresultof35±15.3years.Inonestudy, patients were randomlyassigned tothree groups(A, B,C): patientsingroupsAand Bwere given4-FDC,andpatients ingroupCweregivenSDformulations.25Patientsintheother
studieswererandomizedintotwogroups(4-FDCandSD).All patientsinthestudiesreceivedthe4-FDCduringtheintensive phaseoftreatment.
TwostudiesprovidedinformationregardingHIVstatus.22,24
Inonestudy,2477ofthe1168patients(6.6%)wereHIVpositive.
Inanotherincludedstudy,22onlysixoutof1159patients(0.5%)
wereHIVpositive(oneintheFDCgroup,fiveintheSDgroup). Infourstudies,clinicalefficacywasmonitoredbyregularchest X-rays.14,22,24,25
Twostudiesprovideddatafromdrugsensitivitytests.14,24
Inonestudy,14fourpatientsintheFDCgroupandsixpatients
intheSDgrouphadPZA-resistantbacilli.Twopatientsinthe SDgrouphadEMB-resistantbacilli.Inanotherstudy,241132
patients(573FDC,559SD)weretestedfordrugsensitivity.Fully sensitiveorganismswereidentifiedin508FDCpatients(88.2%) and 497SD patients(88.9%).Non-MDR,H-resistantisolates wereobservedin65FDCpatients(11.3%)and62SDpatients (11.1%).
Only one study evaluated or reported weight gain, a decrease in the erythrocyte sedimentation rate, and an increaseinhemoglobinintheinitialandcontinuationphases oftherapy.25Inanotherstudy,onepatientintheFDCgroup
(1/51,2%)experiencedbacterialrelapseafter5monthsof suc-cessfulcompletionoftheinitialcourseoftreatment.14
Adverseevents
Table2summarizes theAEsreportedbytheincluded
stud-ies.Themostcommon AEswere gastrointestinal disorders (nausea,vomiting),whichwerereportedbyallstudies. How-ever, dermatological, rheumatologic,and hepatic problems, andevendeath,werecited.Allstudiesfoundthatthe differ-encebetweenthe4-FDCandSDgroupsintheoverallnumber ofdrug-relatedAEswasnolongersignificantaftergeneral dis-orderswereexcluded.Threestudiesreportedpatientdeath. Onestudy,24 reportedeightdeaths,whichweremostlikely
(2/591inFDCand2/579inSDgroup)orpossiblyduetoTB (2/591inFDCand2/579inSDgroup).Inanotherstudy,only onedeathwasreported,whichwasinthe SDgroup.25
Bar-taceketal.reported15deaths(11inFDCand4inSDgroup), butonlytwoofthem(twohepatitiscases,bothinFDCgroup) wereconsideredtobedrug-related.22
Onestudyreportedlessfrequentmuscle-jointeffects dur-ingtheintensivephaseoftreatmentinapatientreceivingthe FDCregimen.23Onlyonestudyevaluatedpatient
acceptabil-ity ofmedication,intermsoftaste,number oftablets,and problemswithswallowing.Thepaperreportedsignificantly
438 records identified through database search (n=438) Screening Included Eligibility Identification
0 records identified through other sources
286 records after duplicates were removed
232 records screened
224 records excluded because they were not randomized clinical trials
8 full-text articles assessed for eligibility
3 records excluded due to Mandarin and German (2) or non-RCT study (1) 5 studies included in qualitative analysis 5 studies included in quantitative analysis (meta-analysis)
Fig.1–Flowdiagram.
improvedpatientacceptabilityoftheregimeninthe4-FDC group.22
Studyquality
Toevaluatethe methodologicalqualityofincludedtrials, a Jadadscalebasedonthreequestionswasused.Scoresgreater than3areindicativeofhigh-qualitystudies,andscoresof2 orlessareindicativeoflow-qualitystudies.20Threestudies
hadahighqualityscore,andtwostudieswereconsideredlow quality.
Treatmentoutcomes
Ameta-analysiswasdevelopedforeachvariableinthestudy. Testedvariablesincludedthefollowing:ratesofsputum con-versioninthe initialphaseoftreatment(assessedwithin2 monthsoftreatment initiation), sputum conversion inthe finalphaseoftreatment,default,numberofpatientswithAEs, andnumber ofpatientswithgastrointestinalAEs.For each variable,thefollowingnullhypothesiswastested:
H0. Theeventofinterest(variable)hasthesamechanceof occurringinbothtreatmentgroups(4-FDCandSD).
Fortheanalysisofsputumconversionintheinitialphase oftreatment (≤2months),all five studies collected related dataand wereconsideredintheanalysis. Thefixed-effects modelwaschosenbecauseheterogeneitywasnotidentified (p=0.3169).Thenullhypothesiswasnotrejected(p=0.4922), suggestingthattherewasnostatisticalevidencethattherate ofsputumconversionintheinitialphaseoftreatment dif-feredbetweentreatmentgroups.Aforestplot(Fig.2)showed that the 95% CI range for the log OR contained zero (log OR: −0.09, 95% CI: −0.37 to 0.18), indicating that the OR betweentreatmentswasstatisticallyequaltoone.Therefore, meta-analysisresultsdidnotrevealastatisticallysignificant differencebetween4-FDCandSDtreatmentsintermsofthe rateofsputumconversionintheinitialphaseoftreatment.
Fortheanalysisofsputumconversioninthefinalphase of treatment, onestudy,25 did notcollect related data and
wasexcludedfromtheanalysis.Thefixed-effectsmodelwas chosen because heterogeneity was not identified (p=0.98). Thenullhypothesiswasnotrejected(p=0.5037),suggesting thattherewasnostatisticalevidencethatsputumconversion inthe finalphaseoftreatmentdifferedbetweentreatment groups.Aforestplot(Fig.3)showedthatthe95%CIrangefor thelogORcontainedzero(logOR:0.14,95%CI:−0.27to0.54), indicatingthattheORbetweentreatmentswasstatistically equaltoone.Therefore,meta-analysisresultsdidnotreveala
Table1–Characteristicsofrandomizedclinicaltrials,comparingFDCwithSDregimensfortreatmentofTB,thatwere
includedinthesystematicreview.
Study No.of
patients
Setting Follow-up
(mo)
Eligibilitycriteria Studytreatments,
initialphase(2mo)a
Jadadscale
Su,200214 105 Taiwan 6 18+yrwithactive pulmonaryTB confirmedbysmearor cultureandnohistory ofprevioustreatment forTB FDC=INH50mg+RIF 120mg+PZA 250mg+EMB1200mg; SD=INH300mg+RIF 450mg+PZA 150mg+EMB120mg 2 Gravendeeletal., 200323
360 Indonesia 36 Sputumpositive,weight of33–50kg,and providedwritten consentfor participation FDC=INH75mg+RIF 150mg+PZA 400mg+EMB275mg; SD=INH300mg+RIF 450mg+PZA 500mg+EMB250mg 2 Zakaetal., 200825
293 Pakistan 6 15–55yr,sputum positive,nokidney,liver orheartdisease,and notpregnant GroupA(FDC)=INH 75mg+RIF120mg+PZA 350mg+EMB250mg; GroupB(FDC)=INH 60mg+RIF120mg+PZA 300mg+EMB225mg; GroupC(SD)=INH 100mg+RMP450mg and150mg+PZA 500mg 3 Bartaceketal., 200922 1159 Egypt,India, Pakistan, Philippines,and Thailand 21 15+yr,≥2positive sputumsamplesor1 positivesputumsample andachestX-ray,and receivedtreatmentfor TBfor≤1mo FDC=INH75mg+RIF 150mg+PZA 400mg+EMB275mg; SD=INH75mg+RIF 150mg+PZA 400mg+EMB275mg 3 Lienhardtetal., 201124
1585 Africa,Asia,and LatinAmerica
30 NewdiagnosisofTB confirmedbysputum smear-positive,received treatmentforTBfor≤4 wk,fixedaddress, agreedtoreceive visitors,andprovided writteninformed consent FDC=INH75mg+RIF 150mg+PZA 400mg+EMB275mg; SD=INH100mg+RIF 150mg+PZA 400mg+EMB400mg 3
EMB,ethambutol;FDC,fixed-dosecombination;INH,isoniazid;PZA,pirazinomide;RIF,rifampin;SD,singledose;TB,tuberculosis.
a DoseswereadministeredonthebasisofbodyweightaccordingtoWHOandTheEuropeanUnionrecommendations.
FE Model
2.00 0.00 –2.00 –4.00
Log Odds Ratio Lienhardt (2011) Bartacek (2009) Zaka (2008) Gravendeel (2003) Su (2002) –0.04 [ –0.45 , 0.37 ] 0.10 [ –0.33 , 0.52 ] –1.34 [ –3.49 , 0.80 ] –0.66 [ –1.43 , 0.11 ] –0.87 [ –3.03 , 1.29 ] –0.09 [ –0.37 , 0.18 ]
Fig.2–Forestplotforrateofsputumconversioninthe initialphaseoftreatment(≤2monthsafterstartof treatment).
statisticallysignificantdifferencebetween4-FDCandSD treat-ments interms ofsputumconversioninthefinalphaseof treatment.
For the analysis of default, one study,25 did not collect
related data.Asitwas notpossibletocontacttheauthors, thisstudywasexcludedfromtheanalysis.Thefixed-effects modelwaschosenbecauseheterogeneitywasnotidentified (p=0.0775).Thenullhypothesiswasnotrejected(p=0.9092), suggesting that there was no statistical evidence that the defaultdifferedbetweentreatmentgroups.Aforestplot(Fig.4) showedthatthe95%CIrangeforthelogORcontainedzero (log OR:0.05,95% CI:−0.82to0.92), indicatingthat theOR betweentreatmentswasstatisticallyequaltoone.Therefore, meta-analysisresultsdidnotrevealastatisticallysignificant difference between 4-FDC and SD treatments in terms of default.
FortheanalysisofthenumberofpatientswithAEs,two studies,14,23 did notcollectrelateddata andwere excluded
b r a z i l i a n j o u r n a l o f m i c r o b i o l o g y 4 8 (2 0 1 7) 198–207
203
FDC/SDgroup inFDCgroup inSDgroup death
Su,200214 26/25 Hyperuricemia(8),
skinitching(4),skin rash(2),drugfever (1),abnormalliver function(3)
Hyperuricemia(7), skinitching(7),skin rash(2),abnormal liverfunction(5), gastrointestinal disorders(5),blurred vision(2),sensation ofnumbness(1)
Notevaluated 1/57FDC Notevaluated
Gravendeeletal., 200323 198/162 Gastrointestinal disorders(81),skin reaction(83), muscle-joints(64) Gastrointestinal disorders(89),skin reaction(67), muscle-joints(73)
1/198FDC,2/162SD Notevaluated Notevaluated
Zakaetal., 200825 194/99 Gastrointestinal disorders(28),skin reaction(8), muscle-joints(3) Gastrointestinal disorders(23),skin reaction(3), muscle-joints(0), death(1)
53/197FDC,30/99SD 0/293FDCandSD 1caseingroupC
withsuspectedTB meningitis Bartaceketal., 200922 558/564 Skindisorders(40); asthenia,headache, fever(29); musculo-skeletal disorders(20); hepaticandbiliary disorders(14);others (19) Skindisorders(30); asthenia,headache, fever(5); musculo-skeletal disorders(22);liver andbiliarydisorders (21);others(8) 25/558FDC,15/564 SD 6/344FDC,3/360SD 2/558FDCcasesof hepatitis Lienhardtetal., 201124 798/787 Rheumatological(7); dermatological(16); hepatic(5);and gastrointestinal(6) disorders;others(3) Rheumatological (11);dermatological (15);hepatic(1);and gastrointestinal(11) disorders;others(4). 40/798FDC,39/787 SD 23/591FDC,19/579 SD 4/591FDC,4/579SD
FE Model
4.00 0.00 –4.00
Log Odds Ratio Lienhardt (2011) Zaka (2009) Gravendeel (2003) Su (2002) 0.14 [ –0.36 , 0.63 ] 0.32 [ –0.75 , 1.38 ] 0.01 [ –0.94 , 0.96 ] –0.04 [ –4.00 , 3.92 ] 0.14 [ –0.27 , 0.54 ]
Fig.3–Forestplotforsputumconversioninthefinalphase oftherapy.
theauthorsofthesestudies.Therandom-effectsmodelwas chosenbecauseheterogeneitywasidentified(p=0.0246and
I2=75.85%).Thenullhypothesiswasnotrejected(p=0.4091),
suggesting that there was no statistical evidence that the number of patients with AEs differed between treatment groups.A forestplot(Fig.5)showedthat the95% CIrange forthelogORcontainedzero(logOR:0.24,95%CI:−0.32to 0.79),indicatingthattheORbetweentreatmentswas statis-ticallyequaltoone.Therefore,meta-analysisresultsdidnot revealastatisticallysignificantdifferencebetween4-FDCand SDtreatmentsintermsofthenumberofpatientswithAEs.
Fortheanalysisofthenumberofpatientswith gastroin-testinalAEs,allfivestudiescollectedrelateddataandwere includedintheanalysis.Thefixed-effectsmodelwaschosen becauseheterogeneitywasnotidentified(p=0.5656).Thenull hypothesiswasrejected(p=0.0006),suggestingthattherewas statisticalevidencethatthechanceofoccurrenceof gastroin-testinalAEsdifferedbetweentreatmentgroups.Aforestplot (Fig.6)showedthatthe95%CIrangeforthelogORdidnot con-tainzero(logOR:0.50,95%CI:0.22–0.79),indicatingthattheOR betweentreatmentswasstatisticallydifferentfromone.The meta-analyticmeasure(logOR)revealedthattheSDtreatment wasassociatedwitha1.65-fold[i.e.,exp (0.5)=1.65]greater likelihoodofgastrointestinalAEsthanthe4-FDCtreatment.
FE Model
2.00 –2.00 –6.00
Log Odds Ratio Lienhardt (2011) Bartacek (2009) Gravendeel (2003) Su (2002) –2.20 [ –4.29 , –0.12 ] 1.63 [ –0.54 , 3.80 ] 0.70 [ –1.82 , 3.21 ] 0.16 [ –1.02 , 1.34 ] 0.05 [ –0.82 , 0.92 ]
Fig.4–Forestplotfordefault.
RE Model
1.50 0.50
–0.50
Log Odds Ratio Lienhardt (2011) Bartacek (2009) Zaka (2008) 0.17 [ –0.32 , 0.66 ] –0.14 [ –0.42 , 0.14 ] 0.90 [ 0.19 , 1.61 ] 0.24 [ –0.32 , 0.79 ]
Fig.5–Forestplotfornumberofpatientswithadverse effects. FE Model 6.00 4.00 2.00 0.00 –2.00
Log Odds Ratio Lienhardt (2011) Bartacek (2009) Zaka (2008) Gravendeel (2003) Su (2002) 0.63 [ –0.37 , 1.63 ] 0.34 [ –0.17 , 0.84 ] 0.31 [ –0.50 , 1.12 ] 0.61 [ 0.18 , 1.03 ] 2.65 [ –0.30 , 5.61 ] 0.50 [ 0.22 , 0.79 ]
Fig.6–Forestplotfornumberofpatientswith gastrointestinaladverseeffects.
Discussion
OnthebasisofthepooledresultsoftheRCTs,4-FDCtherapy failedtoshowbenefitsovertheSDregimeninculture conver-sionafter2or6monthsoftreatment. However,theresults did notdemonstratecomplete inferiorityofFDCcompared to SDregimens when usingthe strict definitionappliedin thisreview.Exceptforonestudythatidentifiedbetter treat-ment satisfaction,22 noneoftheincluded studiesidentified
improvedpatientadherenceamongTBpatientstreatedwith 4-FDCcomparedtothosetreatedwithSDformulations.
Mostofthesideeffectsthatwerereportedbythestudiesin thisreviewwerenotconsideredseriousandcouldbemanaged through symptomaticpalliation in bothgroups ofpatients (4-FDC andSD). Eveninastudy that reported176patients (86%)with atleast oneAEassociatedwithtreatment,only twopatientsabandonedthestudybecauseofAEs.26
Gastroin-testinalsideeffects,suchasdiarrheaandmalabsorption,can hinderachievementofoptimalbloodconcentrationsof anti-TBdrugsinpatientsco-infectedwithHIV.27Thisobservation
suggeststhat4-FDCtherapy,bycausingfewergastrointestinal sideeffects,wouldbenefitco-infectedpatients.Somepatients
reportedstoppingmedicationbecauseofAEs,28whereas
oth-ersindicatedthattheywerenotinformedaboutsideeffects orwhattodotocounterthem.29–31NoophthalmicAEs
(ocu-lartoxiceffects)werereportedthatcouldbeassociatedwith thenewdrug(EMB).Retrobulbaropticneuritis,themainAEto EMB,israreinthedosesandexposuretimescommonlyused forTBtreatment.32
Despite the potential for providing the highestlevel of evidence in therapeutic intervention research, RCTs have beencriticizedbecauseoftheirlimitedgeneralizability.RCTs are often conducted under optimalmedical care and may underestimatethepotentialbenefitofusing4-FDC formula-tionstoenhanceadherenceinsettingswheremalpracticeor unmonitored therapiesare common.Importantdifferences inadherence have been foundinmany RCTs.33 Therefore,
pragmatic clinical trials, which are conducted in a way thatmorecloselyresemblestypicalclinicalpractice,maybe moreappropriate toobtain abetter estimate oftreatment effectiveness.34,35
Atthebeginning of2013,a systematicreviewwas pub-lished in Canada to evaluate the risk of treatment failure or disease relapse, acquired drugresistance, bacterial con-version after 2 months of treatment, AEs, adherence, and treatmentsatisfactionassociatedwithtreatmentofactiveTB usingFDCorSDformulations.36 Thisstudy concludedthat,
althoughFDCformulationssimplifyTBtherapy,thecurrent evidencedid notindicate thatthese formulations improve treatment outcomes among patients with activeTB. How-ever,thatsystematicreviewincludedstudiesofbothfour-drug andtwo-drugcombinationsand,therefore,differsfromthe presentoneinthenumberofretrievedarticles.These differ-encesjustifytheneedforarevisiontocomparepreciselythe effectof4-FDCversusSDformulations.
TheWorldHealthOrganizationhasrecommended4-FDC treatments since1999. Combined treatments preventdrug selectionbythepatient(monotherapy)byprovidingallofthe drugsinthesametablet.12,34,35,37Duetotheirsimplifiedand
standardizednature,4-FDCregimensfacilitatedosage calcu-lationand preventprescriptionerrors.However,oneofthe mostrelevantfeaturesof4-FDCformulations,theprevention ofdrugresistance,wasnotaddressedinthosestudies. Nev-ertheless,basedontheirsimilarefficacies,user-friendliness, lowercosts,andoperationalandlogisticaladvantages, gen-eralized use of 4-FDC formulations should continue to be recommended.
Onelimitationofthismeta-analysisisthattheincluded studies did not investigate adherence to the prescribed treatment. Moreover, the impact of the Directly Observed TreatmentShort-Course(DOTS)strategyontheoutcomesof TBtreatmentwasnotassessed,whichresultedinless pre-cise estimates. Another limitation is the inconsistency in ascertainmentofthetimeofrelapseinthedifferentstudies; becauseoftheheterogeneousmethods,wedidnotpoolthe studyresultsforthisvariable.Wecould notassess mortal-ityasanoutcomebecausethistermwasdefineddifferently inthestudies(all-causevs.TB-specificmortality),measured over differentfollow-up periodsand, insomestudies,was notreportedornotattributedtothetreatmentgroup.Finally, small differences in drug concentrations existed between studies.Regardlessoftheselimitations,thissystematicreview
hasseveralstrengths.Lackofsignificantheterogeneityofthe estimatesofsputumconversionintheinitialandfinalphases of therapy and of defaultin the different trials permitted poolingandincreasedtheprecisionofourresultsregarding treatmentefficacy.
By the end of 2009,Brazil was the onlycountry witha high burden ofTBto use athree-drugtreatment regimen. Despiteafree-of-chargetreatment,themeandefaultratewas approximately9.3%andreached14% insomestates.38Ina
Braziliandescriptivestudybasedonprospectivedataobtained from themedicalrecords ofadultTBpatientstreatedwith 4-FDCtablets,theobtainedcureratesweresimilartothose obtainedwithSDtreatments.However,therateoftreatment abandonmentwasmuchhigher(17.5%)thanthatconsidered appropriate(≤5%).Thesedatastronglysuggestthattheuse ofFDCtabletsdoesnothaveasignificantimpacton adher-encetotreatment.Therefore,measurestoimproveadherence, suchassupervisedtreatment,shouldnotbeneglected.11In
addition,studiesconductedinBrazilhavedemonstratedthe associationbetweenlowerratesoftreatmentabandonment andsupervisedtreatment.39–41
Thenew4-FDC regimenwasexpectedtoresultinlower defaultrates andhigher effectivenessoftreatmentby pre-ventingdrugselectionandthefurtherappearanceofresistant pathogens.To ensuresuccessofthenewtreatment, better careandattentiontopatients,includingexpansionofDOTS strategyinBrazil,areneeded. Intheanalysisofthe Brazil-ian case, Zuim et al. said that the success of TB control, as with other health problems, goes beyond the availabil-ityofdiagnostictestsanddrugs,requiringmeasuresrelated to the establishment of links between health profession-als and health system users.42 Corroborating that idea, in
Taiwan, aprospective RCTwas conductedusing the DOTS strategytocomparethe safetyand efficacyoftwotypesof anti-TB regimens (FDCversus SD)for pulmonaryTB treat-ment. No significant difference in safety or efficacy was found between the groups when the DOTS strategy was used.43
Of the 22 high TB-burden countries, Brazil is the last toadoptthe 4-FDC regimen.38 Gemaletal. statedthat the
maintenanceoflow resistancerates inBrazil comparedto othercountriesmightbebecausemedicinesaredistributed exclusivelybypublichealthservices,inaccordancewiththe logisticssystemoftheMinistryofHealth.44
Conclusion
Amongthefivevariables,onlygastrointestinalAEsdiffered significantlybetweentreatments(SDand4-FDC),witha meta-analytic measurement equalto 0.50 and a p-value of less than 0.001. All of the studies showed that 4-FDC therapy providesgreaterpatientcomfortbyreducingthenumberof pills and the incidence of gastrointestinal AEs, which are the most-reported side effects, in addition to simplifying pharmaceuticalmanagement atall levels.Therefore,4-FDC therapy isan important evolution inTB treatment. These therapies shouldbeimplemented withsimultaneous phar-macovigilancestudiesandpragmatictrialdesignstosimulate real-worldclinicalpractice,associatedwithnewtechnologies
andmeasurestoestablishlinksbetweenhealthprofessionals andhealthsystemusers.
Funding
Thisworkhasnotreceivedanyfunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. TheWorldHealthOrganization.TreatmentOutcomes.The
GlobalTuberculosisReport.Geneva,Switzerland:WHOPress; 2014.
2. SkrahinA,AhmedR,FerraraK,etal.Autologous
mesenchymalstromalcellinfusionasadjuncttreatmentin
patientswithmultidrugandextensivelydrug-resistant
tuberculosis:anopen-labelphase1safetytrial.LancetRespir
Med.2014;2(2):108–122.
3. TheWorldHealthOrganization.TheBurdenofDiseaseCaused
byTB.TheGlobalTuberculosisReport.Geneva,Switzerland:
WHOPress;2012:8–28.
4. BRAZIL,MinistryofHealth.SecretaryofHealthSurveillance DepartmentofEpidemiologicalSurveillance.NationalTuberculosis ControlProgramme.TechnicalNoteontheChangesinthe TreatmentofTuberculosisinBrazilforAdultsandTeenagers– Version2;2009.Availablefrom:http://portal.saude.gov.br/
portal/arquivos/pdf/notatecnicaversao28deagostov5.
pdf[cited10.11.14].
5. BRAZIL,MinistryofHealth.DepartmentofManagementand IncorporationofTechnologiesinHealthSecretaryofScience. TechnologyandSuppliesStrategic–DGITS/SCTIE.National TechnologyIncorporationCommissiononSUS(CONITEC).Report No.49;2013.Availablefrom:http://www.fundacaoataul
phodepaiva.com.br/wp-content/uploads/2013/03/Relatorio-XpertMTBRIF-CP5.pdf[acessed22.10.15].
6. KeshavjeeS,FarmerPE.Pickingupthepace-scale-upofMDR
tuberculosistreatmentprograms.NEnglJMed.
2010;363:1781–1784.
7. TheWorldHealthOrganization.GlobalTuberculosisReport.
Geneva,Switzerland:WHOPress;2015.
8. WrightA,ZignolM,VanDeunA,etal.GlobalProjecton
Anti-TuberculosisDrugResistanceSurveillance
Epidemiologyofantituberculosisdrugresistance2002–07:an
updatedanalysisoftheGlobalProjectonAnti-Tuberculosis
DrugResistanceSurveillance.Lancet.2009;373:1861–1873.
9. MalanguN,MngomezuluM.Evaluationoftuberculosis
infectioncontrolmeasuresimplementedatprimaryhealth
carefacilitiesinKwazulu-NatalprovinceofSouthAfrica.
BMCInfectDis.2015;15:117.
10.TheUnionAnti-tuberculosisRegimensofChemotherapy.
RecommendationsfromtheCommitteeonTreatmentofthe
InternationalUnionagainstTuberculosisandLungDisease.
BullIntUnionTubercLungDis.1988;63(2):60–64.
11.FerreiraAC,SilvaJuniorJL,CondeMB,RabahiMF.Clinical
treatmentoutcomesoftuberculosistreatedwiththebasic
regimenrecommendedbytheBrazilianNationalMinistryof
Healthusingfixed-dosecombinationtabletsinthegreater
metropolitanareaofGoiania,Brazil.JBrasPneumol.
2013;39(1):76–83.
12.BlombergB,FourieB.Fixed-dosecombinationdrugsfor
tuberculosis:applicationinstandardisedtreatment
regimens.Drugs.2003;63:535–553.
13.AcocellaG,NonisA,Gialdroni-GrassiG,GrassiC.
Comparativebioavailabilityofisoniazid,rifampin,and
pyrazinamideadministeredinfreecombinationandina
fixedtripleformulationdesignedfordailyusein
antituberculosischemotherapy.I.Single-dosestudy.AmRev
RespirDis.1988;138:882–885.
14.SuWJ,PerngRP.Fixed-dosecombinationchemotherapy
(Rifater/Rifinah)foractivepulmonarytuberculosisin
Taiwan:atwo-yearfollow-up.IntJTubercLungDis.
2002;6(11):1029–1032.
15.GohelMC,SarvaiyaKG.Anovelsoliddosageformof
rifampicinandisoniazidwithimprovedfunctionality.AAPS
PharmSciTech.2007;8:E68.
16.BhutaniH,MariappanTT,SinghS.Thephysicaland
chemicalstabilityofanti-tuberculosisfixed-dose
combinationproductsunderacceleratedclimaticconditions.
IntJTubercLungDis.2004;8:1073–1080.
17.HiremathPS,SahaRN.Oralmatrixtabletformulationsfor
concomitantcontrolledreleaseofanti-tuberculardrugs:
designandinvitroevaluations.IntJPharm.2008;362:118–125.
18.MoherD,LiberatiA,TetzlaffJ,AltmanDG.Preferred
reportingitemsforsystematicreviewsandmeta-analyses:
thePRISMAstatement.JClinEpidemiol.2009;62:1006–1012.
19.TheWorldHealthOrganization.TreatmentofTuberculosis:
GuidelinesforNationalProgrammes.4thed.Geneva,
Switzerland:WHOPress;2010.
20.JadadAR.RandomizedControlledTrials.BMJBooks;1998. Availablefrom:http://www.bmjpg.com/rct/maex.htlm
[accessed03.10.13].
21.CoreTeamR.R:ALanguageandEnvironmentforStatistical Computing.Vienna,Austria:RFoundationforStatistical Computing;2014.Availablefrom:http://www.r-project.org/.
22.BartacekA,SchuttD,PanoschB,BorekM,Rimstar,FDC
StudyGroup.Comparisonofafour-drugfixed-dose
combinationregimenwithasingletabletregimenin
smear-positivepulmonarytuberculosis.IntJTubercLungDis.
2009;13(6):760–766.
23.GravendeelJM,AsapaAS,Becx-BleuminkM,VrakkingHA.
Preliminaryresultsofanoperationalfieldstudytocompare
side-effects,complaintsandtreatmentresultsofa
single-drugshort-courseregimenwithafour-drug
fixed-dosecombination(4FDC)regimeninSouthSulawesi,
RepublicofIndonesia.Tuberculosis(Edinb).2003;83:183–186.
24.LienhardtC,CookSV,BurgosM,etal.Efficacyandsafetyofa
4-drugfixed-dosecombinationregimencomparedwith
separatedrugsfortreatmentofpulmonarytuberculosis:the
StudyCrandomizedcontrolledtrial.JAMA.
2011;305:1415–1423.
25.Zaka-Ur-RehmanZ,JamshaidM,ChaudhryA.Clinical
evaluationandmonitoringofadverseeffectsforfixed
multidosecombinationagainstsingledrugtherapyin
pulmonarytuberculosispatients.PakJPharmSci.
2008;21:185–194.
26.LeimaneV,RiekstinaV,HoltzTH,etal.Clinicaloutcomeof
individualisedtreatmentofmultidrug-resistanttuberculosis
inLatvia:aretrospectivecohortstudy.Lancet.
2005;365:318–326.
27.ZumlaA,ChakayaJ,CentisR,etal.Tuberculosistreatment
andmanagement—anupdateontreatmentregimens,trials,
newdrugs,andadjuncttherapies.LancetRespirMed.
2015;3:220–234.
28.MunroSA,LewinSA,SmithHJ,EngelME,FretheimA,
VolminkJ.Patientadherencetotuberculosistreatment:a
systematicreviewofqualitativeresearch.PLoSMed.
29.JaiswalA,SinghV,OgdenJA.Adherencetotuberculosis
treatment:lessonsfromtheurbansettingofDelhi,India.
TropMedIntHealth.2003;8(July(7)):625–633.
30.EdgintonME,SekataneCS,GoldsteinSJ.Patients’beliefs:do
theyaffecttuberculosiscontrol?Astudyinaruraldistrictof
SouthAfrica.IntJTubercLungDis.2002;6(December
(12)):1075–1082.
31.WaresDF,SinghS,AcharyaAK,DangiR.Non-adherenceto
tuberculosistreatmentintheeasternTaraiofNepal.IntJ
TubercLungDis.2003;7:327–335.
32.AmericanThoracicSociety,CDC,andInfectiousDiseases
SocietyofAmerica.TreatmentofTuberculosis.MMWR.
2003;52(RR-11):1–82.Erratum:MMWR.2005;53(51–52):
1195–222.
33.HaynesRB,AcklooE,SahotaN,McDonaldHP,YaoX.
Interventionsforenhancingmedicationadherence.Cochrane
DatabaseSystRev.2008;2:CD000011.
34.ChalkidouK,TunisS,WhicherD,FowlerR,ZwarensteinM.
Theroleforpragmaticrandomizedcontrolledtrials(pRCTs)
incomparativeeffectivenessresearch.ClinTrials.
2012;9:436–446.
35.TunisSR,StryerDB,ClancyCM.Practicalclinicaltrials:
increasingthevalueofclinicalresearchfordecisionmaking
inclinicalandhealthpolicy.JAMA.2003;290:1624–1632.
36.AlbannaAS,SmithBM,CowanD,MenziesD.Fixed-dose
combinationantituberculosistherapy:asystematicreview
andmeta-analysis.EurRespirJ.2013;42:721–732.
37.BlombergB,SpinaciS,FourieB,LaingR.Therationalefor
recommendingfixed-dosecombinationtabletsfortreatment
oftuberculosis.BullWorldHealthOrgan.2001;79:61–68.
38.DalcolmoMP.TratamentodaTBsensíveleresistente.Pulmão
RJ.2012;21(1):55–59.
39.FerreiraSM,SilvaAM,BotelhoC.Noncompliancewith
treatmentforpulmonarytuberculosisinCuiaba,intheState
ofMatoGrosso–Brazil.JBrasPneumol.2005;31(5):427–435.
40.SouzaMS,PereiraSM,MarinhoJM,BarretoML.
Characteristicsofhealthcareservicesassociatedwith
adherencetotuberculosistreatment.RevSaudePublica.
2009;43(6):997–1005.
41.VieiraAA,RibeiroSA.Compliancewithtuberculosis
treatmentaftertheimplementationofthedirectlyobserved
treatment,short-coursestrategyinthecityofCarapicuíba,
Brazil.JBrasPneumol.2011;37(2):223–231.
42.ZuimR,MenezesA,TrajmanA.TheBrazilianexperienceof
implementingRHZEfixed-dosecombinationfortuberculosis
treatment.EpidemiolServSaude.2014;23:537–540.
43.ZhangHQ,XiXE,WangYL,HanW,ZhangCX,JiaoJH.Side
effectsoftuberculosistreatmentwithfixed-dose
combinations.JBiolRegulHomeostAgents.2015;29(2):379–388.
44.GemalA,KeravecJ,MenezesA,TrajmanA.CanBrazilplaya
moreimportantroleinglobaltuberculosisdrugproduction?
Anassessmentofcurrentcapacityandchallenges.BMC