www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Thyroid
gland
invasion
in
advanced
squamous
cell
carcinoma
of
the
larynx
and
hypopharynx
夽
,
夽夽
João
Mangussi-Gomes
a,
Fernando
Danelon-Leonhardt
a,∗,
Guilherme
Figner
Moussalem
a,
Nicolas
Galat
Ahumada
a,
Cleydson
Lucena
Oliveira
a,
Flávio
Carneiro
Hojaij
a,baUniversidadeFederaldeSãoPaulo,DepartamentodeOtorrinolaringologiaCirurgiadeCabec¸aePescoc¸o,SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo,LaboratóriodePesquisasClínicas---LIM-32,SãoPaulo,SP,Brazil
Received2February2016;accepted23March2016 Availableonline7May2016
KEYWORDS
Squamouscell carcinoma; Larynx; Hypopharynx; Laryngectomy; Pharyngectomy; Thyroidectomy
Abstract
Introduction:Squamous cellcarcinoma ofthelarynx andhypopharynx has thepotential to invadethethyroidgland.Despitethisrisk,thepropositionofeitherpartialortotal thyroidec-tomyaspartofthesurgicaltreatmentofallsuchcasesremainscontroversial.
Objectives: Toevaluatethefrequencyofinvasionofthethyroidglandinpatientswithadvanced laryngeal or hypopharyngeal squamous cell carcinoma submitted to total laryngectomy or pharyngolaryngectomyandthyroidectomy;todetermine whetherclinic-pathological charac-teristicscanpredictglandularinvolvement.
Methods:Aretrospectivecaseserieswithchartreview,fromJanuary1998toJuly2013,was undertaken inatertiary careuniversitymedical center.An inception cohortof83 patients withlarynx/hypopharynxsquamouscellcarcinomawasconsidered.Allpatientshadadvanced stagedisease(clinicallyT3---T4)andunderwenttotallaryngectomyortotal pharyngolaryngec-tomyinassociationwiththyroidectomy.Adjuvanttherapywasindicatedwhentumororneck conditions required. Frequencyofthyroid cartilage invasionwas calculated; univariateand multivariateanalysisofdemographic,clinicalandpathologicalcharacteristicsassociatedwith cartilageinvasionwereperformed.
Results:Theoverallfrequencyofinvasionofthethyroidglandwas18.1%.Glandular involve-ment was associated with invasion ofthe following structures: anterior commissure (odds ratio=5.13; 95% confidence interval 1.07---24.5), subglottis (odds ratio=12.44; 95% confi-denceinterval1.55---100.00)andcricoidcartilage(oddsratio=15.95;95%confidenceinterval 4.23---60.11).
夽 Pleasecitethisarticleas:Mangussi-GomesJ,Danelon-LeonhardtF,MoussalemGF,AhumadaNG,OliveiraCL,HojaijFC.Thyroidgland
invasioninadvancedsquamouscellcarcinomaofthelarynxandhypopharynx.BrazJOtorhinolaryngol.2017;83:269---75.
夽夽Thisarticlehasbeenpresentedasan‘‘OutstandingPoster’’atthe2014AmericanAcademyofOtolaryngology---Head&NeckSurgery
Foundation(AAO-HNSF)Meeting&OTOEXPOSM,whichwasheldonSeptember21st---24th,inOrlando,FL,USA.
∗Correspondingauthor.
E-mail:fernandodanelon@me.com(F.Danelon-Leonhardt).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.03.019
Conclusions:Invasionofthethyroidglandisuncommoninthecontextoflaryngopharyngeal squamouscellcarcinoma.Clinicalandpathologicalfeaturessuchasinvasionoftheanterior commissure,subglottisandcricoidcartilagearemoreassociatedwithglandularinvasion. © 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Carcinoma espinocelular; Laringe; Hipofaringe; Laringectomia; Faringectomia; Tireoidectomia
Invasãodaglândulatireoidenocarcinomaespinocelularavanc¸adodelaringe ehipofaringe
Resumo
Introduc¸ão:Ocarcinomaespinocelulardelaringeehipofaringetem potencialpara invadira glândulatireoide.Apesar desserisco, aproposic¸ãode tireoidectomiaparcialoutotal como partedotratamentocirúrgicodetodosessescasospermanececontroversa.
Objetivos: Avaliarafrequênciadeinvasãodaglândulatireoideempacientescomcarcinoma espinocelularavanc¸adodelaringeouhipofaringesubmetidosalaringectomiatotalou faringo-laringectomiaetireoidectomia;determinarsecaracterísticasclínico-patológicaspodemprever oenvolvimentoglandular.
Método: Umasériedecasosretrospectivoscomrevisãodeprontuários,entrejaneirode1998e julhode2013,foifeitaemumcentromédicouniversitáriodecuidadosterciários.Umacoorte inicial de83pacientescomcarcinomaespinocelulardelaringe/hipofaringe foiconsiderada. Todosos pacientestinham doenc¸a em estágioavanc¸ado(clinicamente T3-T4) e foram sub-metidosalaringectomiatotaloufaringolaringectomiaemassociac¸ãocomtireoidectomia.Foi indicadaterapiaadjuvantequandootumorouascondic¸õesdopescoc¸oexigiram.A frequên-ciadeinvasãodecartilagemdatireoidefoicalculada;análisesunivariadaemultivariadadas característicasdemográficas,clínicasepatológicasassociadasàinvasãodecartilagemforam realizadas.
Resultados: Afrequênciaglobaldeinvasãodaglândulatireoidefoide18,1%.Oenvolvimento glandularfoiassociadoainvasãodasseguintesestruturas:comissuraanterior(oddsratio=5,13; intervalodeconfianc¸a95%1,07-24,5),subglote(oddsratio=12,44;intervalodeconfianc¸a95% 1,55-100,00)ecartilagemcricoide(oddsratio=15,95;intervalodeconfianc¸a95%4,23-60,11).
Conclusões:A invasão da glândula tireoide é rara no contexto de carcinoma espinocelular laringofaríngeo.Ascaracterísticasclínicasepatológicas,comoainvasãodacomissuraanterior, subgloteecartilagemcricoide,estãomaisassociadasainvasãoglandular.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Squamouscellcarcinoma(SCC)ofthelarynxand hypophar-ynx has the potential to invade the thyroid gland. This invasionoccursmainlybydirectextensionduetothe prox-imity of this gland to the pharyngolaryngeal region.1---3
Despitethisrisk, thepropositionof eitherpartial ortotal thyroidectomyaspartofthesurgicaltreatmentofallsuch casesremainscontroversial.2---6
Thefrequencyofneoplasticinvolvementofthethyroidin advancedSCCofthelarynxvariesintheliteraturebetween 1%and30%.4,5,7Accordingtothesefigures,thyroidsurgery
wouldbeunnecessarilyperformedinapproximately75%of patients.3 Just by adding hemithyroidectomy to the
sur-gical treatment of a laryngeal cancer increases the risks of hypothyroidism andhypoparathyroidism to23---63% and 25---52%,respectively.8---10
Adefinitionoftheclinicalandanatomopathological fea-turesassociatedwiththyroidinvolvementwouldbeofgreat
value in such cases. This definition could direct surgical treatment and reduce morbidity without impairing treat-mentobjectives.6,11
The aim of this study was to evaluate the frequency ofthyroidglandinvasioninpatientswithadvancedSCCof thelarynxandhypopharynxundergoingtotallaryngectomy (TL) or total pharyngolaryngectomy (TPL) associatedwith Hemithyroidectomy (HT) or total thyroidectomy (TT) and todeterminewhetherclinicalandpathologicalfeaturesare abletopredictthyroidglandinvolvement.
Methods
for SCCof thelarynxand hypopharynxin theperiodfrom January1998toJuly2013wereincluded.
Patients withmetastatic diseasewere excluded, along with patients undergoing partial or rescue surgery after radiotherapyandpatientswithincompleterecorddata.
The surgerieswereallperformedandallpatients mon-itored at a single Head and Neck Surgery service of a referenceuniversityhospital.Inthisservice,surgical exci-sionofthethyroidinassociationwithTLorTPLisindicated forpatientswithSCCofthelarynxandhypopharynxwhen there is evidence of tumor extension into the following regions: subglottis, pyriform sinuses, and extra-laryngeal tissue. HTor TT is performed according to the laterality of the tumor --- HT ipsilateral tothe tumor for unilateral tumors;TTfortumorswithbilateralinvolvement.
ThechoicebetweenTLandTPLdependsontheprimary siteandprogressionofthetumorintoadjacentregionsand aimstoachievesurgicalmarginsfreeofneoplasia.Advanced tumorsrestrictedtothelarynxrequireTL;laryngealtumors withpharyngealextensionorhypopharynxtumors,withor withoutlaryngealextension,arebettertreatedbyTPL.
Thefollowingclinicalandepidemiologicaldatawere ana-lyzedforallpatients:
Gender,age,currentorpasthistoryofsmoking; Primarytumorsite;
TNMandoverallstaging,accordingtoAmericanJoint Com-mitteeonCancer---AJCCcriteria;12
Surgeryperformed---TLorTPL,withHTorTT.
Thefollowinganatomopathologicalinformationwasalso noted:
Largesttumordiameterundermacroscopicexaminationof thesurgicalspecimen;
Presenceorabsenceofinvasionbytheprimarytumorofthe pyriformsinuses,anteriorcommissure,subglottis,thyroid, andcricoidcartilages.
Presenceorabsenceofmacroand/ormicroscopicthyroid glandinvasion;
Histologicalgradeofthetumor;
Presenceorabsenceofangiolymphaticandperineural inva-sion.
Subglottic invasion was considered when there was extensionofthetumororprimaryinvolvementbythe neo-plasmoftheregionlocatedmorethan10mmbelowthetrue vocalfolds.
The frequency of macroor microscopic involvementof thethyroidglandwascalculatedspecificallyforSCCforthe whole group of patients studied. The patients were then divided into two groups: (1) patients with thyroid gland involvement;(2)patientswiththyroidfreefromcarcinoma. Thetwogroupswerecomparedfordifferenceswithregard tothevariablesmentionedabove.
The study wasapprovedby theinstitution Ethics Com-mittee.SPSSv.17,Minitab 16,andExcelOffice2010 were usedforstatisticalanalysis.TheANOVAandthetwo-tailed Fisher’sexacttestswereappliedtoanalyzequantitativeand qualitativevariables,respectively.Thedegreeofassociation betweeninvolvementofthethyroidglandandother varia-bles was analyzed by calculating the oddsratio (OR) and
its95%confidenceinterval(95%CI).Valuesofp<0.05were interpretedasstatisticallysignificant.
Results
Datafrom83patientswerereviewedandanalyzed. Seventy-eight(94.0%)patientsweremale,and5(6.0%)werefemale. Themeanpatientage(±SD)was59.5±10.2years. Seventy-four (89.2%) patients had a current or past history of smoking.Theprimarytumorsitewasthelarynxin68(81.9%) casesandthehypopharynxin15(18.1%)patients.TheTNM stagingofthepatientsandthesurgeryperformedareshown inTable1.
Thyroid gland invasion by SCC was identified in 15 patients.Thefrequencyofglandularinvolvementwas18.1% (15/83)forallpatients.Amongthetumorslocated primar-ily in the larynx, the frequency of thyroid glandinvasion was19.1%(13/68). Considering onlyhypopharynxtumors, thefrequencyof glandularinvolvementwas13.3%(2/15). Invasionwasmacroscopic,bydirectextensionofthetumor, in13(86.7%) patients.Invasionwasidentifiedonly micro-scopicallyin2(13.3%)cases.
The comparison between the patient groups with and without thyroid involvement revealed that patients with evidenceofglandularinvasionshowedthefollowing char-acteristics:
Table 1 Patients with laryngeal and/or hypopharyngeal SCCsubmittedtoTLorTPLwithHTorTT---clinicaldata. Variable n(%)
Tstaginga
T3 26(31.3%)
T4a 57(68.7%)
Nstaginga
N0 45(54.2%)
N1 10(12.0%)
N2a 8(9.6%)
N2b 7(8.4%)
N2c 11(13.3%)
N3 2(2.4%)
Mstaginga
M0 83(100%)
M1 0(0%)
Globalstaginga
III 15(18.1%)
IVa 66(79.5%)
IVb 2(2.4%)
Performedsurgery
TL/TPL+HT 54(65.1%) TL/TPL+TT 29(34.9%)
SCC, squamous cell carcinoma; TL, total laryngectomy;TPL, totalpharyngolaryngectomy;HT,hemithyroidectomy;TT,total thyroidectomy;TL/TPL+HT,totallaryngectomyortotal pharyn-golaryngectomy with hemithyroidectomy; TL/TPL+TT, total laryngectomy or total pharyngolaryngectomy with total thy-roidectomy.
a TNMandGlobaltumorstaging,accordingtoAmericanJoint
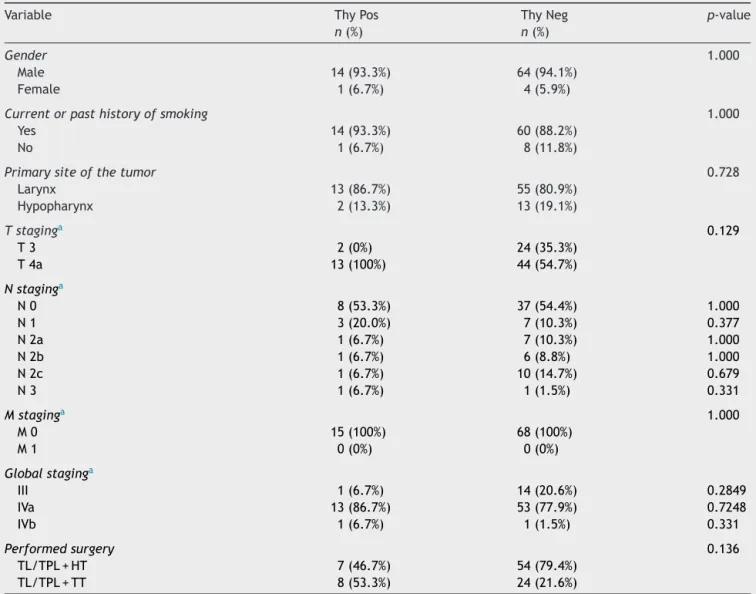
Table2 Comparisonbetweengroupsofpatientswithlaryngealand/orhypopharyngealSCCsubmittedtoTLorTPLwithHTor TT--- clinic-epidemiologicaldata.
Variable ThyPos ThyNeg p-value
n(%) n(%)
Gender 1.000
Male 14(93.3%) 64(94.1%) Female 1(6.7%) 4(5.9%)
Currentorpasthistoryofsmoking 1.000
Yes 14(93.3%) 60(88.2%) No 1(6.7%) 8(11.8%)
Primarysiteofthetumor 0.728
Larynx 13(86.7%) 55(80.9%) Hypopharynx 2(13.3%) 13(19.1%)
Tstaginga 0.129
T3 2(0%) 24(35.3%)
T4a 13(100%) 44(54.7%)
Nstaginga
N0 8(53.3%) 37(54.4%) 1.000
N1 3(20.0%) 7(10.3%) 0.377
N2a 1(6.7%) 7(10.3%) 1.000
N2b 1(6.7%) 6(8.8%) 1.000
N2c 1(6.7%) 10(14.7%) 0.679
N3 1(6.7%) 1(1.5%) 0.331
Mstaginga 1.000
M0 15(100%) 68(100%)
M1 0(0%) 0(0%)
Globalstaginga
III 1(6.7%) 14(20.6%) 0.2849
IVa 13(86.7%) 53(77.9%) 0.7248
IVb 1(6.7%) 1(1.5%) 0.331
Performedsurgery 0.136
TL/TPL+HT 7(46.7%) 54(79.4%) TL/TPL+TT 8(53.3%) 24(21.6%)
SCC,squamouscellcarcinoma;TL,totallaryngectomy;TPL,totalpharyngolaryngectomy;HT,hemithyroidectomy;TT,total thyroidec-tomy;TL/TPL+HT,totallaryngectomyortotalpharyngolaryngectomywithhemithyroidectomy;TL/TPL+TT,totallaryngectomyortotal pharyngolaryngectomywithtotalthyroidectomy;ThyPos,thyroidglandpositiveformalignancy;ThyNeg,thyroidglandnegativefor malignancy.
aTNMandGlobaltumorstaging,accordingtoAmericanJointCommitteeonCancer(AJCC)criteria.12
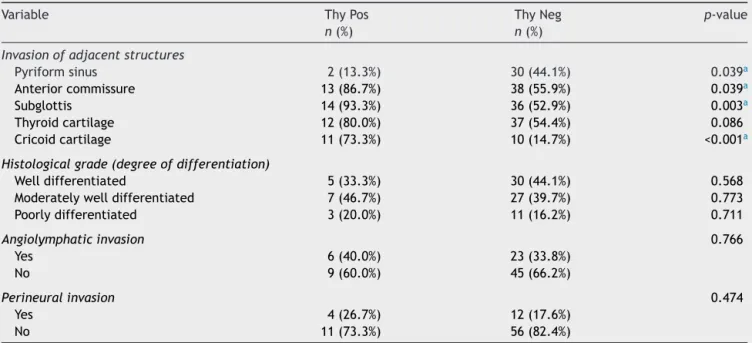
Higherratesofinvasionofthefollowingstructuresbythe primarytumor:
• Anteriorcommissure(p=0.039); • Subglottis(p=0.003);
• Cricoidcartilage(p<0.001).
The primary tumor invaded the pyriform sinus in only twocasesofthyroidinvolvement.Theseinstanceswerethe onlycasesofhypopharynxtumorsinpatientswithpositive thyroidmalignancy.Involvementofthepyriformsinus was statisticallylessfrequent inpatients withpositivethyroid malignancy(p=0.039).
Therewasnostatisticallysignificantdifferencebetween thegroupsregardinggender,age,presentand/orpast smok-ing,primarytumorsite,T,N,M,andglobalstaging,sizeof the tumor, surgery, histologicgrade, and the presence of
angiolymphaticorperineuralinvasion.Adetailed compari-sonbetweenthegroupsisshowninTables2---4.
When calculating the odds ratio (OR), thyroid gland invaded by neoplasia waspositively associated, with sta-tistical significance, with theinvolvement of the anterior commissure, the subglottis, and the cricoid cartilages by the primary tumor. The strongest association could be observed with cricoid cartilage involvement (OR=15.95, 95% CI 4.23---60.11).The ORcalculated for each variable, withtheirrespective95%confidenceintervals,areshownin
Table5.
Discussion
Table 3 Comparison between groups of patients with laryngealand/orhypopharyngealSCCsubmittedtoTLorTPL withHTorTT---ageandlargestsizeofthetumor.
Variable ThyPos ThyNeg p-value
Age(years)
Mean±SD 60.7±11.5 59.2±9.9 0.678
Largestsizeofthetumor(cm)
Mean±SD 5.5±2.7 4.3±1.5 0.943
SCC, squamous cell carcinoma;TL, total laryngectomy; TPL, totalpharyngolaryngectomy;HT,hemithyroidectomy;TT,total thyroidectomy;ThyPos,thyroidglandpositiveformalignancy; ThyNeg,thyroidglandnegativeformalignancy;SD,standard deviation.
thethyroid gland.This eventwasuncommon inthe cases presented.Thethyroidglandwasaffectedbythetumorin 18.1%,19.1%, and13.3%of casesofcarcinoma ofthe lar-ynx and hypopharynx, larynx only, and hypopharynxonly, respectively.Thesedataaresimilartotheresultsreported byotherauthors,accordingtowhomvaluesrangefrom1% to30%.3---5,7,9,13
Thyroid gland invasion is a poor prognostic factor in the context of laryngopharyngeal SCC.6,9,14 Nevertheless,
the frequencies found in this study suggest that thyroid surgery would be performed unnecessarily in more than 80% of these cases. It is known that the performance of thyroidectomy,whether totalor partial, greatly increases therapeutic morbidity. The occurrence of hypothyroidism and hypoparathyroidism, for example, greatly increases whenthyroid is partiallyor totallyremoved.4,8,9 Lo Galbo
et al., for example, showed that of 37 patients who underwent TL with HT in their series, 78.3% developed hypothyroidism within a 5 year follow up period.10
Like-wise,Mortimoreetal.demonstratedthattheincidenceof hypoparathyroidismwas25%inpatientsundergoingTLwith HTandadjuvantradiotherapy.15
Forallthesereasons,theindicationsforthyroidectomy aspart of the treatment of laryngopharyngeal carcinoma havebeenmuchdiscussedintheliterature.Therefinement ofcriteriathataremoststronglyassociatedwithglandular invasionwouldbeofgreatvalue,particularlyinthe reduc-tionofendocrinecomplications.2---6
Inthisstudynoassociationofthyroidglandinvolvement wasdemonstratedwithlymphnodestagingorwiththe pres-enceofangiolymphaticand/orperineuralinvasionsandthe microscopicanalysisoftumors.Furthermore,only2(13.3%) casesofthyroidtumorinvasionwerenotdetectedbasedon macroscopicextensionofthetumor.Thesefindings corrobo-ratethetheorythatglandularinvasionbylaryngopharyngeal SCCoccursmostcommonlybycontiguityordirectinvasion. Invasionoccurredthroughlymphaticdisseminationinonlya fewcasesand,muchmorerarely,hematogenically.2,5,9,11
Onemightimaginethatmoreaggressiveandless differ-entiatedtumorswouldhaveahigherfrequency ofthyroid glandinvasion.However,in thisstudy,therewas no rela-tionshipofglandularinvolvementwiththehistologicalgrade ofthetumor.Thisfindingisconsistentwiththefindingsof other authorsand maybeexplained bythe factthat less differentiated tumors are not necessarily larger or more expansive.4,11
Althoughpyriformsinusinvasionisaclassiccriterionfor performingthyroidectomyaspartofthetreatmentof laryn-gopharyngealSCC,thisstudydemonstratedthatthisfeature
Table4 Comparisonbetweengroupsofpatientswithlaryngealand/orhypopharyngealSCCsubmittedtoTLorTPLwithHTor TT---anatomopathologicaldata.
Variable ThyPos ThyNeg p-value
n(%) n(%)
Invasionofadjacentstructures
Pyriformsinus 2(13.3%) 30(44.1%) 0.039a
Anteriorcommissure 13(86.7%) 38(55.9%) 0.039a
Subglottis 14(93.3%) 36(52.9%) 0.003a
Thyroidcartilage 12(80.0%) 37(54.4%) 0.086 Cricoidcartilage 11(73.3%) 10(14.7%) <0.001a
Histologicalgrade(degreeofdifferentiation)
Welldifferentiated 5(33.3%) 30(44.1%) 0.568 Moderatelywelldifferentiated 7(46.7%) 27(39.7%) 0.773 Poorlydifferentiated 3(20.0%) 11(16.2%) 0.711
Angiolymphaticinvasion 0.766
Yes 6(40.0%) 23(33.8%)
No 9(60.0%) 45(66.2%)
Perineuralinvasion 0.474
Yes 4(26.7%) 12(17.6%)
No 11(73.3%) 56(82.4%)
SCC,squamouscellcarcinoma;TL,totallaryngectomy;TPL,totalpharyngolaryngectomy;HT,hemithyroidectomy;TT,total thyroidec-tomy;ThyPos,thyroidglandpositiveformalignancy;ThyNeg,thyroidglandnegativeformalignancy;SD,standarddeviation.
Table5 AssociationbetweenthyroidglandinvasionbySCCandanatomopathologicaldata---oddsratioand95%confidence interval.
Variable ThyPos ThyNeg OR(95%CI)
Invasionofadjacentstructures
Anteriorcommissure 5.13(1.07---24.5)a
Yes 13 38
No 2 30
Subglottis 12.44(1.55---100.00)a
Yes 14 36
No 1 32
Cricoidcartilage 15.95(4.23---60.11)a
Yes 11 10
No 4 58
OR,oddsratio;95%CI,95%confidenceinterval.
aStatisticallysignificantvalues(p<0.05).
wasmorefrequentinpatientswithneoplasia-freethyroids (p=0.039).Theonlytwocaseswheretherewasinvasionof thepyriformsinus andthyroid glandwererepresentedby theonly hypopharynxtumorsin thegroup of tumorswith positivethyroid.Thatis,inthesecases,thepyriformsinus wastheprimarysiteofthetumor,andthyroidglandinvasion occurreddue todownward growthof the carcinoma. The findings,whichisinaccordancewithotherstudies,indicate thattheinvolvementofthepyriformsinus alonedoesnot indicateglandularthyroidinvolvement.3,13
It was demonstrated that cases with thyroid positive for carcinoma were positively associated, with statisti-calsignificance,with invasionof theanteriorcommissure (p=0.039),thesubglotticregion(p=0.003),andthecricoid cartilage(p<0.001).This association wasrepeatedin cal-culating the odds ratio for these variables, which was strongestforcricoidcartilageinvolvement(OR=15.95,95% CI 4.23---60.11). Other studies have shown similar associ-ations to those found here.2,3,5,7,9,16 These data can be
explainedby the fact that these structuresare anatomi-cally positioned near areas of weakness of the laryngeal framework:thecricothyroidmembraneandtheparamedian cricothyroidspace.Itispreciselythroughtheseregionsthat carcinomasspreadtoextralaryngealtissues,especiallythe thyroidgland.5,7,8,11,14
However,not all findings mentioned above are consid-eredpredictors ofthyroidglandinvasionbyallauthors.A meta-analysisconductedbyMendelson etal.showedthat onlytransglottic or subglottic tumors or tumorswith sub-glotticextension>10mm wereassociatedwithinvasionof thethyroidgland.Despitethepositiveassociation,no statis-ticallysignificantcorrelationwasidentifiedwithinvasionof thecricoidandthyroidcartilages.11Onecriticismthatmay
bemadeofthatstudyisthatfewstudieswereincludedin itsanalysis,particularlywithregardtotheinvolvementof thelaryngealcartilages.
Inamorerecentstudy,Gaillardinetal.compared preop-erativefindingswiththeresultsofahistologicalstudyofthe thyroidgland.Theydemonstratedthatover40%ofpatients withsignsofinvasionofthecricoidcartilageincomputed tomography (CT)scans hadglandular involvement by car-cinoma. They concludedthat this type of examination is essentialin definingthyroidectomy indications.3 Likewise,
itissuggestedthattheinvasionofstructuresmorerelated tothyroidglandinvolvementshouldbeevaluatedpriorto surgery using the available diagnostic methods, such as endoscopyandCT.Thedecisionregardingtheperformance ofthyroidectomyanditsextensionshouldbebasedonthese findings.
Thisstudyhasinherent limitationsinthat itisa retro-spectivestudy,basedontheanalysisofmedicalrecordsand anatomopathologicalstudyreports.Especiallyfor this rea-son, it is subject toinformation bias. Moreover,although thecalculations ofoddsratiosexhibitedstatistical signifi-cance, theconfidence intervalswere relativelywide.The smallnumber of patients withthyroidinvolvement in our samplecouldexplainthisresult.Studieswithlargersamples andbettermethodologyareneededtobetterdefine indica-tionsforthyroidectomyinthecontextoflaryngopharyngeal SCC.
Conclusion
Thyroidglandinvasionbyneoplasiaisuncommoninthe con-textof laryngopharyngeal carcinoma. Tumors that involve theanteriorcommissure,thesubglottis,andespeciallythe cricoidcartilagearemorestronglyassociatedwithinvasion ofthisgland.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KirchnerJA.Pathwaysandpitfallsinpartiallaryngectomy.Ann OtolRhinolLaryngol.1984;93:301---5.
2.SparanoA,ChernockR,LaccourreyeO,WeinsteinG,Feldman M.Predictorsofthyroidglandinvasioninglotticsquamouscell carcinoma.Laryngoscope.2005;115:1247---50.
3.GaillardinL,BeutterP,CottierJ-P,ArbionF,MorinièreS.Thyroid glandinvasioninlaryngopharyngealsquamouscellcarcinoma: prevalence,endoscopicandCTpredictors.EurAnn Otorhino-laryngolHeadNeckDis.2012;129:1---5.
andpharyngolaryngealcarcinoma.OtolaryngolHeadNeckSurg. 2010;142:851---5.
5.DadasB,UsluB,CakirB,Ozdo˘ganHC,Calis¸AB,TurgutS. Intra-operativemanagementofthethyroidglandinlaryngealcancer surgery.JOtolaryngol.2001;30:179---83.
6.HillyO,RazR,VaisbuchY,StrenovY,SegalK,KorenR,etal. Thyroidglandinvolvementinadvancedlaryngealcancer: asso-ciationwithclinicalandpathologiccharacteristics.HeadNeck. 2012;34:1586---90.
7.Croce A, Moretti A, Bianchedi M. Thyroid gland involve-ment in cancer of the larynx. Acta Otorhinolaryngol Ital. 1991;11:429---35.
8.BielMA,MaiselRH.Indicationsforperforming hemithyroidec-tomy for tumors requiring total laryngectomy. Am J Surg. 1985;150:435---9.
9.KimJW,HanGS,ByunSS,LeeDY,ChoBH,KimY-M. Manage-mentof thyroid gland invasion in laryngopharyngeal cancer. AurisNasusLarynx.2008;35:209---12.
10.Lo GalboAM, Kuik DJ, Lips P,vonBlomberg BME, Bloemena E, Leemans CR, et al. A prospective longitudinal study on endocrine dysfunction following treatment of laryngeal or hypopharyngealcarcinoma.OralOncol.2013;49:950---5.
11.MendelsonAA,Al-KhatibTA,JulienM,PayneRJ,BlackMJ,Hier MP. Thyroidgland managementintotallaryngectomy: meta-analysisandsurgicalrecommendations.OtolaryngolHeadNeck Surg.2009;140:298---305.
12.GreeneFL,PageDL,FlemingID,GritzAG,BalchCM,HallerDG, etal.AJCCcancerstagingmanual.6thed.NewYork:Springer; 2002.p.421.
13.JoshiP,NairS,ChaturvediP,NairD,ShivakumarT,D’CruzAK. Thyroidglandinvolvementincarcinomaofthehypopharynx.J LaryngolOtol.2014;128:64---7.
14.Gallegos-Hernández JF, Minauro-Mu˜noz G, Hernández-Hernández DM, Flores-Carranza A, Hernández-Sanjuán M, Reséndiz-ColosiaJA.Thyroidectomyassociatedwith laryngec-tomyinlaryngealcancertreatment.Isitroutinelynecessary? CirCir.2005;73:3---6.
15.Mortimore S, Thorp MA, Nilssen EL, Isaacs S. Hypoparathy-roidismafterthetreatmentoflaryngopharyngealcarcinoma. JLaryngolOtol.1998;112:1058---60.