OPHTHALMIC CONSULTATIONS IN A TEACHING HOSPITAL: DOES
IT MAKE A DIFFERENCE IN THE PATIENT MANAGEMENT?
Rajani Kadri1, Devika Parameshwar2, Nupur Raina3, Asha Achar4, Ajay Kudva5, Sudhir Hegde6
HOW TO CITE THIS ARTICLE:
Rajani Kadri, Devika Parameshwar, Nupur Raina, Asha Achar, Ajay Kudva, Sudhir Hegde. “Ophthalmic Consultations in A Teaching Hospital: Does it Make a Difference in the Patient Management?”. Journal of Evidence based Medicine and Healthcare; Volume 2, Issue 40, October 05, 2015; Page: 6619-6625,
DOI: 10.18410/jebmh/2015/903
ABSTRACT: BACKGROUND: Many a systemic diseases can be diagnosed by a comprehensive ophthalmic examination. Relevant ophthalmic consultations in a teaching hospital is hence of great importance in the management of patients. OBJECTIVE: To study referral pattern of patients and the importance of ophthalmology consultations in a teaching hospital. METHOD:
289 patients, referred to the Ophthalmology OPD of our hospital over a period of 5 months were included in this prospective study. Patient profile, referring department, the reason for referral and ocular findings were documented and the data was analysed. RESULTS: The mean age of referred patients was 46.43±20.81 years of whom 170(58.82%) were males & 119(41.18%) females. Patients were referred from 12 departments. 94(35.52%) had complaints, while 195(67.47%) were sent for screening. Majority of these patients, 169(58.48%) were referred from general medicine. 23(7.46%) new asymptomatic cases of glaucoma and 3 cases of PDR were identified and treated. The commonest cause of reference from paediatrics was headache
(31%). Paediatric cases with Crouzon’s syndrome and thalamic glioma underwent neurosurgical
intervention. CONCLUSION: Ophthalmic consultations in a teaching hospital make a significant difference in management of overall health of inpatients of various departments.
KEYWORDS: Referral, Ophthalmology, Screening, Complaints.
INTRODUCTION: Global burden of visual impairment roughly estimated as 285 million is clustered disproportionately among developing countries including India.1,2
The demand for better and low cost health services is increasing in developing countries.3,4 In India, medical college hospital cater to a large percent of population, thus inter
departmental references in a medical college hospital can take care of overall health of significant number of individuals. Ophthalmic consultations form a major portion of the referral in a medical college hospital. Referrals being from almost all the departments serve as an invaluable tool in diagnosing a wide range of ocular and systemic disorders that would have been left undetected otherwise.5
In our study an attempt has been made to assess how ophthalmic consultations can prove beneficial to the inpatients in a teaching hospital.
Patient profile, referring department, the reason for referral were documented. All patients were subjected to a comprehensive ophthalmic examination including best corrected visual acuity, anterior segment evaluation by slit lamp biomicroscopy, intraocular pressure by rebound tonometry and fundus examination by indirect ophthalmoscopy and s 90D lens for stereoscopic examination. Additional ophthalmic examinations like automated perimetry, syringing, fluorescein staining, shirmers test, diplopia charting and cycloplegic refraction was performed when indicated. The data obtained was tabulated and analysed.
Any intervention performed by ophthalmologists and any changes in the patients management attributed to the referral were also noted.
Inclusion Criteria: All referral patients examined in the ophthalmology department of our medical college hospital were included in the study.
Exclusion Criteria: Self-referral, referrals from general practitioners, primary health centres were excluded from this study.
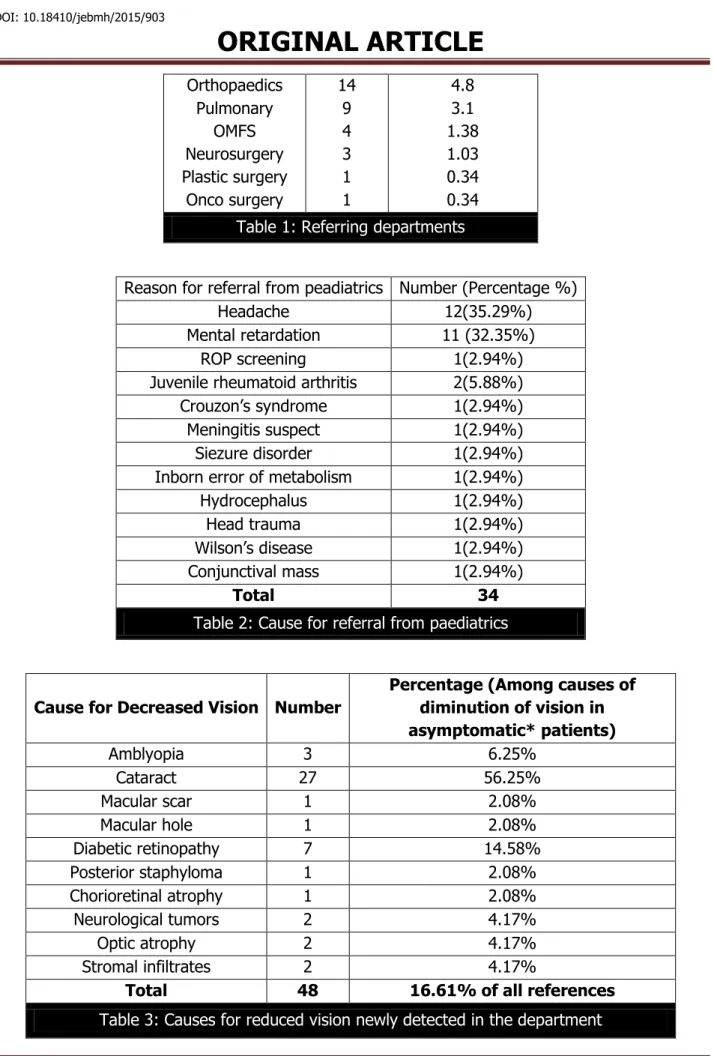
RESULTS: 578 eyes of 289 patients were examined following referral from various departments in medical college hospital. Average of 13.8 consultations per week was examined. Average age of the referred patients was 46.43±20.81yrs. 170(58.82%) males & 119(41.18%) females were referred from 12 departments. The referring departments are as given in Table1. Majority of the references were from General medicine department followed by paediatric department 34(11.76%).
Causes for referral from paediatrics department were as in Table 2.
While 195 (67.47%) were referred for screening purpose, 94(35.52%) were referred for ocular symptoms. Decreased vision was the cause for referral in 38 (13.15%) patients and was newly detected in the department in 48(16.61%) patients. Cataract 27(56.25%) was the most common cause followed by diabetic retinopathy in 7(14.58%) patients detected to have decreased vision. Various causes for decreased vision are shown in Table3.
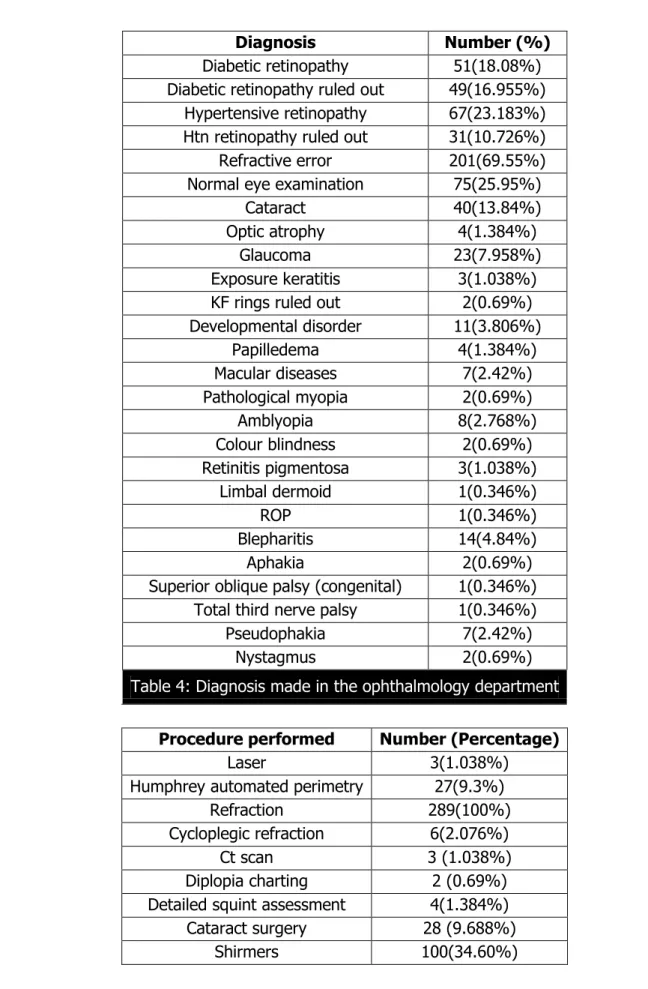
Table 4 outlines the diagnosis made in the ophthalmology department. Table 5 shows the various procedures performed on the referred patients.
The ophthalmic consultations were responsible for a change in management in 161(55.70%) out of 289 patients. These included 57 (35.40%) patients who were referred with complaints, and 104 (64.60%) who were referred for screening. The changes in overall better management included cataract surgery, correction of their refractive errors, laser photocoagulation, glaucoma management, reference to neurosurgery.
DISCUSSION: Interdepartmental references can become a boon to the patients especially in developing countries where access to the medical facility is limited.
In our study general medicine requested the maximum number of ophthalmic consultation with majority being to rule out diabetic retinopathy in diabetic patients, followed by paediatrics. Other studies have reported neurosurgery, neurology,5 internal medicine6,7 as their main subscribers for ophthalmic services. Physician’s awareness regarding ocular diseases in diabetics
could be the cause for these increased references.
Screening of all diabetic patients attending medicine outpatient department helps in early detection of silent cases of proliferative diabetic retinopathy (PDR) that causes sudden diminution of vision due to vitreous haemorrhage. In our study 3 patients with PDR and 1 patient with macular oedema received timely management.
Open angle glaucoma being asymptomatic, routine screening of patients has a major role to play in early detection and prompt management. In our study 23(7.9%) new glaucoma cases were diagnosed during the course of the study. All these patients were referred only for screening purpose. Early detection and management of primary open angle glaucoma is instrumental in preventing the progression of visual field defects in glaucoma. As visual morbidity due to glaucoma occurs late during the course of disease, patients are unaware that they have the disease and fail to get treatment at the right time in developing countries.8,9
Ocular symptoms may not be well expressed by children especially in the preverbal age. Gradually progressive painless diminution of vision caused by refractive errors, hereditary retinal dystrophies, developmental cataracts, need to be detected by screening alone. Wang Yu Dong et al,10 in a study on paediatric referrals found squint (57%) the most important cause for referral.
In our study headache which was the commonest cause for referral had simpler treatable causes
like refractive errors, vision threatening causes like optic atrophy as in Crouzon’s syndrome and
life threatening causes like thalamic glioma which were managed in time.
Cataract, the single largest cause of blindness is the cause of more than half of all blindness in low and middle economic countries.11,12, Out of the 40(13.84%) inpatients referred
for decreased vision and diagnosed to have cataract, 28(9.68%) were surgically managed. This approach can prove to be beneficial in developing countries to reduce the burden of treatable blindness.
90% of people with uncorrected refractive errors, worldwide reside in rural and low income countries.13 The cost to access eye services, lack of awareness of services, poor referral
networks seem to be the major barriers for availing services at secondary and tertiary centres.14
In our study 201(69.55%) patients with refractive errors were treated of whom 180(62.28%) had presbyopia. Hence the huge burden of visual impairment due to lack of awareness of refractive errors, un-affordability and unavailability of eye care services can be tackled to a certain extent by ophthalmic references in a medical college hospital.
This study though done with limited subjects during a short period emphasizes the fact that ocular morbidity can be detected to a large extent by screening more and more people. The implications of this study resulted in suggestion of an improvised protocol for referral of patients to the department of ophthalmology in our teaching hospital.
Diseases that are the causes of preventable blindness can be detected early and managed by screening more patients.
REFERENCES:
1. World health organisation: visual imparment and blindness fact sheet 282, 2011. Available from http://www. Who.int/mediacentre/factsheets/fs282/e/.
2. Armstrong KL, Jovic M, Vo-Phuoc JL, Thorpe JG, Doolan BL. The global cost of eliminating avoidable blindness. Indian J Ophthalmol 2012; 60: 475-80.
3. Van Doorslaer E, O'Donnell O, Rannan-Eliya RP, Somanathan A, Adhikari SR, et al. Effect of payments for health care on poverty estimates in 11 countries in Asia: an analysis of household survey data. Lancet. 2006; 368: 1357–1364.
4. Sudhan A, Khandekar R, Deveragonda S, Devi S, Jain BK, Sachan R et al. Patient satisfaction regarding eye care services at tertiary hospital of central India. Oman J Ophthalmol. 2011; 4: 73-6.
5. Bala C, Poon AC, Joblin P, McCluskey PJ. Ophthalmologists in teaching hospitals: do we make a difference to patient outcome? Clin Experiment Ophthalmol 2001; 29: 59-63.
6. Tajunisah I, Azida J, Zurina ZA, Reddy SC. Ophthalmology Inpatient Consultation: Does it Make a Difference to Inpatient Management? Med J Malaysia. 2009; 64: 130-133.
7. Carter K, Miller KM. Ophthalmology inpatient consultation. Ophthalmology 2001; 108: 1505-11.
8. Foster PJ, Thomas R, Glaucoma care in developing countries. In: Grehn F, Stamper R, editors. Essentials in Glaucoma. Berlin: Springer; 2006.
9. Thomas R. Glaucoma in developing countries. Indian J Ophthalmol 2012; 60: 446-50.
10.Wang YD, Thompson JR, Goulstine DB, Rosenthal AR. A survey of the initial referral of children to an ophthalmology department. Br J Ophthalmol. 1990; 74: 650- 653.
11.Neena J, Rachel J, Praveen V, Murthy GVS, for the RAAB India Study Group (2008) Rapid Assessment of Avoidable Blindness in India. PLoS ONE 3:e2867. doi:10.1371/journal.pone.0002867
12.Lindfield R, Vishwanath K, Ngounou F, Khanna RC. The challenges in improving outcome of cataract surgery in low and middle income countries. Indian J Ophthalmol 2012; 60: 464-9. 13.Naidoo KS, Jaggernath J.Uncorrected refractive errors. Indian J Ophthalmol 2012; 60:
432-7.
14.Chiang PP, Marella M, Ormsby G, Keeffe J. Critical issues in implementing low vision care in the Asia-Pacific region. Indian J Ophthalmol 2012; 60: 456-9.
Department Number Percentage (%)
General medicine General Surgery
OBG Paediatric Dermatology
ENT
169 30
9 34
3 12
58.48 10.38 3.1 11.76
Orthopaedics Pulmonary
OMFS Neurosurgery Plastic surgery
Onco surgery
14 9 4 3 1 1
4.8 3.1 1.38 1.03 0.34 0.34
Table 1: Referring departments
Reason for referral from peadiatrics Number (Percentage %)
Headache 12(35.29%)
Mental retardation 11 (32.35%)
ROP screening 1(2.94%)
Juvenile rheumatoid arthritis 2(5.88%)
Crouzon’s syndrome 1(2.94%)
Meningitis suspect 1(2.94%)
Siezure disorder 1(2.94%)
Inborn error of metabolism 1(2.94%)
Hydrocephalus 1(2.94%)
Head trauma 1(2.94%)
Wilson’s disease 1(2.94%)
Conjunctival mass 1(2.94%)
Total 34
Table 2: Cause for referral from paediatrics
Cause for Decreased Vision Number
Percentage (Among causes of diminution of vision in asymptomatic* patients)
Amblyopia 3 6.25%
Cataract 27 56.25%
Macular scar 1 2.08%
Macular hole 1 2.08%
Diabetic retinopathy 7 14.58%
Posterior staphyloma 1 2.08%
Chorioretinal atrophy 1 2.08%
Neurological tumors 2 4.17%
Optic atrophy 2 4.17%
Stromal infiltrates 2 4.17%
Total 48 16.61% of all references
Diagnosis Number (%)
Diabetic retinopathy 51(18.08%) Diabetic retinopathy ruled out 49(16.955%)
Hypertensive retinopathy 67(23.183%) Htn retinopathy ruled out 31(10.726%) Refractive error 201(69.55%) Normal eye examination 75(25.95%)
Cataract 40(13.84%)
Optic atrophy 4(1.384%)
Glaucoma 23(7.958%)
Exposure keratitis 3(1.038%) KF rings ruled out 2(0.69%) Developmental disorder 11(3.806%)
Papilledema 4(1.384%)
Macular diseases 7(2.42%)
Pathological myopia 2(0.69%)
Amblyopia 8(2.768%)
Colour blindness 2(0.69%)
Retinitis pigmentosa 3(1.038%)
Limbal dermoid 1(0.346%)
ROP 1(0.346%)
Blepharitis 14(4.84%)
Aphakia 2(0.69%)
Superior oblique palsy (congenital) 1(0.346%) Total third nerve palsy 1(0.346%)
Pseudophakia 7(2.42%)
Nystagmus 2(0.69%)
Table 4: Diagnosis made in the ophthalmology department
Procedure performed Number (Percentage)
Laser 3(1.038%)
Humphrey automated perimetry 27(9.3%)
Refraction 289(100%)
Cycloplegic refraction 6(2.076%)
Ct scan 3 (1.038%)
Diplopia charting 2 (0.69%) Detailed squint assessment 4(1.384%) Cataract surgery 28 (9.688%)
TBUT 100(34.60%)
Tonometry 255(88.23%)
Syringing 5(1.73%)
Flourescein staining 8(2.768%) Table 5: Procedures performed on referred patients
5. Associate Professor, Department of Ophthalmology, AJ Institute of Medical Sciences, Mangalore.
6. Professor & HOD, Department of Ophthalmology, AJ Institute of Medical Sciences, Mangalore.
NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajani Kadri,
Department of Ophthalmology, AJ Institute of Medical Sciences, Kuntikana,
Mangalore-575004.
E-mail: [email protected]
Date of Submission: 13/09/2015. Date of Peer Review: 14/09/2015. Date of Acceptance: 21/09/2015. Date of Publishing: 29/09/2015. AUTHORS:
1. Rajani Kadri
2. Devika Parameshwar 3. Nupur Raina
4. Asha Achar 5. Ajay Kudva 6. Sudhir Hegde
PARTICULARS OF CONTRIBUTORS: 1. Associate Professor, Department of
Ophthalmology, AJ Institute of Medical Sciences, Mangalore.
2. Consultant, Department of Pediatric Ophthalmology & Squint Services, AJ Institute of Medical Sciences,
Mangalore.
3. Junior Resident, Department of Ophthalmology, AJ Institute of Medical Sciences, Mangalore.