executivecommitteeof
workingparty of
the direc
ti
ng council
the regional committee
:_
I_1
PAN
AMERICAN
_'
IV//
HEALTH
HEALTH
WOR
L
,
'
t'
°_
_'°_*_
/
ORGANIZATION
ORGANIZATION
118th Meeling
Washington,
D.C.
June
1996
Provisional Agenda Item 4
.
9
CE118
/
17
(Eng.)
15 April 1996
ORIGINAL: SPANISH
ACQUII_Er_
IMMUNOD_C_CY
SYNDROME
(AMS)
IN _
AMERICAS
The
do
c
ument
reviews the situation
of the HIV
/
AIDS
/
STD
epidemic
in the
Region and
briefly
reports on
the status
of the
United Nations
Joint
Program on
tilV
/
_S
(UNAIDS),
as well as
the development of national
programs on AIDS
in
Latin Ameri
c
a and
the Caribbean over
the last 12 years.
Despite major efforts, it was
not possible to have a fully operational joint
program at the world level by
January 1996, as envisaged in the original
plan.
In
the Americas PAHO
has continued
to
provide crucial support for
the
establishment of UNAIDS
and has promoted,
the creation of interagency
Theme
Groups on AIDS in
all the countries.
These Groups
,
which will be
responsible for
improving collaboration between the various agencies, are endeavoring to enlist
greater
multisectoral
support for
the
national
response
in
each country to
the
challenge of AIDS.
The Executive
Committee is
asked for guidance on the suitability of
the
proposed approach
as
a basis for continued technical coope
r
ation with
the Member
CE
l
1
8
/
1
7 (F
a
g.)
P
a
ge2
CONTENTS
Page
Exe
c
utive Summary
...
3
1.
Introduction
...
4
2.
Review of the Situation
...
5
3.
Development of
Progrmnming
for
the Prevention of
AIDS
/
HIV
/
STD
in
the
Region of
the Americas
...
5
4.
The Joint
United Nations Program
on
HIV
/
AIDS:
Challenges
for
Its
Implementation
in the Region
of
the Americas
...
7
5
.
The Regional Program and PAHO
Technical
C
ooperation
within the
UNAIDS Framework
...
8
Annexes
A.
AIDS Surveillance
in
the Americas
B.
Development
of
the
National
Programs
C.
List of
Prevention Indicators
(PI)
CmlS
/
l?
(
E
n
g.
)
g
e
3
EXECUTIVE
SUMMARY
Four United Nations agencies (UNDP, UNICEF, UNFPA
,
UNB
S
CO
f
and the
World Bank
have
joined forces
with
the World Health Organization to establish the
J
o
int
United
Nati
o
ns Program
o
n
HIV
/
AID$
(UNAIDS).
The
t
r
ansition fr
o
m the WHO
Global
Program
on
AIDS to UNAIDS resulted in a sharp
reducti
o
n in technical
c
oo
peration f
o
r
AIDS prevention in
the
Americas at a time
when
the epidemic
is
surging
ahead on its
unrelenting
course thr
o
ughout the
world.
At the beginning
of 1995,
in preparation for
the full-scale startup
of
UNAIDS
in
January
1996
,
the
PAHO Regional Program
on
AIDS
/
STD drafted
a
Regional
Plan of
Action for 1996-1999, which was reviewed and endorsed by the Directing Council
of
PAHO in
September 1995.
Despite severe budgetary
cutbacks, the
Organization
decided t
o
maintain
its
Regi
o
nal
Pr
o
gram on AIDS
/
STD
and mandated it t
o
carry on
with its activities
in
technical and scientific areas
for the prevention of
AIDS and the
control of human
immunodeficiency
virus (HIV) and sexually transmitted
diseases (STD) within the
interagency and multisectoral framework
of UNAIDS, and at the
same time
to
continue
its technical support
of national programs
on AIDS prevention in the
Region.
Given
the unpostponable
need to m
o
bilize
the human
,
financial
,
and p
o
litical
resources that
are
needed
to shore up national
responses in the
countries
o
f
the Regi
o
n
,
it is
critically important that
the
Executive C
o
mmittee
c
o
nsider appr
o
priate mechanisms
within the framew
o
rk
of interagen
c
y a
n
d
intersect
o
ral
c
o
llab
o
rati
o
n s
o
that techni
c
al
cooperation
on HIV
/
AIDS
prevention and
c
o
ntr
o
l will
n
o
t be subject t
o
delays
o
r
interruptions
which might result
in an
upsurge
of the epidemic
and its
consequences
,
and
that
the Committee
provide the Secretariat
with proposals
and
orientati
o
n in this
regard.
CEl18
/
17
(Eng.)
Page 4
1.
Introduction
In an effort to achieve greater interse
c
toral involvement
in the
global campaign
against AIDS, four United Nations agen
c
ies
(UNDP, UNESCO,
UNICEF, and UNFPA)
and the World Bank have joined forces with the World Health Organization to establish
the
Joint United Nations Program on HIV
/
AIDS
(UNAIDS),
which officially
began
operations
in
De
c
ember 1994 with the sele
c
tion and appointment of Dr. Peter Piot as its
Executive Dire
c
tor.
In
1995
UNAI
D
S
held
several
consultations at the
regional
and
c
ountry level aimed at defining its stru
c
ture and operations more
pre
c
isely,
and it also
prepared a budget for the 1996-1997
biennium and a strate
g
ic plan for the next five
years.
Despite these efforts, it was not possible for the Joint United Nations Program on
HI
/
AIDS
to
be
fully operational at the world level by
January 1996, as envisa
g
ed in
the original
plan.
Among other factors, the transition from the WHO Global
Program
on AIDS
(GPA) to UNAIDS
required the
Exe
c
utive Dire
c
tor to give almost his
full
attention to enlisting
political support and mobilizin
g
resources,
an
effort
which
culminated in
the
approval in
November
1995 of a proposed budget of USS 120 million
for the 1996-1997
biennium.
At the same time, UNAIDS
conducted
ne
g
otiations to
enlist the cooperation of various agen
c
ies,
including WHO Headquarters
and its
regional
offices, on spe
c
ific areas of collaboration,
taking
into account their
respe
c
tive strengths.
The sudden loss of more
than
200 experienced
GPA
staff members
from WHO
Headquarters
in
Geneva, the
regional offices,
and the
countries when their
c
ontracts
expired in 1995 or early 1996, followed
by unavoidable delays
in
the recruitment of a
new, mu
c
h smaller staff for UNAIDS,
made for a notable decrease
in
te
c
hnical
cooperation for AIDS prevention--while
at the same time
the
epidemic
continued to
advance at its
unrelenting pace
throughout the
world.
C
E118
/
17
(Eng.)
Pa
g
e
5
2.
Review of the
Situation
As
of
10 De
c
ember
199
5,
a
cumulative total of 6
5
9
,
662
c
ases of AIDS in the
Ameri
c
as, with 388,633 asso
c
iated deaths, had been reported
to the Pan Ameri
c
an Health
Organization.
However, it is estimated
that the tree cumulative number of persons with
AIDS in the Region may
be
at least double
that figure.
In addition, it is
believed
that
the number of HIV-infe
c
ted
men, women,
and
c
hildren in reality stands at 2.5
to
3 million.
Although there
have been signifi
c
ant advan
c
es
c
ontributing to the reduction of
HIV
/
AIDS
transmission, espe
c
ially through blood, the
number of persons infe
c
ted
with
and dying from AIDS
c
ontinues to increase throughout the world.
It is estimated
that
between
6
,
000 and 10
,
000 new
infections
occur
each
da
y
,
60%
to
70%
of
them
in the
least
industrialized countries.
The data available on the epidemic
in Latin Ameri
c
a and
the
Caribbean
show a
general rising
trend
in
infe
c
tions
among
the heterosexual
population,
which particularly affects women and adolescents and, within these groups,
especially those in
the
e
c
onomically weakest sectors
of so
c
iety.
In addition, the infection
is beginning to be seen
in
rural
and marginal
urban
communities.
In many
c
ountries
AIDS is already one of the
five leading
causes of death
in
the population aged
25
to
44
years.
Annex
A
gives up-to-date
information on reported
cases of AIDS
in
the
Region.
It is estimated
that
each year there
are
between
40
and
50 million new
cases of
STD
in
the
Region
of the Americas.
The
trends
in
the data
from Latin America and the
Caribbean
vary fr
o
m country to country.
While the
incidence of gonorrhea
declined
between
1987 and 1993, in 1
2
countries the incidence of primary,
secondary, and
congenital syphilis increased.
The annual incidence of the congenital form of the disease
is estimated at 250,000 cases. In addition, it is
distressing to note that every year
some
24,000 women in the Region die of cer
v
ical cancer, which is produced
by the
sexually
transmitted human papilloma virus. Given the major deficiencies
in
the surveillance and
reporting
of
STD, it is more than likely that the foregoing
figures
are
greatly
underestimated,
and they should therefore be analyzed with caution.
The fact that the
true figures are so much greater should be ample reason to step up the efforts
that have
been made so far.
3.
Development
of Programming
for the Prevention
of AIDS
/
HIV
/
STD
in
the
Region of the Americas
In the
early
1980s the
public
health sector
was the
first area t
o
feel the impact
o
f
the HIV
/
AIDS
epidemic.
A
cco
rdingly
,
the
first f
o
rmal
prog
r
amming
resp
o
nses t
o
.CI_118
/
17 (Fag.)
Page 6
1988
be
c
ame the primary axis
around which
the
other
se
c
tors
of
so
c
iety--by then alerted
and
committed
to addressing
the
c
hallenge
of AIDS--were
mobilized.
Gradual
re
c
ognition of the growing impa
c
t of AIDS on other areas of individual and
community
life led
to the organization of interse
c
toral
and multise
c
toral
c
ommissions to orchestrate
various initiatives of so
c
iety
as a whole.
In a number of
c
ases
the role played
by these
c
ommissions was more symboli
c
than functional.
As a result, with
few exceptions, the
health se
c
tor
c
ontinued to
c
oordinate the responses of the various other se
c
tors to the
HIV
/
AIDS
epidemi
c
--sometimes
without even
volunteering
for this
responsibility.
Spe
c
ial
note should
be made
of the
outstanding
work
done
by
some
of the
nongovernmental organizations
(NOOs), which in many
cases pre
c
eded
and stimulated
the
responses of governments to the
emerging problem of AIDS.
Thus, it is the health sector programs---even those criticized for
being partial to
the public sector, adopting excessively
medicali?ed
approaches,
or supposedly
being
unable to address the
social implications of the epidemic--that
continue to be the tangible
presence
of the
national response to the
HIV
/
AIDS epidemic.
Moreover, it is the health
sector programs that are responsible for collecting,
analyzing,
and disseminating
the
epidemiological
,
technical, and scientific information
that the other sectors need in any
country in order to act
usefully and effectively.
It is not without reason that the health
sector programs are universally known as the "national AIDS programs."
Even allowing
for their weaknesses due to such factors as frequent changes in leadership, shortage of
financial resources, and lack of official status, at the country level the national AIDS
programs are performing a number of functions that no other agency or entity is in a
position to carry out. Although all sectors of society can become involved in health care
activities,
the primary
responsibility continues to fall on the health sector
,
which is
expected,
in addition,
to standardize and regulate the responses of the entire community.
Even UNAIDS--which,
like PAl-lO, assumes that the national response to AIDS should
be multisectoral--does
not propose to duplicate the coordination
and leadership role being
performed
by the national programs.
However,
most of the financing
agencies,
e_
w
.
c
ially the bilateral agencies, in their concern
to promote greater involvement of the
private sector and civil society, represented mainly by NGOs, are concentrating
their
international support almost
exclusively on nongovernmental
sectors. Thus, the national
programs, established with such great effort by the Member States with support from
PAHO and WHO's Global Program on AIDS, have seen a sharp decline in international
financing, which has reduced their operating capacity and, ironically, their capacity to
mobilize
resources
and articulate
efforts at the national level.
CBll8
/
17
(Eng.)
rase7
already being
validated
in
five
c
ountries of the Region.
Soon it will be possible to show,
to a greater or lesser degree, whether or not
the work done so far toward
the prevention
of HIV
/
AIDS
has a
c
tually borne fruit. For
the information of the Exe
c
utive
Committee,
Annex B provides a brief
chronology of the national programs andAnnex C summarizes
the prevention
indicators
that have been developed by
the
GPA.
4.
The
Joint
United
Nations
Program
on HIV
/
AIDS:
Challenges
for Its
Implementation
in the
Region of the
Americas
The establishment
of Theme
Gr
o
ups on AIDS in
the Latin
American
and
Caribbean countries
reflects
the basic
UNAIDS
concept of participation by its six
cosponsoring agencies, except in the smaller countries of
the English-speaking Caribbean
where not
many of the agencies are represented.
The specific details of how each of
these Groups will operate in
their
respective countries are being
refined at
the national
level,
and this exercise is currently in progress.
Some of
the
questions
that
remain to
be worked out have to do with
the
mechanisms for
mobilizing and channeling resources;
interaction
between the Theme
Gr
o
up and
the national program, the NGOs
,
and the
various actors
involved in the
national response to AIDS; interagency
communication;
location of the headquarters
in each case;
and, especially
,
the most efficient
and
appropriate
mechanisms for providing technical cooperation to
the countries.
Annex D
lists the main activities
being carried
out by UNAID
S
through the Theme Groups
in
the
countries, which consist for the
most part of technical direction on the part of PAHO.
As a complement to this effort,
UNAIDS
/
Geneva,
through its Department of
Country Support
,
is attempting to determine the best way to take advantage of its own
resources
and those
of the agencies
,
and it is developing
monitoring
and follow-up
capacity with global
,
regional
,
and subregional
focus.
Among the steps it
has taken
,
UNAIDS
has extended
the contracts of four of the
seven PAHO
intercountry
AIDS
advisers for
another six
months so that the technical capability developed in recent years
will
not
disappear completely.
Dire
c
t UNAIDS
financial
support to
the
c
ountries
($2.5
million
in
1996-1997)
has been reduced
to 42%
of the financing level approved
by
the WHO Global Program on AIDS for the 1994-1995 biennium
andto one-fourth of the
amount
made available to the
countries
in
1992-1993
($5.9
and $10.7
million,
respectively).
CEl18
/
17
(Fag.)
Page 8
Like any incipient program,
UNAIDS
has its
limitations.
Its organizational
stru
c
ture
is still meager and not fully
developed, and
the same
c
an be said of its
te
c
hnical
c
apa
c
ity
and its ability
to mobilize
financial resour
c
es vis-a-vis the high expe
c
tations of
the international
c
ommunity
and
the needs of the Member
States.
UNAIDS
is also
undermined by a
c
limate of resignation, skepticism, and discouragement
among
AIDS
veterans,
and by impatien
c
e
and
/
or
inexperience
on the part of some of the
newer
members.
The combination of aH these fa
c
tors gives it a very small margin for error.
On the
other hand,
there is no
denying the
implicit strength
of a
p
ro
gram
that
has
inherited a fund of
experience and knowledge
gathered f
ro
m aH parts of the
world over
the
past 10
years.
At the
same
time
,
UNAIDS
has an official mandate
to bring together
and ufili?e
the
diversified
multiagency
synergy afforded
by the United Nations and the
other major players and
enlist it for the
prevention of AIDS
at the global, regional, and
country level. The
opportunity that is available through
UNAIDS should not be
wasted.
The success
of
UNAIDS will be not only the
success of a new and independent United
Nations
program on AIDS
but also that of a joint
,
innovative, and synergistic
effort of
governments
,
NGOs,
agencies, sectors,
and institutions
to address a public
health
problem that has an impact on aH areas of life
and human endeavor.
5.
The Regional Program and PAHO Technical Cooperation
within the UNAIDS
Framework
At the beginning
of
1995, in preparation
for
the full-scale startup of
UNAIDS
in
January
1996,
the PAHO
Regional
Program
on
AIDS
/
STD
drafted
a
Regional
Plan
of
Action for 1996-1999, which was reviewed and endorsed by the Directing Council of
PAHO in
September
1995.
This Plan forms part of the Organization's
institutional
response
to the mandate given by the heads of state
and government of the countries of
the Western Hemisphere
at the
Summit of the Americas (Miami, December
1994),
according to which
PAHO was called upon to develop a program to combat endemic and
communicable diseases, as well as a program to prevent the spread of
HIV
/
AIDS,
and
to identify
sources of funding.
This Plan
proposes to fulfill the following objectives:
1.
Support the multisectoral response to the
epidemic, as promoted
by UNAIDS, by
strengthening the
capacity of the health sector.
¢mls
n
7 (E
n
g
.
)
Page 9
3.
Develop
effective, Region-specific interventions, including
evaluation procedures,
that
are
in
keeping
with the local public health situation
and the resources
available in the Member States.
4.
Expand the
response
of
the
health
sector through the
delivery of appropriate
HIV
/
STD
prevention and
c
are servi
c
es, seeking to
integrate them at all
levels of
the health
system.
5.
Increase the impact of
STD prevention
and care programs
at all levels of
the
health system with a view to reducing
the sequelae of STD
and
their
c
ontribution
to the spread of ttlV.
Even though its team has been greatly reduced
in
size, PAHO has
c
ontinued
to
support the
countries through
technical cooperation.
It
has con
c
entrated its a
c
tions in
specific areas
of training in management,
epidemiological
surveillance, education, and
development
of programming for the distribution
of condoms, in
c
luding access
thereto,
at the regional and subregional
levels.
In carrying
out this
work it has
mobilized
consultants
and, when requested, experts in
s
pecific
subject areas.
In 1996 and 1997
PAHO will continue its efforts to
mobili
z
e
resources and strengthen
the
re
s
ponse
capacity
of the Region, and it will also
promote greater interprogrmn cooperation through
other
technical programs and units
of the Organization--for
example, Communicable
Diseases;
Health
Situation Analysis;
Women, Health, and Development;
Maternal and Child
Health; External Relations; Legal Affairs; and Public Information--and
with the
staff
of
these programs in the countries.
In addition, it has reached agreements for te
c
hni
c
al
coope
ra
tion and financing for the
English-speaking Caribbean (through CAREC) with the
German and French technical cooperation agencies and with
Spain
for Central America
and the Andean area. In addition, there have been preliminary negotiations
with CIDA,
the
Netherlands,
and the
Nordic countries aimed at securing the relevant financial
support
for the governments
of the Region.
At this critical
time
of transition toward a new form
of interagency and
intersectoral
collaboration,
it is fundamental that the existing scientific and te
c
hnical
capacity and the focus
of the earlier AIDS programs are
not lost, and,
e_ecially,
that
advantage is
taken of the experience accumulated at the national level.
This should be
done, whenever possible, by promoting greater cooperation between governments
as part
of the world and regional effort for the prevention
of I-IIV
/
AIDS.
CBl18
/
17
(Fag.)
Page 10
program
will
c
on
c
entrate
in the immediate
future
on
the
provision
of
te
c
hnical
c
ooperation for strengthening the health
se
c
tor.
Its
principal
counterparts in this
task,
although not the only ones, will be--as they have been up to now--the
national AIDS
programs
in the
countries of the Region.
Its
sphere
of action, however,
should
go
beyond
the s
c
ope of a single
institution; it is important to promote the active participation
of NOOs,
bilateral and unilateral agen
c
ies,
and se
c
tors
and
institutions at the
country
level to back up the work of UNAIDS.
Finally,
in
order to promote an
interagency response, given the
limitation of its
own
resour
c
es, UNAIDS
suggests that WHO,
and by extension PAHO,
confmes its
a
c
tivities
to traditional
health
areas--for
example,
laboratory,
epidemiologi
c
al
surveillan
c
e, training
of physi
c
ians
and nurses.
However,
since its
inception the
Regional
Program on AIDS
/
STD
has known
how to successfully
enhance national
response
c
apacity through the
establishment of ties
and
collaboration with other se
c
tors
(e.g.,
NGOs,
education,
law, the private
sector, the armed
for
c
es,
religious
and
c
ommunity
groups).
Several of
the
bilateral donors have asked
PAHO to
continue to
pursue this line of
integrative a
c
tion within the
UNAIDS framework,
allowing
time for
other agen
c
ies to gradually assume functions that are
complementary to the
health se
c
tor
as part of
the effort to
c
ombat AI
D
S.
The Secretariat is
currently fa
c
ing
the question of
whether it will be limited
to Obje
c
tives
4 and
5
of the Plan of Action, as suggested by
UNAI
D
S, or
continue to also address Objectives
1, 2,
and 3 of the Plan (see pages
8 and
9), depending
on the decision
reached by the Governing Bodies of PAHO,
in regard to
which it is requesting
the orientation of the Executive Committee.
CB
l18
/
1
7
(
E
ng
.)
A
n
ne
x A
,
PAHO/HCA/96
.
004
AI
D
S S
U
RVEI
L
LANCE IN THE AMERICAS
II
Oo °
QUARTERLYREPO
RT
10 March 199
6
k,
REGIONAL
P
ROGRAM
ON AIDS
/
STD
Divi
s
ion
of Di
s
ea
s
e Prevention
and Control
!__
,(
_
Pan American
Health Organization
/
,
_
_
'
_
TABLE OF CONTENTS
I
.
R
e
gi
on
al Pr
og
r
am
o
n A
IDS
/
S
TD
-
Funct
i
on
I
I.
AID
S S
urve
i
llance
i
n the Ame
ri
cas
(10
Marc
h 1
99
6)
-
S
ummary of the Surve
il
l
an
ce
System and
th
e Epidemic.
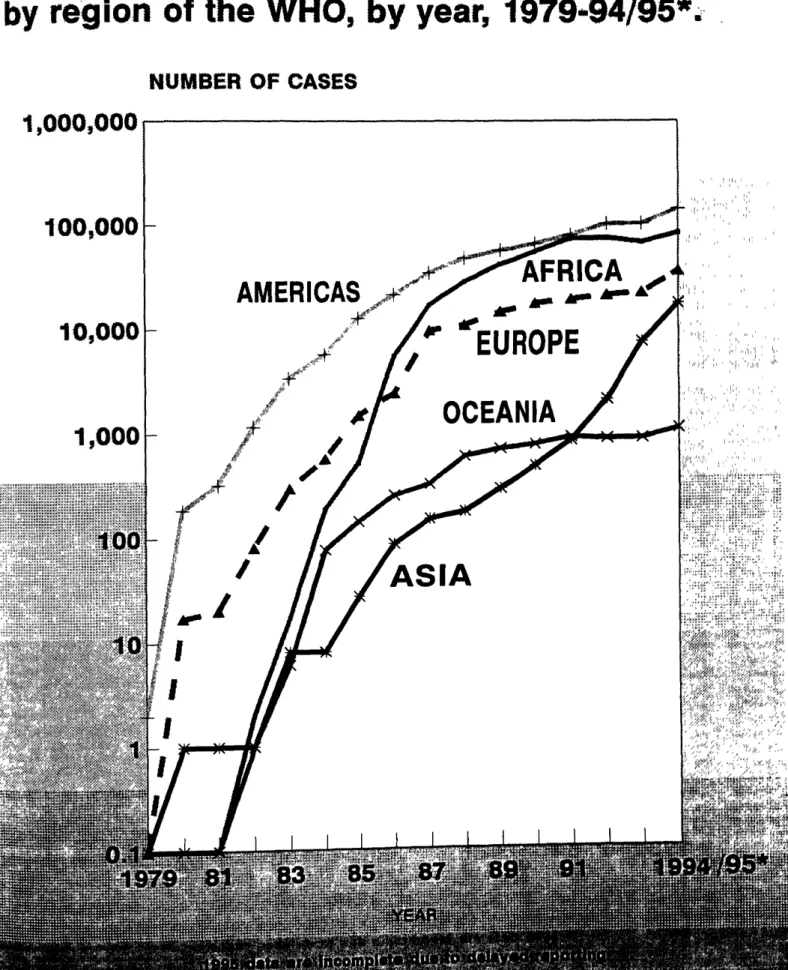
Fig. 1.
Annual incidence of AIDS cases, by WHO region, by y
e
ar, 1979
-199
4
-
9
5
Fig. 2.
Annual incidence rates of
A
IDS in
th
e Americas
(
per million
)
,
thre
e
subregions,
1
98
2
-
199
5
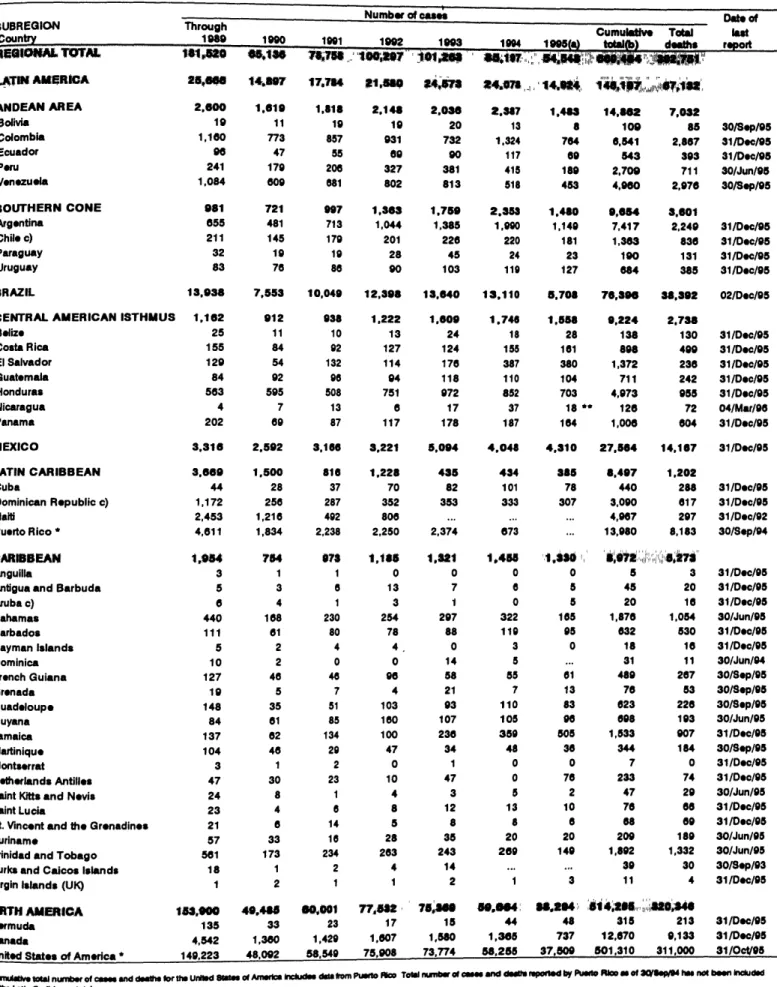
Table
1
.
Number of
re
ported c
as
es of AIDS by year, and c
um
ulative c
as
es and
dea
th
s, by countr
y
and subregion
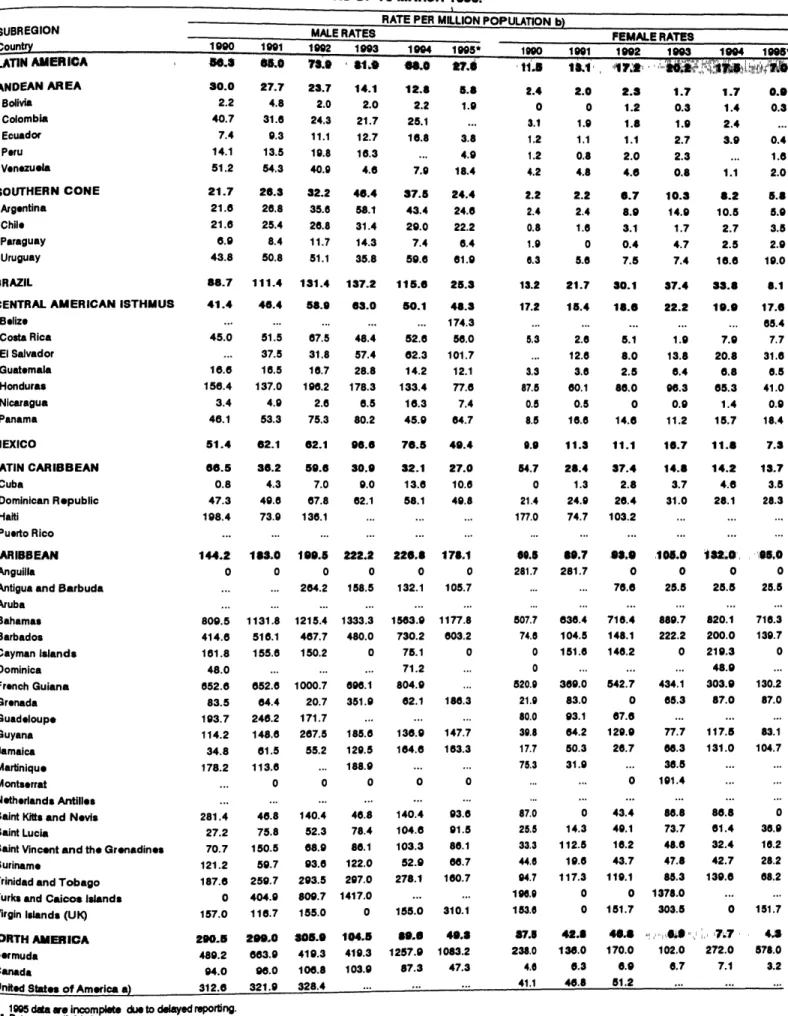
Table 2.
Annual incidence rates of
AI
DS
(
per million population), by country
and by year,
1
990
-
199
5
Table
3
.
Annual in
c
iden
c
e rate of
AI
DS
(
per million population), by sex, by
c
o
un
try and
b
y y
e
ar, 1990-19
9
5
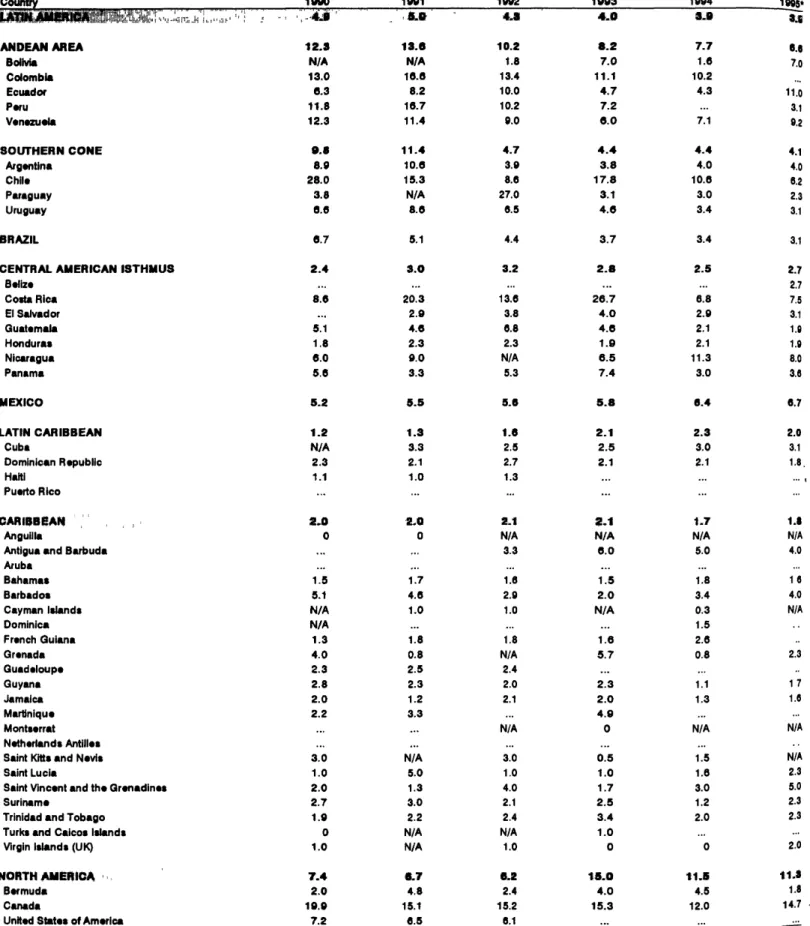
Table 4.
Male:Female rati
o o
f rep
o
rted AIDS cases, by c
o
unt
r
y and by year,
199
0
-1995
Table 5.
T
o
tal ca
s
es, pediatric cases, percent
o
f pediatric cases fr
o
m t
ot
al,
perinata
l c
as
e
s, and pe
rce
nt
o
f p
e
ri
n
ata
l c
a
ses
fr
om
t
o
tal p
e
d
i
atri
c
, by
s
ubregi
o
n and c
o
untr
y
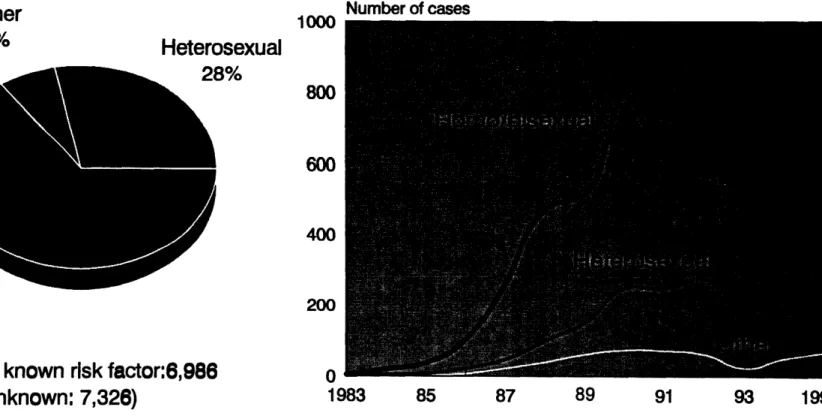
Fig. 3a.
Distributi
o
n
o
f AIDS
c
as
e
s by risk fact
o
rs, And
e
an Ar
e
a
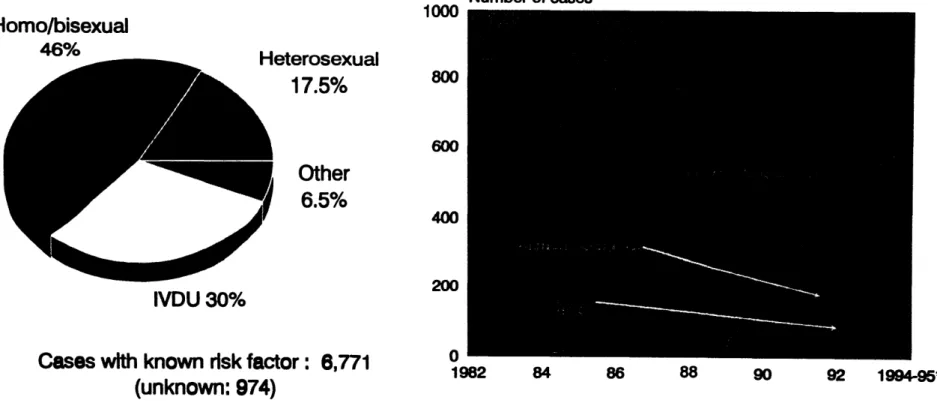
Fig. 3b.
Distributi
o
n
o
f AIDS
c
as
e
s by risk fact
o
rs, S
o
uth
e
rn C
o
n
e
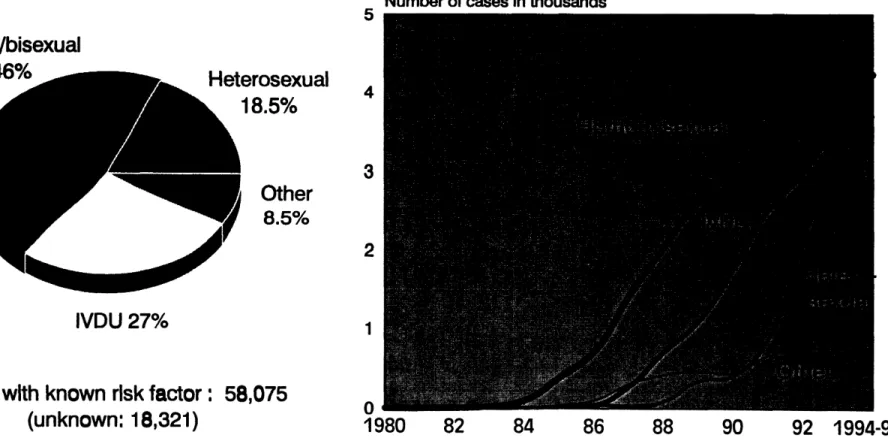
Fig. 3c.
Distributi
o
n
o
f AIDS cas
e
s by risk fact
o
rs, Brazil
Fig. 3d.
Distributi
o
n
o
f AIDS cases by risk fact
o
rs, C
e
ntral Am
e
rican I
s
thmu
s
Fig. 3e.
Distributi
o
n
o
f AIDS ca
s
e
s by risk fact
o
rs, M
e
xic
o
Fig. 3f.
Distributi
o
n
o
f AIDS cas
e
s by risk fact
o
rs,
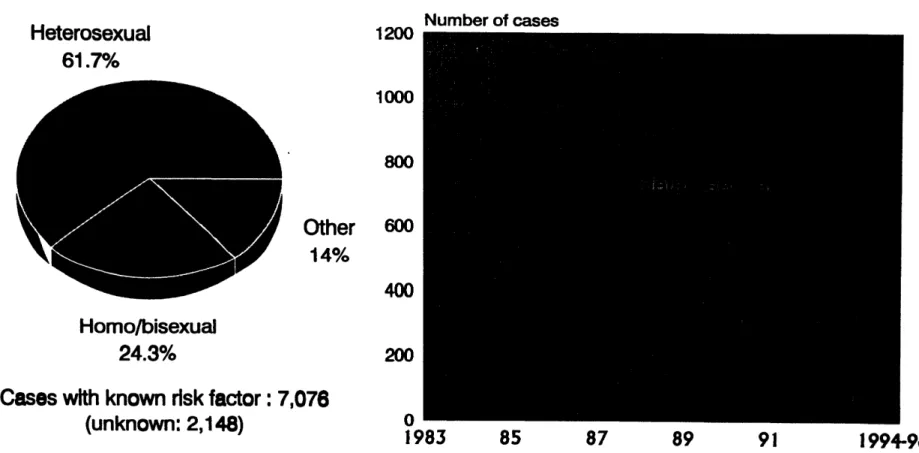
C
aribb
e
an
I. The Re_onai
Pro_
,
am
on
A
IDS
/
STD
The Reg
i
onal Program on AID
S
/
S
TD of the D
i
v
i
s
i
on of Disease Preven
ti
on and
C
ontr
o
l of the PanAmerican Health
O
rganization
(
PAH
O)
provides technical collaboration
an
d
e
xpert
i
s
e
for
the
pre
ve
ntio
n
and control o
f
HIV
/
AIDS and o
the
r s
ex
ua
lly
transm
i
tted d
i
s
ease
s
in the Region of
th
e Ameri
cas
.
Th
e mandate for PAHO
'
s Re
g
ional Program on AIDS
/
STD
is
to promote, design and fa
c
ilit
a
te te
c
hni
c
al a
c
tivities and poli
c
ies to improve the
c
apa
c
ity of
Member
Countries to reduce the number of futur
e
infections and to provide timely
an
d
adequate
c
are for people livin
g
wi
th
HIV
/
AIDS and STD.
T
he Regional Program is part of a broader set of culturally
-
sensitive,
g
ender
-
spe
c
i
fic
,
multinational
and multi
s
ectoral responses to H
I
V
/
AI
DS
an
d STD in the Ameri
c
as.
Th
e
followin
g
types of te
c
hni
c
al
as
sistan
c
e provide a fr
am
ework
for
th
e Pro
g
ram
'
s myriad
a
c
tivities:
·
dissemination of information
·
trainin
g
·
dire
c
t te
c
hnical
c
ooperation
·
resour
c
e mobilization
Th
e Re
g
ional Pro
gr
am on A
I
DS
/
S
TD
is desi
gn
ed to:
·
advocate
for H
I
V
/
S
TD
prevention and
c
ontrol
a
t
th
e
c
ountry level in Latin Ameri
c
a
an
d the
C
aribbean;
·
s
trengt
h
en management c
apa
c
ity to develop and implement poli
c
ies for H
I
V
an
d STD
prevention
and control;
·
involve nongovernmental organi
z
ations
(NC_
s
) in
p
r
e
v
ention
an
d
c
on
tro
l effo
rt
s
an
d
build netw
o
rks am
o
ng NGOs at the
c
o
untry level;
·
coordinate regional cooper
at
ion
w
i
th PAHO and th
e
W
or
ld H
ea
lth Or
g
an
i
za
tion
headquarter
s
;
and analyze financial and admini
s
trativ
e
data t
o e
n
s
ur
e effe
ctiv
e
e
xecuti
o
n and monit
o
ring
o
f nati
o
nal pr
o
gram
s
;
·
provide direct technic
al
cooper
at
ion
to
M
em
be
r
C
o
untr
ies in
clu
di
ng (b
ut
n
ot
l
i
m
ite
d
t
o
):
epid
e
mi
o
l
o
gical
analysi
s
; d
e
v
e
l
o
pm
e
nt
o
f
e
ducati
o
nal mat
e
rial
s
and
co
untry
HIV
/
STD surveillance rep
o
rts; lab
o
rat
or
y
support f
o
r STD diagn
o
sis, impr
o
v
e
m
e
nt
o
f
bl
oo
d saf
e
t
y
m
e
asur
e
s, et
c
.
·
promote research
a
bo
u
t H
IV
/
AI
DS
epi
d
e
m
io
l
o
g
ica
l tr
e
n
ds and
th
eir re
l
a
t
ion t
o o
t
h
er
STD; design of prevention messages b
as
ed on
c
ultural and other factors; studies on
socioeconomic
impa
c
t, etc.
·
disseminate information
(
t
e
c
hn
ical
an
d s
c
ienti
fi
c
)
to
an
d from Mem
be
r Coun
tr
ies;
·
establish sentinel surveillance
,
an
d advise
an
d train professionals to monitor H
I
V
/
STD
I
L
,AIDS Surveillance
in the Americas
(1
0 March
1996_
PAHO began its AIDS Survei
l
lan
c
e S
y
ste
m
in
1
986, although
c
as
e
s
h
ad
be
e
n r
e
p
orte
d
informally to PAHO since 1983. The information is
c
urrently submitted to P
A
HO from
4
7
c
ountries and territories of the Region of the Ameri
cas
. These data are received wi
th
in
3
0 to
4
5
days a
f
ter
th
e end of e
a
ch quarter. PAl-lO then produ
c
es
th
e present report, which is
distributed to all the
co
untries
in th
e Region. Twi
c
e a ye
ar
PAHO sends the information to the
World Heal
th
Organization he
ad
quarters
in
Geneva, Switzerland, where data are ga
th
ered from
all re
g
ions,
an
d produ
c
ed as
th
e Global A
I
DS Report.
As of
M
ar
c
h 1996, a cu
m
ul
a
tive
to
ta
l of 669,4
0
4 cases were repo
rt
ed in the Ameri
c
as.
From these, 11,643 are pediatric
c
a
ses
(<15
years old). A total of 392,751
cumulative
dea
t
h
s
have been reported sin
c
e
1
9
8
6.
C
ertain fa
c
tors su
c
h as underdiagnosis, underreportin
g
and delayed reporting affe
c
t
th
e completeness
of
th
e da
ta
.
!
Th
is should be considered when analyzing
1
99
5
da
ta
.
Additionally, many times
th
e
c
ountries provide
th
e number of
c
ases by year but can not repo
rt
the
c
orresponding age, sex
an
d risk fa
c
tor for
th
ose
c
ases.
PAl-lO
an
d its
M
ember S
ta
tes are working
c
ontinuously to improve the quality
and
c
ompleteness of
th
e info
rm
ation, to be able to analyze
an
d provide a better profile of the
epidemi
c
in ea
c
h conse
c
utive repo
rt
.
In
1
99
4
, the rate of reported A
I
DS
cas
es per million population in Latin Ameri
c
a was
5
2.9, in the
C
aribbe
an
201.2, and in
N
orth
Am
eri
c
a 20
5
.8.
Th
e primary modes of H
I
V
transmission in
th
e subregions are homo
/
bisexual
(
Andean Area, Sou
th
e
rn
Cone,
B
ra
z
il and
M
exi
c
o)
an
d heterosexual
(C
entral
Am
eri
can I
sthmus and
th
e
Car
ibb
e
an
)
. Tr
an
smission
attributed to
intr
avenous dru
g
use is
c
ommon in
th
e Sou
th
ern Cone and Bra
z
il wi
th
30%
an
d
2
7%, respe
c
tively.
In
th
is issue, we have added Fig.
4 "
Distribution of
c
umulative
AI
DS c
as
es by a
g
e, sex
and subregion
"
whi
c
h shows
th
e in
c
idence of A
I
D
S
by age group in ea
c
h subregion.
I
n the
Sou
th
ern
C
one
an
d
C
entral
A
me
ri
c
a
th
e age of the highest infe
c
tion is
in th
e
gr
oup between
2
0-2
9 years old for bo
th
sexes; this
h
olds for females in
B
r
az
il too.
I
n
th
e
A
ndean Area,
M
exi
c
o
an
d
th
e
C
arib
be
an
th
e age of infection is between 30-
3
9 ye
ar
s old for males
an
d females; this
a
g
e o
f
infe
c
tion is also frequent in males in
B
ra
z
il.
AIDS SURVEILLANCE
IN THE AMERICAS
Summary
Data received
by 10 March 1996
Cumulat
ive
number of cases reported
worldwide:
1,301,61 2
Cumulative
number
of cases
reported
in
t
he Americas:
669,464
Adul
t
s: 65
7
,821
Pedia
t
rics: 11,643
Cumulative
number of deaths re
p
orted
Fig
.
1. Annual in
c
idence of AIDS caseS,
"
by region of
t
he WHO, by year, 1979-94
/
95'.
-NUMBER OF CASES
1,000,000
...I
_tr _ __
100
000-AFRICA
",
AMERICAS
i
,,
,
lO,OOO
-
/
EUROPE
_;l'_r _ _J_ ;]"[; I _1 :_\'_'"_+_ _ / ="r';,!r' r ';r,r 'ryt(t,(' 1Jib I"" I,,,, :,,'',' ,,4
_.'_
'
OCE
AN
I
A
'""'? r r '....'r' '_
.vvvd,nnn
_
"
E, tE',
I1_ la3,."
[ ,t,, ,
,?r,i,"
r,
,,'' d=