Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1164
CLINICAL STUDY OF MECHANICAL OCULAR INJURIES AND THEIR VISUAL
OUTCOME
Suresha Anepla Rajappa1, Supriya Khardenavis2, Aditi Samirbhai Parikh3
HOW TO CITE THIS ARTICLE:
Suresha Anepla Rajappa, Supriya Khardenavis, Aditi Samirbhai Parikh. Clinical Study of Mechanical Ocular Injuries and their Visual Outcome. Journal of Evolution of Medical and Dental Sciences 2014; Vol. 3, Issue 05, February 03; Page: 1164-1173, DOI: 10.14260/jemds/2014/1962
OBJECTIVE:
To study the distribution of ocular injuries under various parameters like place,
objects causing injuries, etiological agents, modes of presentation & visual outcome.
METHODOLOGY:
A prospective, stratified, random sampling study of eighty patients with
significant ocular trauma was done in the Department of Ophthalmology, J.J.M. Medical
College, Davangere from June 2012 to May 2013. All patients were appropriately managed
and followed up for a minimum period of three months.
RESULTS:
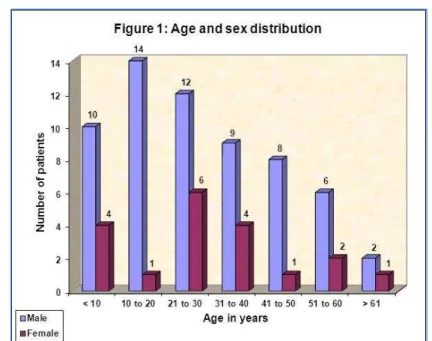
Majority of the injuries
occurred in males, accounting for 76.25% of the total. Maximum age incidence was in 21-30
years with 60% of injuries occurring within 30 years of age. Overall, agricultural injuries
accounted for 33.75%, being commonest, with 65% of patients from rural area. Majority
required hospitalization (77.5%), with 52.5% cases being open globe injuries and, 47.5%
closed globe injuries. Most common cause of injury was stick (30%), followed by stone
(20%) accounting for 50% of cases. Forty-two (52.5%) cases presented within 24 hours of
injury. Commonly involved structures in order of frequency were cornea (63.75%), lens
(50%) and, iris & pupil (45%). 57 (71.25%) cases required surgical intervention. Best
corrected visual acuity of >6/18 was achieved in 47.5% of cases.
INTERPRETATION &
CONCLUSION:
Majority of the injuries were sustained by young adults, in the most
productive period of their lives. Improvement in basic farming methods and use of protective
eye wear can reduce the incidence of eye injuries. Delayed presentation was noted in many
patients. Education & early intervention need to be stressed.
KEYWORDS: Agricultural; Open globe and Closed globe; Cornea; Iris; Pupil
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1165 clinical and investigational means. This would enable us in the management of ocular trauma so that timely intervention can prevent loss of vision and preserve the eyes.
OBJECTIVES:To study the demographic details, etiological agents causing ocular injuries, modes of presentation, extent of involvement of ocular structures, and their visual outcome.
MATERIALS & METHODS: In this hospital-based prospective stratified random sampling study, eighty patients with significant ocular trauma attending the outpatient & inpatient department of the Department of Ophthalmology attached to J.J.M. Medical College, Davangere, Karnataka between June 2012 to May 2013 were studied after obtaining ethical committee clearance.Inclusion criteria were open globe injuries and closed globe injuries. Exclusion criteria were extra ocular foreign body, corneal abrasions, adnexal injuries, orbital injuriesand non-mechanical injuries.
In every case a relevant history was taken with particular emphasis on the nature, activity at the time of injury, causative agents and time interval between injury and the time of presentation. All these details were recorded in a proforma.After general physical examination, all the patients were subjected to detailed ocular examination with torch light and slit lamp examination. Pupillary reactions, both direct and consensual, were noted in both eyes. Unaided visual acuity was determined for each eye separately. The BCVA was recorded after refraction. Detailed fundus examination was done by direct & indirect ophthalmoscope and slit lamp biomicroscopy of fundus using non-contact lens. Applanation tonometry & gonioscopy were done in relevant cases.Ultrasound B scan was done in patients presenting with hazy or opaque media to evaluate posterior segment structures and in cases where IOFB was suspected. Plain X-ray of orbit – PA and lateral views – (with limbal ring in cases with suspected radiopaque IOFB) were also obtained.
CT scan orbit was also taken in cases with unexplained visual loss and optic nerve injuries.All cases where surgical intervention was required and, cases where frequent examination was required were hospitalized. Other cases were managed and followed up on outpatient basis. Patients were referred to higher centers in cases of posterior segment involvement which could not be managed in our hospital.BCVA was recorded at the time of discharge and also at subsequent follow-ups till that stage in the patient recovery where stability is likely to have been achieved and no further improvement expected. All cases were followed up for a minimum period of 3 months.
Chi- square test was the statistical tool used to assess the results at the end of the study period.
RESULTS: A clinical study of ocular trauma and its visual outcome was conducted over a period of one year from June 2012 to May 2013. A total of eighty patients with significant ocular injury of either sex and all age groups were included. Analysis of these cases yielded the following results.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1166 Majority of cases were from rural area, accounting for 52 (65%), followed by urban, which included 19 (23.5%) patients, and semi- urban constituting 9 (11.5%) cases.Majority of cases, 62 (77.5%) required admission.
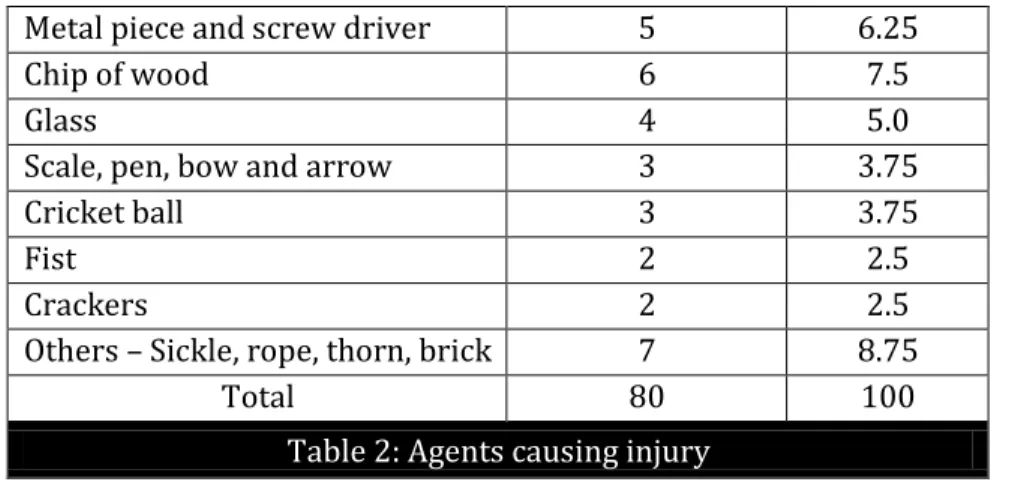
Occupational injuries (51.25%) were more common compared to non-occupational injuries (48.75%). Agricultural injuries (33.75%) were most common, followed by work place injuries (17.5%). Among non-occupational injuries, sports related injuries were highest (18.75%), followed by domestic (12.5%) (Table 1). 50% ocular injuries were caused by stick and stone put together. Animal injuries were seen in 10% cases (Table 2).
Category Number of cases Percentage
Occupational (a) Agriculture (b) Work place
27 14
33.75 17.50
Total 41 51.25
Non-occupational (a) Domestic (b) Sports
(c) Road traffic accidents (d) Other accidental injuries (e) Assault
10 15 2 8 4
12.50 18.75 2.50 10.00
5.00
Total 39 48.75
Table 1: Activity at the time of injury
Injury causing agents Number of cases Percentage
Stick 24 30
Stone 16 20
Animal injuries like bull gore,
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1167
Metal piece and screw driver 5 6.25
Chip of wood 6 7.5
Glass 4 5.0
Scale, pen, bow and arrow 3 3.75
Cricket ball 3 3.75
Fist 2 2.5
Crackers 2 2.5
Others – Sickle, rope, thorn, brick 7 8.75
Total 80 100
Table 2: Agents causing injury
Open globe injuries, 42 (52.5%), were more than closed globe injuries, 38 (47.5%). Among open globe injuries, zone II injuries were seen in 20 of 42 cases. Closed globe, zone III injuries were observed in 17 of 38 cases (Fig 2).
Majority (52.5%) presented within 24 hours of injury. Of these, 28.75% presented within 6 hours. 20% presented between 1-3 days and 18.75% after seven days. Time elapsed between injury and presentation was different in different activity at the time of injury. Among agricultural related injuries, 37.04% presented within 24 hours and 62.96% presented after 24 hours, while in work place related injuries, 85.71% presented within 24 hours and 14.28% presented after 24 hours. In sports related injuries, 46.67% presented within 24 hours and 53.33% presented after 24 hours.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1168 Maximum number of injuries were restricted to the cornea. Lens injuries followed this, constituting nearly 50% of the cases. Iris and pupil injuries closely followed making up for 36 cases.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1169
Closed globe injuries (Total: 38 cases) Open globe injuries (Total: 42 cases)
Structures affected No. of
Cases (%) Structures affected
No. of cases (%) Anterior segment
* Corneal abrasion/ edema * Lamellar laceration * Hyphaema
* Secondary glaucoma/ Angle recession
* Iridodialysis * Sphincter tears * Traumatic iritis
* Cataract/ subluxation/ dislocation of lens 6 (15.78) 7 (18.42) 9 (23.6) 2 (5.26) 1 (2.63) 13 (34.2) 6 (15.78) 17 (44.65) Anterior segment
* Self sealed corneal tears * Corneal tears
* Scleral tears/ Cornea-scleral tears
* Iridiocyclitis * Iris prolapse * Hyphaema * Iridodialysis *Cataract/Subluxation/dislocation of lens 4 (9.5) 16 (38.09) 14 (33.25) 3 (7.15) 13 (30.9) 6 (7.5) 1 (2.3) 18 (42.84) Posterior segment
* Vitreous hemorrhage * Endophthalmitis
* Retinal edema/ hemorrhages * Choroidal rupture
* Optic neuropathy
7 (18.42) 1 (2.63) 8 (21.05) 4 (10.52) 2 (5.26) Posterior segment
* Retinal detachment * Vitreous prolapse * Badly ruptured globe * Infection * IOFB 1 (2.3) 3 (7.15) 5 (11.9) 3 (7.15) 3 (7.14) Table 3: Showing structural effects of ocular injury
Fifty-seven (71.25%) patients required surgical management and 23 (28.75%) were treated by conservative methods.
Final visual outcome was assessed. 38 (47.5%) patients had visual acuity > 6/18, 15 (18.75%) had visual acuity between 6/24 to 6/60, 8 (10%) had visual acuity < 6/60, 6 (7.5%) had only perception of light and 3 (3.75%) had total blindness, while visual outcome could not be assessed in 4 (5%) cases as they were lost for follow up. Six (7.5%) eyes were enucleated. Visual outcomes were analyzed for different activities. 57.14% of work place and 53.33% of sports injuries had visual acuity of > 6/18, while 44.5% of agricultural related injuries had visual acuity of > 6/18. Two eyes each in agricultural and work related injuries underwent enucleation. No eye required enucleation in sports and domestic injuries. There was no significant difference in visual outcome in different groups ( 2 = 1.15, df = 4, p = > 0.05).
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1170
Vision Open globe injuries [No. (%) of cases] Closed globe injuries [No. (%) of cases] Zone I Zone II Zone III Zone I Zone II Zone III
> 6/18 9 (21.42%) 6 (14.28%) - 9 (23.68%) 9 (23.68%) 5 (13.17%)
6/24 to 6/60 3 (7.14%) 8 (19.08%) 1 (2.38%) - 2 (5.26%) 1 (2.63%)
< 6/60 - 3 (7.14%) 1 (2.38%) - 1 (2.63%) 3 (7.89%)
PL +ve - 2 (4.76%) - - - 4 (10.52%)
PL –ve - 1 (2.38%) 1 (2.38%) - - 1 (2.63%)
Unknown - - 2 (4.76%) - 1 (2.63%) 1 (2.63%)
Enucleated - - 5 (11.9%) - - 1 (2.63%)
Total 12 (28.56%) 20 (47.64%) 10 (23.8%) 9 (23.68%) 13 (34.2%) 16 (42.12%)
Table 4: Visual outcome in different types of ocular injuries
DISCUSSION: Ocular injuries are one of the leading causes of monocular blindness and visual impairment worldwide.3 In developing countries, eye injuries are not only more common but also more severe in their effects. Since eye injuries are related to particular occupations or cultural environments, the type and prognosis of injuries seen in developing countries are not similar to those in industrialized countries.4
Eighty cases of ocular injuries were studied in detail and critically analyzed from June 2012 to May 2013. Age of the patients in the present study varied from 3 to 80 years. Nearly 60% were under 30 years of age. There were more number of cases in this age group in the present study as compared to other studies. In a study done by Mukherjee et al.5, there were 44.91% cases less than 30 years of age as compared to 58.7% in the same age group in this study. Commonest age group was between 21 and 30 years (22.5%). The study Mathen MM6 reported 33% patients between 20 and 30 years of age. Thus there is a great deal of concordance between the present study and the above mentioned studies. Males were affected more often than females across all age groups, with an overall male: female ratio of 3.2:1 (76.25%:23.75%). Macewen7 reported 87% incidence in males.
Most patients were from rural areas (65%) as compared to patients from urban (23.5%) and semi-urban areas (11.5%). However the study by Banait et al.8 did not find any difference between urban, rural and urban slum population in the incidence of ocular injury. This difference could be due to inclusion of minor ocular injuries in the latter study. Inpatient care was required for 77.5% patients while 22.5% were treated on outpatient basis. The study by Macewen7 reported that 98.2% were treated as outpatients. This gross difference could be because majority in their sample had involvement of periorbital and superficial structures only, whereas the present study included significant ocular injuries.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1171 majority of patients were from rural areas. Krishnan et al.9 reported stick (40.31%) as the most common offending agent, followed by stone (19.37%), in penetrating injuries. Stick was also the commonest means of injury (23.37%) followed by bull gore injuries (18.18%), in blunt trauma. This is in agreement with our study.
In the present study 52.5% of patients presented within 24 hours of injury and 28.75% presented between 2-7 days. Mathen et al.6 found that 40% presented within 24 hours and 41% between 2-7 days. Most patients in the present study had poor vision at presentation. 72.5% had visual acuity worse than 6/60. This was due to involvement of cornea in 63.75% cases, lens in 50% and, iris & pupil in 45% cases. Posterior segment structures like retina (17.5%) and vitreous (15%) were involved in few cases. This is in agreement with many previous studies.7-11
In the present study, among closed globe injuries, lenticular involvement (44.65%) like cataract and subluxation was most common, followed by hyphaema (23.6%), corneal lamellar laceration (18.42%), retinal and vitreous involvement (39.47%). The study by Krishnan and Srinivasan9 showed subluxation of lens in 38.96%, hyphaema in 27.27%, cataract in 15%, macular edema and hemorrhage in 16% and posterior segment involvement in 20.7%. This is in agreement with the present study.In the present study, among open globe injuries, corneal tears (47.59%) were commonest, followed by lenticular involvement (42.84%), iris prolapse (30.9%), corneo-scleral tears (26.1%) and posterior segment involvement (20.27%). Mukherjee et al.5 reported corneal perforation in 62%, corneo-scleral tears in 29.26%, posterior segment damage in 34.1%, which is similar to our study. Three cases (7.15%) developed infection and three (7.14%) presented with intraocular foreign body. Saini et al.12 reported a 14% incidence of infection. In the present study, 71.25% required surgical intervention against 28.75% requiring conservative management. In the present study, 47.5% had BCVA > 6/18 at the end of three months and 17.5% had < 6/60 (PL +ve to < 6/60). Ten eyes (11.25%) ended with total loss of vision, out of which 5 eyes were enucleated due to badly ruptured globe and one eviscerated due to endophthalmitis.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1172 injuries required enucleation (n = 5). Zone-I closed globe injuries had best visual outcome since all cases had visual acuity >6/18.
Ocular trauma occurs frequently in developing countries and constitutes a major health problem. After considering the frequency, causes, nature, consequences and final visual outcome, any ocular injury, however trivial, must be considered as an ophthalmic emergency and adequately dealt by exercising utmost care, caution and speed to salvage whatever possible in terms of structure and function of the eye.
REFERENCES:
1. Albert DM, Jakobiec FA. Principles and practice of ophthalmology. 2nd edition. Philadelphia: WB Saunders Company 2000; 6:5179-277.
2. Duke-Elder S, MacFaul PA. Mechanical injuries part I in injuries in system of ophthalmology. Vol. XIV. Duke Elder S (editor). London: Henry Kimpton; 1972.
3. Vasu U, Vasnaik A, Battu RR, Kurian M, Georg S. Occupational open globe injuries. Indian J Ophthalmol 2001; 49(I):43-47.
4. Negral A. Magnitude of eye injuries worldwide. Community eye health. 1997; 10(24):49-53. 5. Mukherjee AK, Saini JS, Darbal SM. A profile of penetrating eye injuries. Indian J Ophthalmol
1984; 32:269-71.
6. Mathen MM, Prajna NV, Srinivasan M. Ocular trauma South Indian profile ocular trauma – the South Indian profile. AIOC Proceedings; 2003.
7. Macewen CJ. Eye injuries: A prospective survey of 5671 cases. Br J Ophthalmol 1989; 73:888-94. 8. Banaith S, Venkataraman VR, Shukla AK, Smitha S, Tyagi NK, Pandith M et al. Epidemiology and
clinical profile of ocular injuries in a rural district hospital. AIOC Proceedings; 1999.
9. Krishnan MM, Srinivasan R. Ocular injuries in union territory of Pondicherry – visual outcome. Indian J Ophthalmol 1988; 36:86-7.
10.Jain BS and Soni Sr. Ocular injuries: An analytical study in a teaching general hospital. Indian J Ophthalmol 1987; 35(3).
11.Koval R, Teller J, Belkin M, Romen M, Yanko L, Savir H. The Israeli ocular injuries study. Arch Ophthalmol 1988; 106.
12.Saini JS, Mukherjee AK, Dabral SM, Moraes O. A profile of penetrating eye injuries. Indian J Ophthalmol 1985; 33:95-7.
Journal of Evolution of Medical and Dental Sciences/ Volume 3/ Issue 05/February 03, 2014 Page 1173
AUTHORS:
1. Suresha Anepla Rajappa 2. Supriya Khardenavis 3. Aditi Samirbhai Parikh
PARTICULARS OF CONTRIBUTORS:
1. Associate Professor, Department of Ophthalmology, J.J.M. Medical College, Davangere.
2. Postgraduate Student, Department of Ophthalmology, J.J.M. Medical College, Davangere.
3. Postgraduate Student, Department of Ophthalmology, J.J.M. Medical College, Davangere.
NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR:
Suresha Anepla Rajappa, Associate Professor,
Department of Ophthalmology, J.J.M. Medical College,
Davangere- 577004, Karnataka. E-mail: [email protected]