rev bras hematol hemoter. 2015;37(4):269–271
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Acquired
deficiency
of
coagulation
factor
VII
Vanessa
Afonso
da
Silva
∗,
Sheila
Soares
Silva,
Fabrício
Frederico
Mendes
Martins
UniversidadeFederaldoTriânguloMineiro(UFTM),Uberaba,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24October2014 Accepted25March2015 Availableonline3June2015
Introduction
FactorVII(FVII)isfoundinsmallamountsinplasmaandhas averyshorthalf-lifeincirculation.
FVIIisvitaminK-dependentlysynthesizedintheliver.As such,hepatopathies,vitaminKdeficiency,oruseofvitaminK antagonistsisthecauseofacquireddeficiency.Othertypesof acquiredFVIIdeficienciesarerare.1Herewedescribeacase ofacquiredfactorVIIdeficiencyassociatedtothepresenceof lupusanticoagulant.
Case
report
A36-year-oldblackmalepatientwashospitalizedinMarch 2013afterafour-dayperiodoflowbackpain,bruisedhips, macroscopichematuria,andgingivalbleeding.Atadmission, hewasconscious,oriented,pale,andtachycardic(108beats per minute), with a blood pressure of 120/90mmHg, mild edema,and varicose veins ofthe lower limbs.In addition, chronicmalleolarulcerswereobserved,withsignsof bleed-ingandbruisinginthepelvicregion.Thepatientdeniedany personalor family historyofbleeding diathesis. Renaland
∗ Correspondingauthorat:RuaGetúlioGuarita,s/n,38080-125Uberaba,MG,Brazil.
E-mailaddress:[email protected](V.A.daSilva).
urologicaldiseaseswerealsoruledout.Additional examina-tionsrevealedahemoglobinlevelof4.8g/dL,plateletcountof 270×109/L,andincoagulablebloodbasedontheprothrombin
time(PT)and activatedpartialthromboplastin time(APTT). Thepatientreceivedatransfusionofredbloodcells, cryopre-cipitateandfreshfrozenplasma.Hewasthentransferredto theintensivecareunit.Twodayslater,thepatientstill pre-sentedwithhematuria,ecchymosis,andincoagulableblood according toPT,with patient-to-controlAPTT ratioof1.79. Thus, transfusion supportwas continued. Thepatient had positiveresultsforlupusanticoagulantantibodiesand nega-tiveresultsforanticardiolipinimmunoglobulin(Ig)M,IgGand IgA antibodies,aswell asantinuclear and rheumatoid fac-tors.Theactivity levelsofthe coagulationfactors were3%, 130%,150%,>200%,47%,and75.8%forfactorsVII,II,V,VIII, IX and X,respectively. Wechosetostartintravenouspulse therapywithmethylprednisoloneandadministera prothrom-bincomplexconcentrateforpersistentbleeding.Thepatient recovered well, with no bleeding after the administration oftheprothrombincomplexconcentrateandcorticotherapy. Corticotherapywasmaintainedwiththeoraladministration of1mg/kg/dayprednisone.Thepatientwasdischargedafter 17daysofhospitalizationandreferredforfollow-upinan out-patientclinic.Thecorticoiddosewasreducedaftermonitoring
http://dx.doi.org/10.1016/j.bjhh.2015.05.002
270
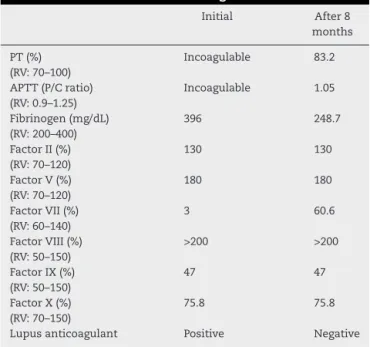
rev bras hematol hemoter. 2015;37(4):269–271Table1–Evolutionoftestsovereightmonths.
Initial After8
months
PT(%) (RV:70–100)
Incoagulable 83.2
APTT(P/Cratio) (RV:0.9–1.25)
Incoagulable 1.05
Fibrinogen(mg/dL) (RV:200–400)
396 248.7
FactorII(%) (RV:70–120)
130 130
FactorV(%) (RV:70–120)
180 180
FactorVII(%) (RV:60–140)
3 60.6
FactorVIII(%) (RV:50–150)
>200 >200
FactorIX(%) (RV:50–150)
47 47
FactorX(%) (RV:70–150)
75.8 75.8
Lupusanticoagulant Positive Negative
PT:prothrombintime;APTT:activatedpartialthromboplastintime; RV:referencevalue;P/Cratio:patient/controlratio.
intheclinic,andconsecutive PTtestresultsshoweda pro-gressivetendencytowardnormality.Thepatient’scondition stabilized,withoutnewhemorrhagicepisodes.Thecorticoid treatmentwassuspendedsixmonthsaftertheinitial adminis-tration.Twomonthsafter,thePTwas83.2%,patient-to-control APTTratiowas1.05,fibrinogenlevelwas248.7mg/dLandFVII activitylevelwas60.6%.
Table 1 shows the evolution of the main tests from hospitalization totwo monthsafterthe discontinuation of corticosteroids.
Discussion
Hereditarycoagulationfactordeficiencies,excepthemophilia, areautosomalrecessivehereditarydiseases,withincidences rangingfromonecasein500,000toonecaseintwomillion people.2Thus,theyareconsideredrarecoagulopathies.The suspecteddiagnosisisconfirmedusingprolongedPTand/or APTT,thereby suggesting the need forfurtherevaluations. Amongtherarecongenitalfactordeficiencies,FVIIdeficiency is the most common.2 The clinical manifestations of this conditionrange from asymptomaticto severehemorrhagic disorders,althoughthemostcommonbleedingsitesarethe skinandmucosae.3
AcquiredFVIIdeficiency,whichisnotassociatedwith vita-minKdeficiency,antagonistsorhepatopathies,thoughrare, is correlated with the presence of different tumors,1,4 the occurrenceofsepsis,5antiphospholipidantibodies,6aplastic anemia7andhematopoieticstemcelltransplantation.8
Coagulation inhibitors are abnormal endogenous com-poundsthatinhibitbloodcoagulation.Mostoftheseinhibitors areantibodiesthatpartiallyorcompletelyneutralizethe acti-vationorfunctionofaspecificcoagulationfactor,but they canalsointerferewithinteractionsbetweenseveralfactors.
Inmostcases,theseantibodiesleadtodeficiencyofaspecific factorduetoincreasedperipheralclearance.6
Thepresenceoflupusanticoagulantwasoriginally iden-tifiedinassociationwithsystemiclupuserythematosusbut iscurrentlydescribedasassociatedwithotherinflammatory andbenigndiseases,aswellasinhealthyindividualswithout anyapparentunderlyingdisease.9Invitro,lupusanticoagulant isassociatedwithprolongedAPTTandrarelytoprolongedPT. Invivo,thesituationisdifferentanditisstronglyassociated witharterialandvenousthrombosesandrarelywithbleeding. However,thepresenceoflupusanticoagulantmayalsobe associatedwith antibodies againstFVII,resulting insevere hemorrhagic diathesis.Inastudyof33patientspresenting withantiphospholipidsyndrome,Bidotetal.10reportedthat 67%ofthepatientshadlowFVIIlevels.
There are reports of acquired FVII deficiency associ-atedwithdifferentclinicalconditions.GrangerandGidvani1 describedacaseofFVIIdeficiencyinassociationwithWilms’ tumor in a 2-year-old child, and Fatimi et al.4 reported a 64-year-oldpatientwithisolatedprolongedPT,severe reduc-tionsinFVIIactivity,andagiantrightatrialmyxoma.After thesurgicalremovalofthemyxoma,thePTnormalizedand the FVII activity level increased within the first 24h after surgery. Bidet et al.5 described a 24-year-old patient with intra-abdominalsepticfocuswhodevelopedFVIIdeficiency, withoutevidenceofinhibitors;thedeficiencypartially recov-eredonlywiththeintravenousadministrationofvitaminK. Withtheresolutionofsepsis,thepatient’sPTandFVII activ-itynormalized.Limetal.6reporteda71-year-oldpatientwith anexpandinghematomaofthethoracicandabdominalwalls, andprolongedAPTTandPT.Additionalexaminationsrevealed apotentlupusanticoagulantandreducedlevelsofmultiple coagulationfactors.
Itisnoteworthythat,inthecurrentcase,theprolongedPT mayberelatedtothefactorVIIdeficiencyandtheprolonged APTTtothe presenceoflupusanticoagulant,but it is pos-siblethathighlevelsoflupusanticoagulantcanaffectboth PTandAPTT6,11and,althoughrare,thetitersmaybereduced orevennormalizedwithimmunosuppressivetherapy.11 How-ever,theparadoxicaleffectofthrombotictendencyshouldbe remembered inthepresenceoflupusanticoagulantinvivo asthereare reportsofthromboticcomplicationsduetothe treatmentofsecondarybleedingusingprothrombincomplex concentratesandrecombinantactivatedFVIIinthepresence oflupusanticoagulants.12,13
Thispatientdidnotpresentthromboticcomplications sec-ondary tothe treatmentinstituted and,althoughhehad a historyofvenousinsufficiencyandchronicmalleolarulcers, there isno evidenceofcurrent or previous venous throm-boembolism.Sothediagnostic criteriaforantiphospholipid syndromeshouldnotbeclosedbecause,despitehaving pos-itive lupus anticoagulanttest results, there are no clinical criteria,namely:(1)arterial,venousorsmallvesselthrombosis occurringinanytissueor(2)miscarriagesinwomen.14
rev bras hematol hemoter. 2015;37(4):269–271
271
useddependingonthe severityofbleedingandtheir avail-abilityineachinstitution.Somereportsdescribetheuseof immunomodulatorytherapies,withvaryingsuccess depend-ingonindividualpatients.Noteworthywasthesuccessfuluse ofrFVIIatocontrolacquiredandcongenitalFVII deficiency-inducedbleeding,whichwasadministeredinrepeateddoses untiltheriskofhemorrhagewaseliminated.12,13,15
Althoughthepresenceofalupusanticoagulantisoften related to thrombotic events, in this study, we describe a patientwith anassociated bleedingdisorder. During treat-ment, the patient did not present other symptoms that justifiedFVIIdeficiency.Aswehaveobserved,lupus anticoag-ulantmayalsodevelopinnormalindividuals.Thiscasestudy wasbasedontheadministrationandsubsequent discontin-uationofhighdosesofcorticoids,andtheadministrationof prothrombincomplexconcentratestocontrolacutebleeding. Theclinicalcourseofthepatientwassatisfactory.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GrangerJ,GidvaniVK.AcquiredfactorVIIdeficiency associatedwithWilmstumor.PediatrBloodCancer. 2009;52(3):394–5.
2. SalciogluZ,TugcuD,AkcayA,SenHS,AydoganG,AkiciF, etal.Surgicalinterventionsinchildhoodrarefactor deficiencies:asingle-centerexperiencefromTurkey.Blood CoagulFibrinolysis.2013;24(8):854–61.
3. SalciogluZ,AkcayA,SenHS,AydoganG,AkiciF,TugcuD, etal.FactorVIIdeficiency:asingle-centerexperience.Clin ApplThrombHemost.2012;18(6):588–93.
4. FatimiSH,Ali-KhawajaRD,KianiSK.Imagingand
interventionofparaneoplasticeffectofarightatrialmyxoma
onfactorVIIactivitylevels.AnnThoracSurg. 2011;91(1):278–81.
5.BidetA,Boiteux-VergnesC,MoutonC.Déficitacquisetrépété enfacteurVIIaucoursd’épisodesinfectieux:àproposd’un cas.AnnBiolClin(Paris).2009;67(5):587–9.
6.LimS,ZuhaR,BurtT,ChackoJ,ScottR,MainwaringCJ. Life-threateningbleedinginapatientwithalupusinhibitor andprobableacquiredfactorVIIdeficiency.BloodCoagul Fibrinolysis.2006;17(8):667–71.
7.WeisdorfD,HasegawaD,FairDS.AcquiredfactorVII deficiencyassociatedwithaplasticanaemia:correctionwith bonemarrowtransplantation.BrJHaematol.
1989;71(3):409–13.
8.ToorAA,SlungaardA,HednerU,WeisdorfDJ,KeyNS. AcquiredfactorVIIdeficiencyinhematopoieticstemcell transplantrecipients.BoneMarrowTransplant.
2002;29(5):403–8.
9.KyriakouDS,AlexandrakisMG,PassamFH,FoundouliK, MatalliotakisE,KoutroubakisIE,etal.Acquiredinhibitorsto coagulationfactorsinpatientswithgastrointestinaldiseases. EurJGastroenterolHepatol.2002;14(12):1383–7.
10.BidotCJ,JyW,HorstmanLL,HuishengH,JimenezJJ,YanizM, etal.FactorVII/VIIa:anewantigenintheanti-phospholipid antibodysyndrome.BrJHaematol.2003;120(4):618–26. 11.KaaroudH,BejiS,GuermaziS,MoussaFB,HamidaFB,Ezzine
S,etal.Bleedingandthrombosisinapatientwithsecondary antiphospholipidsyndrome.SaudiJKidneyDisTranspl. 2008;19(2):227–31.
12.BartoshNS,TomlinT,CableC,HalkaK.Newlydiagnosed congenitalfactorVIIdeficiencyandutilizationof recombinantactivatedfactorVII(NovoSeven®).Clin
Pharmacol.2013;5(1):53–8.
13.MahaleR,RathiP,GinegiriC,AggarwallR.FactorVII deficiency:ararecasereport.IndianJHematolBlood Transfus.2010;26(2):68–9.
14.LimW.Antiphospholipidsyndrome.ASHEducBook. 2013;2013(1):675–80.
15.MullighanCG,RischbiethA,DuncanEM,LloydJV.Acquired isolatedfactorVIIdeficiencyassociatedwithseverebleeding andsuccessfultreatmentwithrecombinantFVIIa