PHASE PROGRESSION THROUGHOUT THE THERAPEUTIC PROCESS: LONGITUDINAL CASE STUDIES
Joana Fojo Ferreira
Orientadores: Professor Doutor António José dos Santos Branco Vasco Professor Doutor Michael Basseches
Tese especialmente elaborada para obtenção do grau de Doutor no ramo de Psicologia, especialidade de Psicologia Clínica
PHASE PROGRESSION THROUGHOUT THE THERAPEUTIC PROCESS: LONGITUDINAL CASE STUDIES
Joana Fojo Ferreira
Orientadores: Professor Doutor António José dos Santos Branco Vasco Professor Doutor Michael Basseches
Tese especialmente elaborada para obtenção do grau de Doutor no ramo de Psicologia, especialidade de Psicologia Clínica
Júri:
Presidente: Doutora Isabel Maria de Santa Bárbara Teixeira Nunes Narciso Davide, Professora Associada e Vice-Presidente do Conselho Científico da Faculdade de Psicologia da Universidade de Lisboa
Vogais:
- Doutor Victor Manuel Martinez Pimentel Cláudio, Professor Auxiliar, Departamento de Psicologia Clínica e da Saúde do ISPA - Instituto Universitário de Ciências Psicológicas, Sociais e da Vida
- Doutor David Manuel Dias Neto, Professor Auxiliar, Instituto Superior de Estudos Interculturais e Transdisciplinares do Instituto Piaget
- Doutor João Manuel de Castro Faria Salgado, Professor Auxiliar, Instituto Universitário da Maia - ISMAI
- Doutor António José dos Santos Branco Vasco, Professor Catedrático, Faculdade de Psicologia da Universidade de Lisboa, orientador
- Doutor Nuno Miguel Silva Conceição, Professor Auxiliar Convidado, Faculdade de Psicologia da Universidade de Lisboa
i
ACKNOWLEGMENTS
Along this journey, I have had the good fortune to count on many people who have helped and inspired me in different ways.
My first acknowledgment necessarily goes to my supervisor, António Branco Vasco – you have accompanied me throughout this project and been the first and most important influence on the therapist and researcher I am today. By broadening my horizons and teaching me the importance of integrating different perspectives, you have shown me the way to a more comprehensive view of patients and their problems. You brought out and fostered the researcher in me to the point where I now constantly wonder what else can I learn about my patients, how better can I help them.
I would like to thank Michael Basseches, my co-supervisor, for the meetings we had to discuss the project design, our joint workshops, the deep reflections on human change and how to analyze it, your measured feedback and words of encouragement, the confidence you had in me, your kind words and hugs of reassurance.
Heartfelt thanks to my team of researchers, Andreia Santos, João Miguel Ferreira, Nuno Conceição and Catarina Vaz Velho, who promptly volunteered to analyze the cases with me. Thank you for your company, your involvement and your joint reflections.
To Nuno Conceição I owe additional thanks for being part of my academic and professional life for so long, and for consistently being there for me with important feedback, challenges and incentives throughout these years.
I should also like to thank Andreia Santos for her friendship, for the hours we spent discussing cases and clinical challenges, and for telling me at some point that I
ii
I deeply thank the patients, therapists and original research teams who made these analyses possible; the external adjudicators for the feedback you provided; Cícero Pereira for your indispensable help with the statistics; and Melinda Eltenton for the English revision.
I also thank the Paradigmatic Complementarity Lab for your support, team work and the joint project.
More closely connected to my clinical practice, but with an important influence on my research, I thank my clinical supervisors throughout these years – António Branco Vasco, Hans Welling, Isabel Gonçalves and Catarina Vaz Velho – who always sparked my curiosity and interest in my patients’ functioning, and in how to bring about the desired changes.
Likewise, I deeply thank my patients, both present and past, for giving me so much of themselves. It is a privilege to accompany or have accompanied your personal growth and to be a part of it.
I also thank my colleagues for always being there with kind words and reflections, for letting me share my difficulties with you, and for sharing your resources with me. Thank you for your presence and availability.
On a more personal note, I thank my friends for the laughter, for helping me to find a balance between work and leisure and for keeping me sane.
A big thank you, too, to my extended family, for believing in my worth, for being proud of me and being part of my life.
iii
And lastly, but most important, deepest thanks to my parents. My mother for her unconditional support. You have always had my best interests at heart, always believed in my choices, and supported my projects. Especially this one, which you so kindly financed. And my father for the legacy; you didn’t have the chance to accompany me on this project, but much of what I am, I am because of you, because of what you allowed me to be and believed I could become. Though not physically, I felt your support and your pride all the time, and that gave me immense strength, thank you!
v
DECLARATION
According to Article 41 of the Regulations for Postgraduate Studies of the University of Lisbon, approved by Resolution of the Rectory No 1506/2006, this dissertation encompasses scientific articles submitted for publication to international indexed journals in collaboration with other authors. The author states that she was authorized to analyze the data of this study (previously collected by other authors), was responsible for data analysis and interpretation of results (with the help of four other researchers), and was responsible as well for the writing, submission and review of the papers submitted for publication.
Joana Fojo Ferreira July of 2015
vii
ABSTRACT
The purpose of this study was to explore, in specific cases, the value of adding a phase-by-phase perspective to the more common, and essential, moment-by-moment analyses.
With this aim, and in order to better understand the therapeutic process and patients’ development throughout it, we gathered a team of researchers to track markers of intermediate sequential gains in each case, and explored the processes of change that favored these intermediate gains.
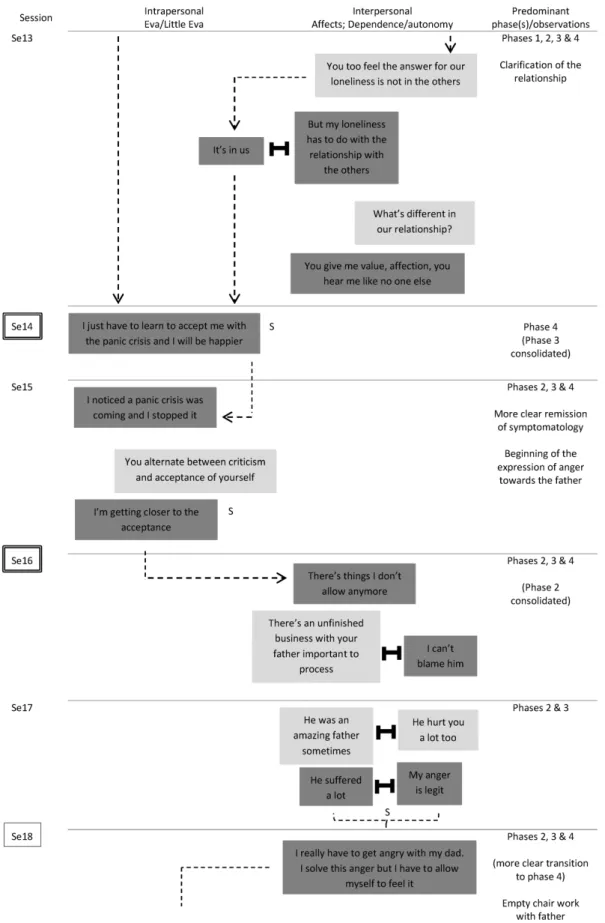
We analyzed three longitudinal case studies in light of the temporal sequencing component of the Paradigmatic Complementarity Metamodel (PCM) and used the Developmental Analysis of the Psychotherapy Process (DAPP) Method to understand moment-by-moment how phase-by-phase changes developed and were co-constructed in each case. The first case study involved analyzing the first year of a 4-year therapy of a female patient complaining of panic and depression. She was accompanied by a male therapist following an integrative approach and familiar with the PCM principles. The second case study involved analyzing a short-term process of a female with depression. She was accompanied by a female therapist following Emotion-Focused Therapy. The third case study involved analyzing a short-term process of a female victim of intimate violence. She was accompanied by a female therapist following Narrative Therapy.
In all three cases both patients and therapists tendentiously followed the sequence of phases proposed by the PCM, at least until phase 4 (regulation of responsibility). For each case, we present both the quantitative and qualitative analyses in order to clarify how each process unfolded and what, in each, contributed to the phase transitions and consolidations observed.
viii
an article, and explore the implications and limitations of the entire study at the end, providing suggestions for future research.
Keywords: Process Research; Processes of change; Tracking and Sequencing; Case
ix
RESUMO
O presente estudo procurou averiguar, em casos específicos, se a contemplação de uma sequência de fases a nível estratégico acrescenta valor à compreensão da evolução do processo terapêutico.
Inspirado no repto de Goldfried (1980) de identificar princípios de mudança terapêutica a um nível estratégico (intermédio), mais do que identificar ingredientes ou técnicas específicas que possam influenciar o sucesso de uma terapia, o Metamodelo de Complementaridade Paradigmática (MCP) investigou princípios de mudança terapêutica transversais às diferentes abordagens e, adotando uma perspetiva desenvolvimentista, ordenou-os numa sequência em que as competências desenvolvidas numa fase beneficiam o desenvolvimento das competências das fases seguintes. Segundo este modelo, a sequência de fases a promover ao longo do processo terapêutico passa por 1) Confiança, motivação e estruturação da relação, 2) Aumento da consciência da experiência e do Self, 3) Construção de novos significados relativos à experiência e ao Self, 4) Regulação da responsabilidade, 5) Implementação de ações reparadoras, 6) Consolidação da mudança, e 7) Antecipação do futuro e prevenção da recaída.
Neste estudo, em continuação de estudos anteriores (e.g. Conceição, 2005, 2010; Ferreira, Conceição & Vasco, 2011; Rodrigues, 2012; Simões, 2012), propusemo-nos verificar se esta sequência surge em casos específicos e, surgindo, procurámos identificar marcadores de transições e consolidações de fase e explorar no processo terapêutico que processos de mudança contribuíram para o desenvolvimento das competências observadas.
Analisámos, portanto, cada estudo de caso à luz do MCP, e integrámos o Método de Análise Desenvolvimentista do Processo Psicoterapêutico (ADPP), que
x
mudança terapêutica associadas às fases do MCP e analisar que elementos do processo terapêutico favoreceram o desenvolvimento do paciente.
O método ADPP propõe que os pacientes evoluem na progressiva síntese de teses e antíteses, e que estas sínteses são favorecidas pela identificação e trabalho sobre conflitos entre ideias contraditórias. Paralelamente, o método ADPP também estimula a reflexão sobre que recursos o terapeuta está a oferecer ao paciente, como é que o paciente os recebe, e como é que o terapeuta por sua vez se adapta ao que o paciente mostra conseguir ou não receber. Os três grandes recursos que o método ADPP propõe identificar são Suporte Atencional, Interpretação, e Enactment (associado à apropriação/ação de uma competência). Neste estudo usámos o método ADPP para, aquando da identificação de um marcador de ganhos intermédios, identificar os processos que o favoreceram – identificar teses e antíteses originais, que recursos o terapeuta utilizou para salientar ou resolver o conflito entre elas, e como é que chegaram a uma síntese mais saudável e num nível de desenvolvimento superior.
Analisámos três estudos de caso longitudinais: um primeiro, o primeiro ano de um processo de 4 anos de uma paciente com queixas de pânico, depressão e dificuldades no relacionamento familiar, com traços de personalidade dependente, evitante e auto-derrotista, acompanhada por um terapeuta integrativo, seguidor dos princípios do MCP e que integra as abordagens Terapia Focada nas Emoções, Dinâmica Relacional, Existencial e Cognitivo-Comportamental. O segundo, um processo de curta-duração de uma paciente deprimida e com traços dependentes, acompanhada por uma terapeuta que segue a abordagem da Terapia Focada nas Emoções. E o terceiro, um
xi
processo de curta-duração de uma paciente vítima de violência doméstica, acompanhada por uma terapeuta que segue a abordagem da Terapia Narrativa.
Cada estudo de caso foi analisado individualmente com análises quantitativas e qualitativas, que são apresentadas no capítulo 2 desta dissertação. Ambas as análises foram feitas por equipas de 3 avaliadores, que analisaram cada sessão individualmente, preencheram uma grelha com os objetivos estratégicos de cada fase (apresentados na Figura 1 na Introdução) identificando dois parâmetros: 1) quanto é que o terapeuta promoveu cada objetivo estratégico naquela sessão e 2) quanto é que o paciente se mostrou capaz de assimilar cada objetivo estratégico naquela sessão. Estas avaliações quantitativas foram discutidas pelos 3 elementos a cada sessão, ainda que cada um tenha cotado de acordo com a sua perceção em caso de desacordo. Os avaliadores salientaram ainda os excertos que consideraram mais salientes e mais representativos de transições e consolidações de fase, e no fim de todas as sessões do caso analisadas, voltaram a reunir-se para discutir a evolução do caso, os principais marcadores de conquistas intermédias e sequenciais, e aproveitando o método ADPP, identificar os processos de mudança ao longo do processo que favoreceram estas conquistas.
Os resultados de todos os três casos denotaram que tanto as pacientes como os terapeutas seguiram, tendencialmente, a sequência de fases proposta pelo MCP, pelo menos até à fase 4 (regulação da responsabilidade). No terceiro estudo de caso todas as fases estiveram presentes e de forma sequencial, no primeiro e segundo estudos de caso as últimas fases (a partir da fase 5 – Implementação de ações reparadoras) não estiveram significativamente presentes. No primeiro ainda houve 3 anos de terapia posterior, onde as últimas fases poderão ter sido trabalhadas, no segundo o processo terapêutico terminou sem o trabalho destas últimas fases consolidado.
xii
sugerem ainda, no mesmo sentido do preconizado por Stiles, Honos-Webb and Surko (1998), que a responsividade dos terapeutas às necessidades e competências dos pacientes é um fator determinante no sucesso de uma terapia; e acima de tudo o que a sequência de fases do MCP procura incutir, assim como o ADPP, é o cuidado de atentar nas capacidades e vulnerabilidades processuais dos pacientes e promover intervenções ao encontro de onde os pacientes estão e do que conseguem assimilar.
A integração de um modelo de fases com um método de análise momento-a-momento também mostrou ser muito útil para a análise do que favorece bons resultados terapêuticos, e parece ser promissora para a análise de casos com menos bons resultados e impasses e ruturas na relação. Estes potenciais são elaborados num quarto artigo incluído no 3º capítulo desta dissertação.
Iniciamos a dissertação com a exposição dos princípios, ideias e modelos terapêuticos na base do nosso estudo: desenvolvemos a ideia do processo terapêutico como um processo de desenvolvimento, exploramos conceitos e ideias da psicoterapia integrativa e fatores comuns, clarificamos princípios de mudança terapêutica a nível intermédio e processos de mudança a diferentes níveis de abstração, identificamos que a mudança terapêutica é co-construída pelo paciente e terapeuta, e elaboramos sobre a importância da responsividade. Apresentamos o MCP e o Método ADPP, e incluímos também considerações metodológicas ligadas à investigação de processo, conjugação de metodologias quantitativas e qualitativas, e estudos de caso longitudinais e com aspirações de criação e aprimoramento de teorias de mudança humana.
xiii
Apresentamos posteriormente, no 2º capítulo, os três estudos de caso, cada um constituindo um artigo em que são incluídas as análises quantitativas e qualitativas de cada um, e terminamos com uma discussão integrada dos casos, no 3º capítulo, onde apresentamos os resultados comuns, exploramos a evolução de cada fase, discutimos a utilização do MCP a nível macro (fase-a-fase) e micro (momento-a-momento) e a articulação dos dois, elaboramos sobre a responsividade dos terapeutas nestes três casos, exploramos desafios de analisar processos curtos à luz de um modelo de fases, e refletimos sobre a pertinência de um modelo de 7 fases sequenciais. Neste último capítulo incluímos ainda o 4º artigo com uma reflexão sobre os benefícios da integração de princípios fase-a-fase com um método de análise momento-a-momento, e onde apresentamos também linhas orientadoras para a reflexão clínica de casos em processo; e finalizamos o capítulo com a exposição das implicações e limitações do estudo, e sugestões para investigação futura, que passam essencialmente por analisar mais casos, e também casos de longa duração, mais complexos e com menos bons resultados.
Palavras-chave: Investigação de processo; Processos de mudança; Identificação e
xv
CONTENTS
List of Tables ………... xix
List of Figures ……….. xx
List of Acronyms ………. xxi
CHAPTER I – Introduction Introduction ………... 1
Principles and ideas of psychotherapy important to this study Psychotherapy as a developmental process ………. 1
Psychotherapy Integration ……… 5
Common factors ……… 7
Principles of therapeutic change ………... 9
Responsiveness ………..………... 11
Change processes at different levels of abstraction ………..……… 13
Psychotherapy models at the base of this study Temporal sequencing component of the Paradigmatic Complementarity Metamodel ……….………... 17
The Developmental Analysis of Psychotherapy Process Method …...…….… 22
Research principles and methodologies important to the present study Process research ………...……. 26
Theory-building research ………..……… 29
Methodological pluralism ………. 29
xvi
CHAPTER II – Case studies
Case study 1 – Exploring phase progression throughout the therapeutic process: the case of Eva
Abstract ………. 39
Introduction ………... 41
The present study ……….. 50
Method ……….. 52
Results ………... 57
Discussion ………. 75
Case study 2 – Tracking and understanding phase progression in Lisa’s case Abstract ………. 81
Introduction ………... 83
The present study ……….. 90
Method ……….. 91
Results ………... 97
Discussion ………. 118
Case study 3 – Analyzing phase progression in Susan’s case Abstract ………. 125
Introduction ………... 126
The present study ……….. 133
xvii
Results ………... 139
Discussion ………. 153
CHAPTER III – Integrated discussion and final thoughts Integrated discussion on the sequence of phases proposed by the Paradigmatic Complementarity Metamodel ……….. 161
Article – Guidelines for reflective practice in psychotherapy: A reflection on the benefits of combining moment-by-moment and phase-by-phase mapping in clinical decision making ……….. 169
Implications, limitations and future research ………... 189
REFERENCES ……… 195
xix
LIST OF TABLES
Table 1 – Descriptives (Eva’s case) ………. 58
Table 2 – Descriptives (Lisa’s case) ……… 98
xx
Figure 2 – The evolution of patients’ capacity and therapists’ promotion
throughout the therapeutic process ……….. 23
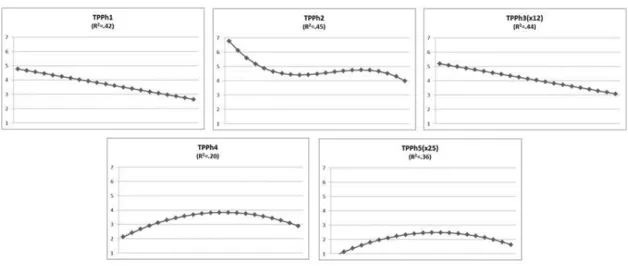
Figure 3 - Lines of evolution of therapist’s promotion and patient’s capacity of
the clinically relevant phases (Eva’s case) ………... 60
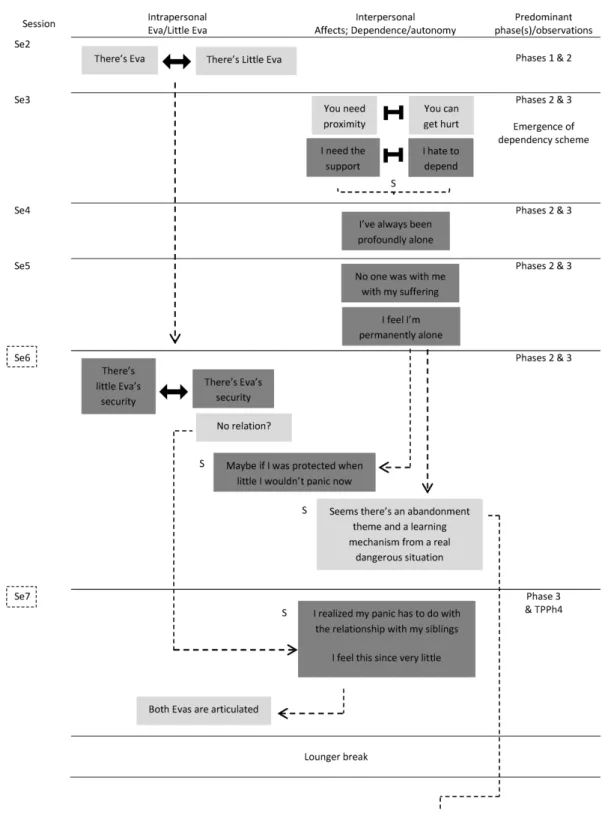
Figure 4 – The evolving process throughout the first year of Eva’s therapy ...…... 64
Figure 5 – Lines of evolution of therapist’s promotion and patient’s assimilation
of the clinically relevant phases that changed significantly throughout the
therapeutic process (Lisa’s case) ………. 100
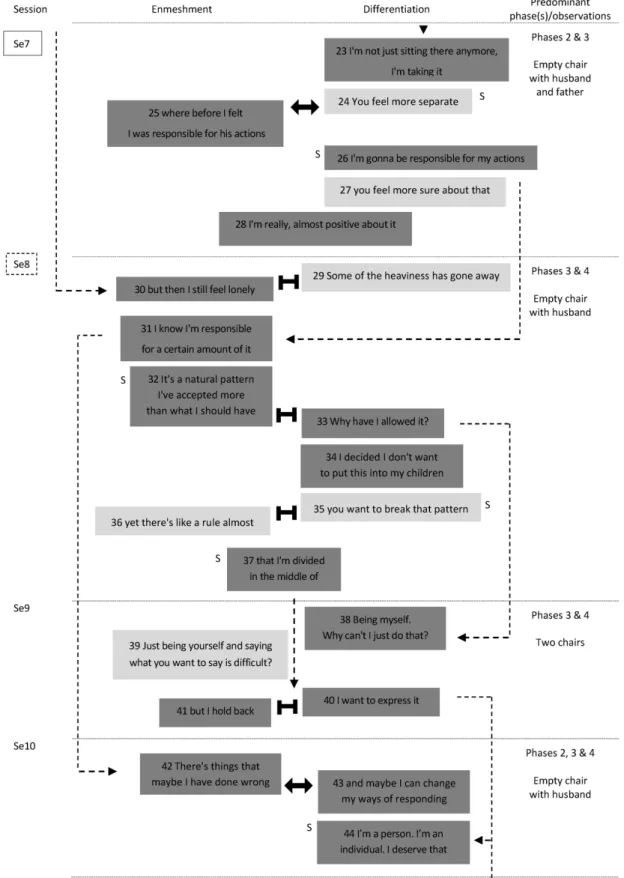
Figure 6 – The evolving process throughout Lisa’s therapy ………... 103
Figure 7 – Lines of evolution of therapist’s promotion of the clinically relevant
phases that changed significantly throughout the therapeutic process (Susan’s
case) ………. 142
Figure 8 - Lines of evolution of patient’s assimilation of the clinically relevant
phases that changed significantly throughout the therapeutic process (Susan’s
case) ………. 143
Figure 9 – Diagram for the evolution of each phase for patients’ capacity and
xxi
LIST OF ACRONYMS
DAPP – Developmental Analysis of Psychotherapy Process Method GSI – Global Severity Index
PCM – Paradigmatic Complementarity Metamodel SO(s) – Strategic Objective(s)
SOG – Strategic Objectives Grid S(s) – Session(s)
CHAPTER I
Introduction
1
“We are what each time we build of ourselves”
Adapted from Luigi Pirandello
The main aim of this research was to better understand the processes of change in psychotherapy, adding a phase-by-phase perspective to the analysis of the therapeutic process.
We conceive psychotherapy as a developmental process co-constructed by the patient and therapist, both moment-by-moment and phase-by-phase. Our emphasis in this research was to examine actual processes to explore whether and how a phase-by-phase perspective adds comprehensive value to the understanding of the therapeutic process and the practice of psychotherapy.
In the introduction, we quote several authors, sometimes extensively.
Because the quotes are so important and inspiring, we opted to keep them despite the fact some are quite long.
PRINCIPLES AND IDEAS OF PSYCHOTHERAPY IMPORTANT TO THIS STUDY
Psychotherapy as a developmental process
Basseches and Mascolo (2010) state “some form of development is the common outcome of all effective psychotherapy” (p.4). Taking inspiration from Kaplan’s
2
global and undifferentiated state to states of increasing differentiation, integration, and hierarchic integration” (Basseches & Mascolo, 2010, p.14).
According to this conceptualization, psychotherapeutic change is much more than symptom reduction or stabilization – it is a developmental process that aims to promote structural change. This is an idea defended not only by Basseches and Mascolo (2010) but also by Grande et al. (2009) who studied the long-term effects of therapy outcomes and found that, at the 3-year follow-up, patients attribute their therapeutic progress significantly more to structural than symptomatic changes.
Grande et al. (2009) define structural changes as particularly persistent effects (vs. more superficial changes like symptom reduction), concerned with changes in the “entire reference system within which the patient evaluates his or her experience and behavior” (p.345). Structural change is thus change at deeper levels of the personality, resulting in a more stable personality organization (Grande et al., 2009). They suggest that the gains of therapy are not the elimination of the internal conflicts (patients actually remain susceptible to them long after successful therapeutic processes), but rather the capacity to deal with these conflicts and find healthier solutions (Grande et al., 2009). The authors also consider that by changing the experience of self, structural change has an extended impact on many life domains and is “essential in attaining persistent therapeutic effects at all levels (e.g., also at the symptomatic level)” (Grande et al., 2009, p.345).
The idea that what changes with psychotherapy is the patients’ capacity to resolve their internal conflicts more than the elimination of the conflicts themselves (Grande et al., 2009) resembles Greenberg, Rice and Elliott’s (1993) concept of Process
3 predicts good therapeutic outcomes, but the work on how the patient is processing that content. They thus encourage therapists to make clinical decisions based on how the patients organize their experiences at each moment: “What we attempt to facilitate is change in the manner in which people are processing, change in both what they attend to and how they symbolize, rather than the modification or understanding of specific contents” (Greenberg et al., 1993, p.15).
Ferreira, Conceição and Vasco (2011) give an example of this focus on process rather than content. They suggest that if we know how to promote a patient’s capacity to transform self-criticism into self-acceptance, we can facilitate this process in other patients independently of the specific content of each patient’s self-criticism. It is a question of working at the level of the process of self-criticism rather than at the level of the content of it, even if we address the content while working the process.
The ideas of Piaget are also worth mentioning in this context. On the one hand, we have the priority given to structural knowledge over factual knowledge and his stages of change that reflect children’s structural development (Lourenço, 2005; Piaget, 1977). On the other hand, he developed the concept of equilibration, which is the pillar of his constructivist theory of development (Basseches & Mascolo, 2010; Lourenço, 2005; Piaget, 1977).
Inspired by this concept, Basseches and Mascolo (2010) say “developmental change is a process of equilibration. Thus the process of encountering and resolving disequilibrium brings about developmental change, and developmental change is reflected in the production of structures or organizations of activity that provide greater equilibrium” (p.31).
4
Equilibration, for Piaget, is acquired through the processes of assimilation and accommodation, where assimilation refers to the incorporation of something new to the
existing structure, and accommodation refers to the adaptation of the structure to what was incorporated (Achenbach, 1986; Basseches & Mascolo, 2010; Lourenço, 2005; Piaget, 1977). Vasco and Conceição (2008) and Conceição (2010) applied these concepts to the development of the therapeutic process and relate assimilation to the immediate and potentially occasional gains sustained at the therapist’s instigation (the patient’s consideration of something new), and accommodation to the solid and stable gains integrated in the patient’s repertoire and manifested even without the therapist’s prompting (the integration of the novelty into one’s being and acting). They warn that although assimilation is very important, it is not enough to structure or consolidate change, and therapists should be alert to whether patients are accommodating the assimilated novelties and how to favor this accommodation process in order to consolidate change (Conceição, 2010; Vasco & Conceição, 2008).
Inspired by sociocultural theories, Basseches and Mascolo (2010) bring another important consideration to our thinking about the developmental process of psychotherapy – “the developmental changes that occur in psychotherapy do not emanate from within the client; they occur as a product of processes that occur between the client and therapist” (p.38). Therapeutic change is thus co-constructed, patients internalize what they build while interacting with the therapist. This idea is also shared by Safran and Muran (2000) in their model Relational Psychotherapy, where they emphasize the importance of the therapeutic alliance to the therapeutic process and the patients’ development. Wachtel (2008) expands this idea from a two-person psychology perspective and his cyclical-contextual model, where he clarifies that patients are
5 immersed in context (the therapist being part of it) and they respond to it, they don’t evolve alone in isolation from their relational world. Thus, it is important to consider the impact on the patient of every part of his/her context, namely the therapist’s impact.
Psychotherapy Integration
The psychotherapy integration movement is another important base for this study.1
Norcross and Goldfried (2005) begin the Handbook of Psychotherapy Integration by stating that:
From its beginning, psychotherapy integration has been characterized by a dissatisfaction with single-school approaches and the concomitant desire to look beyond school boundaries to see what can be learned – and how patients can benefit – from other forms of behavior change. Improving the efficacy, efficiency, and applicability of psychotherapy is the raison d’être of integration. (p.v)
This movement reflects “a general decline in ideological struggle and the movement toward rapprochement” (Norcross, 2005, p.3). Norcross (2005) also explains the context that allowed this movement to evolve:
At least eight interacting, mutually reinforcing factors have fostered the development of integration in the past two decades:
1. Proliferation of therapies
2. Inadequacy of single theories and treatments
1 For the history of psychotherapy integration the reader is directed to Goldfried, Pachankis and
6
3. External socioeconomic contingencies
4. Ascendency of short-term, problem-focused treatments
5. Opportunity to observe various treatments, particularly for difficult disorders
6. Recognition that therapeutic commonalities heavily contribute to outcome
7. Identification of specific therapy effects and evidence-based treatments 8. Development of a professional network for integration. (p. 5)2
Thus, the integrative movement reflects the understanding that no single school can adequately explain adequately the whole of human functioning, that every school has something relevant to add to the understanding of human functioning and change, and even that different schools actually have many aspects in common that have more to do with therapeutic success than was initially expected.
Norcross (2005) and Gold and Stricker (2006) identify four paths to integration:
technical eclecticism – comprising the selection of interventions from different theories
that better adjust to the specific person or problem, and that can be used sequentially or in combination; – theoretical integration – where two or more therapies (and theories) are integrated and the emergent therapy is more comprehensive than the sum of its parts; – assimilative integration – where there’s still a predominant orientation but one that selectively incorporates ideas and practices from other approaches; – and common
factors – that looks for the ingredients that different therapies have in common and that
best contribute to therapeutic success across approaches.
7 Lambert (1992) and Lambert and Barley (2002)3 present a pie chart with the approximated percentages of the contributions of four therapeutic factors to improvements in psychotherapy. 40% is considered to be due to extra-therapeutic change – “those factors that are a part of the client (such as ego strength and other homeostatic mechanisms) and part of the environment (such as fortuitous events, social support) that aid in recovery regardless of participation in therapy” (Lambert, 1992, p.97) – 30% to common factors – “include a host of variables that are found in a variety of therapies regardless of the therapist’s theoretical orientation: such as empathy, warmth, acceptance, encouragement of risk taking, et cetera” (Lambert, 1992, p.97) – 15% to techniques – “those factors unique to specific therapies (such as biofeedback, hypnosis, or systematic desensitization)” (Lambert, 1992, p.97) – and another 15% to expectancy (placebo effects) – “that portion of improvement that results from the client’s knowledge that he/she is being treated and from the differential credibility of specific treatment techniques and rationale” (Lambert, 1992, p.97).
Norcross and Lambert (2011) present an additional pie chart where they add the approximated unexplained variance in psychotherapy outcome (40%) and redistribute the remaining explained 60% between patient contribution (30%), therapy relationship (12%), treatment method (8%), individual therapist (7%), and other factors (3%).
Common factors
The apparent larger influence of common factors in the therapy outcome (30%) over specific techniques (15%) stimulated the determination of the core ingredients present in any successful therapy and the reconsideration of previously “diminished”
8
aspects of the therapeutic process (such as relationship factors) as truly important and that need to be acknowledged, studied, developed and practiced (Duncan, Miller, Wampold & Hubble, 2010; Norcross, 2002, 2005). The ingredients typically recognized as part of every good therapy are the development of a therapeutic alliance, facilitation of hope, opportunity for emotional release, exploration and integration of one’s problems, support, advice, encouragement, acquisition and practice of new behaviors and clients’ positive expectancies (Lambert, 2013b; Norcross, 2005).
Hubble, Duncan, Miller and Wampold (2010) provide an important consideration regarding common factors:
In reality, the common factors are not invariant, proportionally fixed, or neatly additive. Far from it, they are interdependent, fluid, and dynamic. Unlike a manufacturing operation, with linear inputs and predictable outputs, therapy is a reciprocal process, in which the inputs are changed in and by the participants' interaction. In short, the role and degree of the influence of any one factor are dependent on the context: who is involved; what takes place between therapist and client; when and where the therapeutic interaction occurs; and ultimately, from whose point of view these matters are considered. (p.34)
What their consideration highlights is that it is not only the presence or absence of the common and important ingredients that lead to good outcomes, but how they are integrated and adjusted to each specific process and therapeutic relationship. So the idea of the co-construction of therapeutic change presented while elaborating on psychotherapy as a developmental process, and the importance of the therapeutic relationship that the common factors approach highlights are, once more, reinforced.
9 Additionally, the consideration of Huble et al. (2010) has links to the next section on principles of therapeutic change and the subsequent one on responsiveness.
Principles of therapeutic change
Still in light of the common factors perspective, a hugely important contribution to therapeutic integration and the main hallmark of one of the models at the base of this study came from Goldfried (1980):
In considering how one might approach the task of looking for points of commonality among different orientations, it might be helpful to conceptualize the therapeutic enterprise as involving various levels of abstraction from what is directly observable. At the highest level of abstraction we have the theoretical
framework to explain how and why change takes place, as well as an
accompanying philosophical stance on the nature of human functioning. In the search for commonalities, it is unlikely that we can ever hope to reach common ground at either the theoretical or the philosophical level. Indeed, numerous differences can be found at this level within the psychoanalytic, behavioral, and humanistic orientations. At the lowest level of abstraction, we have the therapeutic techniques or clinical procedures that are actually employed during the intervention process. Although commonalities across approaches may be found in the realm of specific techniques (e.g. role playing, relaxation training), it is unlikely that such comparisons would reveal much more than trivial points of similarity. I would suggest, however, that the possibility of finding meaningful consensus exists at a level of abstraction somewhere between theory and technique which, for want of a better term, we might call clinical strategies.
10
Were these strategies to have a clear empirical foundation, it might be more appropriate to call them principles of change. In essence, such strategies function as clinical heuristics that implicitly guide our efforts during the course of therapy. (p.994)
This movement from ingredients to principles of change, and looking for them at a strategic level, allowed the recognition or reinforcement that the therapeutic process must have purpose, or goals, and its outcome may be enhanced if the techniques/the specific interventions are guided by principles of change (Arkowitz, 2009; Beutler & Castonguay, 2006; Goldfried, 2009, 2014).
Along with guiding the selection of the techniques to apply at a specific moment or to a specific patient, Goldfried (2014) identified other important contributions of thinking on this strategic level:
Principles of change become particularly useful to ensure that therapy proceeds in the optimal fashion. When problems in therapy occur, such as when resistance and noncompliance occur, it is most useful clinically to review the various principles of change to see whether or not they are operating. Change principles thus can help to better understand problems in therapy progress when they occur, such as when there are ruptures in the therapy alliance or when motivation for change has waned. (p.277)
Beutler (2009) makes an interesting association of Goldfried’s (1980) higher and lower levels of abstraction to theoretical integration and technical eclecticism respectively, and suggests a movement toward strategic integration at this mid-level of
11 abstraction. He identifies two strategic integration approaches – Prochaska’s Transtheoretical Psychotherapy and his and Clarkin’s Systematic Treatment Selection. The sequential component of the Paradigmatic Complementarity Model, that we will expound upon later, is another example of strategic integration (Vasco, 2006; Vasco & Conceição, 2008).
Goldfried (1980) gives two examples of strategies common to different approaches: providing the patient with new corrective experiences and offering the patient direct feedback.
Responsiveness
In our view, a therapeutic principle that deserves to be highlighted is responsiveness.
Stiles, Honos-Webb, & Surko (1998) explain it clearly and beautifully. For instance they state that “human interaction is systematically responsive” (Stiles et al., 1998, p.439) and explain “in suggesting that psychotherapy is responsive, we mean that the content and process emerge as treatment proceeds, rather than being planned completely in advance. Thus, no two clients receive identical treatments, just as no two conversations are identical” (p.440). They alert us to recognize that behavior is affected by emergent context, if we fail to consider the context and just apply interventions without considering the immediate needs of the patient and process, we will probably fail to help the patient in front of us, even if the same interventions were very useful to a different patient or in a different moment (Stiles et al., 1998, Stiles & Shapiro, 1989).
12
Butler and Strupp (1986) share the same idea – “psychotherapy cannot be meaningfully reduced to "factors" independent of a particular interpersonal context” (p.31).
The significance of the procedure is not in the application of a disembodied technique but how the procedure becomes integrated into the ongoing interpersonal context of the particular dyad. In this sense, the procedures (techniques) and interpersonal factors are thoroughly intertwined and cannot be separated. (Butler & Strupp, 1986, p.33)
It is the capacity to be interpersonally responsive to the patient that permits the techniques to be effective. Similar to what the Paradigmatic Complementarity Model (Vasco 2001, 2006) argues, Butler and Strupp (1986) say:
How the therapist manages the interpersonal climate created with a particular patient becomes central to the question of skill and technique. It no longer makes sense to understand techniques as discrete operations or procedures that somehow alleviate disembodied conditions. Instead, skill and technique refer to efforts on the part of the therapist to influence the quality of the patient's experience in relation to the therapist as a significant other (…) Such efforts are founded on specifiable principles of human interaction which, in turn, suggest strategies that may take different manifest forms in different dyads. (p.36)
And Stiles et al. (1998) explain:
The therapist’s job is to monitor the situation and to choose a treatment that is appropriate for the client’s problems, follow a strategy that is appropriate for the
13 client’s capacity, and intervene with techniques that are appropriate for the client’s current state.
Appropriate responsiveness thus demands sensitivity to emerging client requirements. A therapist must, to some degree, recognize the client’s deficits (e.g., needs, problems) and resources (e.g., ability to make use of) as they emerge and must intervene in ways that take them into account. (p.440)
This idea of responsiveness at different levels of abstraction, integrating moment-to-moment needs to macro considerations of the patient’s problems and characteristics, are essential, we believe, to productive and consistent therapeutic gains. And if we believe (and research shows) that no one approach is necessarily better than another, a responsive therapist is definitely better than an unresponsive one and will better help his/her patients improve (Conceição, 2005, 2010; Stiles et al., 1998, Vasco & Conceição, 2008).
The responsiveness principle even helps clarify how important therapeutic ingredients work, like the ingredient alliance, which “is not a therapeutic technique but instead reflects the responsive use of techniques” (Stiles et al., 1998, p.448).
Change processes at different levels of abstraction
Change processes, at different levels of abstraction, are also important to discuss here.
With the advent of process research4, there was a change in researchers’ focus, from macro-outcomes – assessed at the end of therapy – to micro-outcomes – assessed
14
during the therapeutic process (Orlinsky & Howard, 1986). These micro-outcomes are “subtle but significant steps toward personal transformation” (Orlinsky & Howard, 1986, p.366). Orlinsky and Howard (1986) add:
Given unfavorable conditions in the patient’s life, successful micro-outcomes may dissipate before they can be consolidated into significant macro-outcomes. Under favorable circumstances, however, micro-outcomes should gradually accumulate over the course of therapy and be synthesized by the patient to change the habitual, problematic assumptive systems (schemata, scripts, programs) used in dealing with self and others. (p.367)
In this sense (and here lies the often hard and reductionist distinction between processes and outcomes) these micro-outcomes can be seen as change mechanisms or even change processes that promote the ultimate macro-outcomes (Marmar, 1990).
These micro-outcomes can be analyzed at different levels, from seconds, to minutes, to entire sessions, to groups of sessions, depending on the level of abstraction (Orlinsky, Ronnestad & Willutzki, 2004). So we can have moment-by-moment analyses (more at the micro level) and/or phase-by-phase analyses (more at the meso or intermediate level).
Doss’ (2004) concept of change mechanisms reflects these intermediate gains, while his concept of client change processes seems to reflect more micro changes, supposed to facilitate the change mechanisms. His concept of therapy change processes, in our view, can fall under the micro or meso level, as the therapist can facilitate the patient’s gains moment-by-moment, through direct interventions or, at a more intermediate and strategic level, through the principles of therapeutic change.
15 The idea of sequence5 is often related to change processes (e.g. Benjamin, 2003; Stiles et al., 1990). The organismic-developmental paradigm sustains that “major advances in psychological functioning are assumed to occur in a uniform sequence, with advanced levels depending on the prior emergence of less advanced levels” (Achenbach, 1986, p.120).
Lampropoulos (2001) for instance, organized the most frequently reported common factors in a time sequence in psychotherapy and change:
1. formation of a therapeutic relationship (bond, positive personal skills and qualities), and establishment of a working alliance (contract, goals, tasks);
2. accomplishment of catharsis and relief from distress (i.e. ‘emotional regulation’ via empathy, and support);
3. instillation of hope and raising of expectations (to actively engage client in therapy);
4. self-exploration, awareness, and insight into problems (feedback, reality testing);
5. provision of a theoretical explanation (rationale) for clients’ behavior and change (via interpretation, restructuring, reframing);
6. problem confrontation (exposure, working through, use of techniques);
7. acquisition and testing of new learning in and outside psychotherapy (behavioral–cognitive–experiential–interpersonal learning, via suggestion, persuasion, identification, modeling, etc.); and
5 Note that some authors defend dialectic or cyclical movements over sequential ones (e.g.
16
8. control over the problem and mastery of the new knowledge (self-attributions of change and self-efficacy enhancement; generalized use of the solutions; change maintenance and relapse prevention). (p.22)
Stiles et al. (1991) developed the Assimilation Model that sustains eight stages of assimilation of problematic experiences, from warded off, to unwanted thoughts, to
vague awareness, to problem statement/clarification, to understanding/insight, to application/working through, to problem solution, to mastery.
Benjamin (2003) in her Interpersonal Reconstructive Therapy, postulates five sequential steps in therapy: 1. collaboration, 2. Learning what the patterns are, where
they are from, and what they are for, 3. Blocking maladaptive patterns, 4. Enabling the will to change, and 5. Learning new patterns.
Vasco’s (2006) sequential component of the Paradigmatic Complementarity Metamodel is one more example of this sequencing of the therapeutic process that we explore later on.
This idea of sequence can be related to the idea of a phase-by-phase level of analysis. As therapeutic principles (meso) can orient therapeutic interventions (micro), “certain therapist interventions may also vary as a function of the phase of therapy” (Marmar, 1990, p.267). Vasco, Conceição and Ferreira (2014) and Basseches, Conceição and Ferreira (2014) highlighted the importance of articulating moment-by-moment and phase-by-phase levels of analysis, where the macro picture (phase-by-phase principles) orients the micro interventions, and the micro context (moment-by-moment changes and needs) feeds back to the macro picture of what the patients’ capacities and vulnerabilities are.
17 As the integrative movement in psychotherapy highlights, looking from only one perspective can be reductionist and misleading. Especially with more complex cases, it is important to be alert to the moment-by-moment nuances of the patient and the relationship, but at the same time, interventions should be planned bearing in mind also where the patient is in the process, what his/her capacities already are and his/her remaining vulnerabilities (Basseches et al., 2014; Vasco et al., 2014).
PSYCHOTHERAPY MODELS AT THE BASE OF THIS STUDY6
Temporal sequencing component of the Paradigmatic Complementarity Metamodel
The Paradigmatic Complementarity Metamodel (PCM) is a transtheoretical model inspired by the integrative movement in psychotherapy. It contemplates four components (Vasco, 2006): a) general principles of therapeutic change, b) the therapeutic alliance, c) the conceptualization of the patient and the problem, and d) a temporal sequence of phases regarding therapeutic goals.
This last temporal sequencing component of the PCM was inspired by Goldfried’s (1980) challenge to develop principles of therapeutic change at a strategic level, and is a product of a sequencing of common factors systematically identified in the literature as particularly important for therapeutic success.
So the PCM suggests a sequence of seven phases (seven therapeutic principles) that work on a strategic level, and each phase identifies five strategic objectives or general strategies to be promoted by the therapist, and developed by the patient (in a
18
kind of symmetry), and whose sequential prosecution fosters patients’ gradual progress along the therapeutic process (Vasco & Conceição, 2008; Vasco, 2001, 2006).
The phases of the model are:
Phase 1 - Trust, motivation, hope building and structuring; Phase 2 - Increasing awareness of self and experience; Phase 3 – Meaning-making regarding self and experience; Phase 4 - Regulation of responsibility;
Phase 5 - Implementation of repairing actions; Phase 6 - Consolidation of change; and
Phase 7 - Anticipation of the future and relapse prevention.
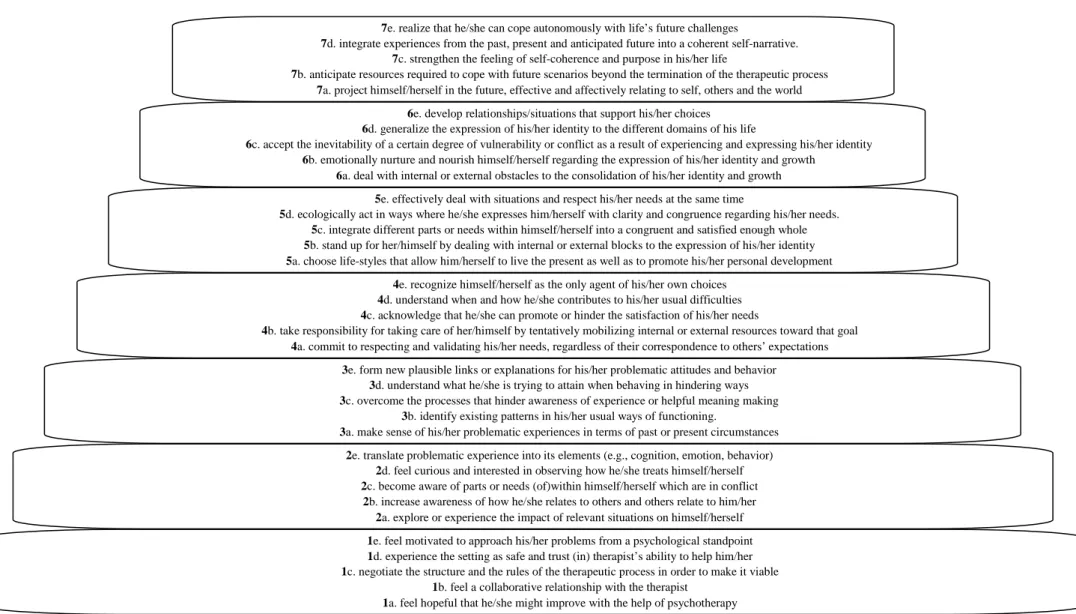
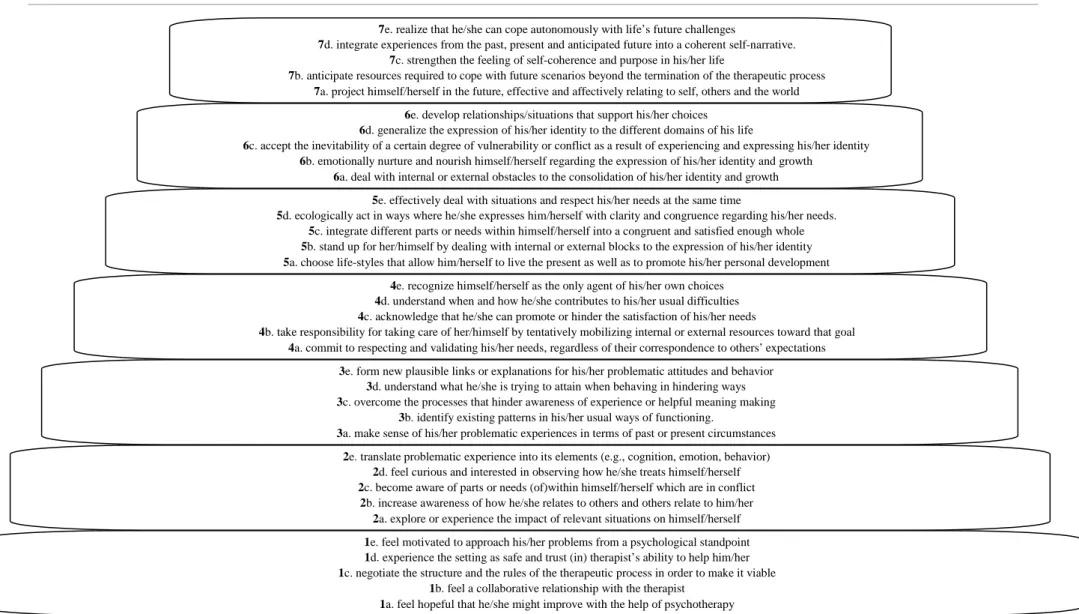
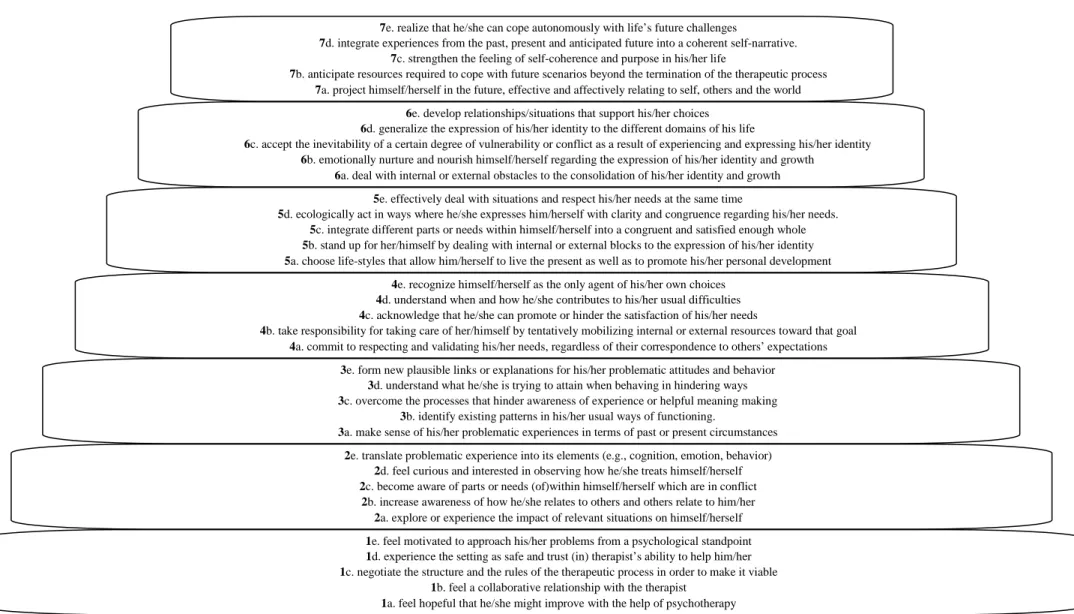
Figure 1 identifies the five strategic objectives of each phase that can be read both in light of what the therapist promotes and what the patient is supposed to assimilate (e.g. when working on the strategic objective 1a in Figure 1 the therapist
helps the patient to feel hopeful that he/she might improve with the help of psychotherapy and the patient assimilates the ability to feel hopeful that he/she might improve with the help of psychotherapy).
According to PCM, at this strategic/intermediate level of analysis, a micro vs. macro distinction can still be made. At a micro level, the therapist can promote general strategies associated with different phases in a single session, while at a macro level, he/she will predominantly stress one type of general strategy and give less emphasis to others. The concept of Phase is associated with this predominance of strategic work over several consecutive sessions from a more macro perspective (Conceição, 2010). At this macro level, things tend not to change so frequently as at the micro level.
19 1e. feel motivated to approach his/her problems from a psychological standpoint
1d. experience the setting as safe and trust (in) therapist’s ability to help him/her 1c. negotiate the structure and the rules of the therapeutic process in order to make it viable
1b. feel a collaborative relationship with the therapist 1a. feel hopeful that he/she might improve with the help of psychotherapy 2e. translate problematic experience into its elements (e.g., cognition, emotion, behavior)
2d. feel curious and interested in observing how he/she treats himself/herself 2c. become aware of parts or needs (of)within himself/herself which are in conflict
2b. increase awareness of how he/she relates to others and others relate to him/her 2a. explore or experience the impact of relevant situations on himself/herself 3e. form new plausible links or explanations for his/her problematic attitudes and behavior
3d. understand what he/she is trying to attain when behaving in hindering ways 3c. overcome the processes that hinder awareness of experience or helpful meaning making
3b. identify existing patterns in his/her usual ways of functioning.
3a. make sense of his/her problematic experiences in terms of past or present circumstances 4e. recognize himself/herself as the only agent of his/her own choices 4d. understand when and how he/she contributes to his/her usual difficulties 4c. acknowledge that he/she can promote or hinder the satisfaction of his/her needs
4b. take responsibility for taking care of her/himself by tentatively mobilizing internal or external resources toward that goal 4a. commit to respecting and validating his/her needs, regardless of their correspondence to others’ expectations
5e. effectively deal with situations and respect his/her needs at the same time
5d. ecologically act in ways where he/she expresses him/herself with clarity and congruence regarding his/her needs. 5c. integrate different parts or needs within himself/herself into a congruent and satisfied enough whole 5b. stand up for her/himself by dealing with internal or external blocks to the expression of his/her identity 5a. choose life-styles that allow him/herself to live the present as well as to promote his/her personal development
6e. develop relationships/situations that support his/her choices 6d. generalize the expression of his/her identity to the different domains of his life
6c. accept the inevitability of a certain degree of vulnerability or conflict as a result of experiencing and expressing his/her identity 6b. emotionally nurture and nourish himself/herself regarding the expression of his/her identity and growth
6a. deal with internal or external obstacles to the consolidation of his/her identity and growth 7d. integrate experiences from the past, present and anticipated future into a coherent self-narrative.
7c. strengthen the feeling of self-coherence and purpose in his/her life
7b. anticipate resources required to cope with future scenarios beyond the termination of the therapeutic process 7a. project himself/herself in the future, effective and affectively relating to self, others and the world
Figure 1. Paradigmatic Complementarity Phases Sequential Component, adapted from Vasco and Conceição (1998:2008). 1) Trust,
motivation, hope building and structuring; 2) Increasing awareness of self and experience; 3) Meaning making regarding self and experience; 4) Regulation of responsibility; 5) Implementation of repairing actions; 6) Consolidation of change, and 7) Anticipation of the future and relapse prevention.
20
As an integrative model that works at a strategic level, the sequential component of the PCM was developed to orient therapists regarding what kind of work to promote when, while leaving them room to choose whichever intervention from whatever approach they think best fits the patient and the goal they’re working toward. This is the same idea – to have principles orienting the techniques/interventions – suggested by Goldfried (1980, 2014).
The temporal sequencing component of the PCM suggests that, even if the patient needs to develop competencies from more advanced phases, therapeutic gains are more solid when the competencies of the previous phases are sufficiently grounded; steady gains (accommodation/capacity) are more important than sudden gains (assimilation), even if the latter may contribute to the former. This idea incorporates the concepts of assimilation and accommodation previously discussed under the section
Psychotherapy as a developmental process and follows the responsiveness principle of
Stiles et al. (1998).
Inspired by this responsiveness principle, the sequencing component of the PCM supports the importance of integrating the therapist’s promotion of general strategies with the patient’s capacity to process those interventions. It is useful to ask two questions: a) what is the therapist predominantly promoting at each session and b) has he/she considered whether the patient is adequately capable of receiving and processing it. For example, a therapist who wants to help a patient give meaning to his/her problematic experiences (phase 3 work) must consider whether the patient is sufficiently aware of these problematic experiences, and how they are part of his/her life (which would be phase 2 gains). Without phase 2 capacity, phase 3 work would not be productive. These considerations inform the therapist whether the patient needs to
21 proceed to the work of subsequent phases or whether he/she needs to consolidate the work of the current phase or even of a previous one (Conceição, 2005, 2010).
The PCM does not argue for a rigid sequence that all therapists should follow; the intention is mainly to provide a structural responsiveness map, an orientation tool to use during the therapeutic process. This serves to alert the therapist to check which point the patient is at regarding his/her processing capacities, and not to rush too quickly to work on strategic objectives regarding more advanced phases if the patient is not yet ready.
An important stimulus to develop this sequence was the day-to-day work done with patients with personality disorders. We feel this sequence is particularly important when working with patients such as these, since they tend to be particularly sensitive to misattunements and to lack of responsiveness from their therapists. They also tend to need more time and skills to attain therapeutic goals.
The sequencing component of the PCM has been studied for the last 14 years with both transversal and longitudinal analyses. Previous studies have systematically a) supported a temporal sequence of strategic objectives (Conceição, 2005, 2010; Vasco, 2006), b) shown the potential of this sequence in intervening with personality disorders in long-term processes (Conceição, 2010; Gonçalves & Vasco, 2001; Rodrigues, 2012), c) pointed to an increase of the estimated improvements of the patient as he/she progresses along the therapeutic process (Vasco, 2006), and d) indicated that the articulation of therapist’s work according to client's assimilation capacity may be associated with good outcomes and better alliances at least regarding the task agreement dimension (Conceição, 2005, 2010).
22
The studies have also systematically shown that patients’ capacities tend to evolve sequentially and cumulatively along the process. Regarding therapists’ promotion of strategic objectives at a micro level, we notice more back and forth movements. Even so, a sequence is also found when analyzing what the therapist is predominantly promoting at a more macro level: he/she seems to promote mainly one phase and the adjacent phases, and when moving forward tends to give up the work of previous phases in favor of subsequent ones (Conceição, 2005, 2010; Ferreira et al., 2011; Vasco, 2006). Figure 2 illustrates the evolution of patients’ capacity and therapists’ promotion (Vasco & Basseches, 2013; Vasco et al., 2014).
Recent studies have shown qualitative evidence of this phase-by-phase temporal sequencing of therapeutic gains, with excerpts from patients’ discourse illustrating markers of acquired processing capacities (Ferreira et al., 2011; Rodrigues, 2012, Simões, 2012). These studies involve qualitative analyses of the cases that Conceição (2010) studied in quantitative terms. The four studies together constitute an integration of quantitative and qualitative evidence supporting the temporal component of the PCM.
The Developmental Analysis of Psychotherapy Process (DAPP) Method
The DAPP is an approach aimed at analysing and understanding therapeutic dialogue and interaction. Therapy is conceptualized as a developmental process which proceeds by the differentiation and integration of activities and meanings within relational contexts. The method tries to clarify, on a moment-by-moment basis, what resources therapists bring to the therapeutic process, and whether and how patients are using those resources in the service of developmental transformation.
23
Figure 2 – The evolution of patients’ capacity and therapists’ promotion throughout the
therapeutic process.
As a dialectical perspective, the DAPP framework tracks micro-developmental movements through sequences of three steps, or moments: 1) differentiation of antitheses from theses, 2) holding in the attentional field conflicts among theses and antitheses; and 3) constructing “novel” syntheses that integrate and organise
24
differentiated theses and antitheses. A completed DAPP analysis begins by identifying the emergence of conflicts between different ideas, feelings, behaviors and experiences – all understood as aspects of human activity – within the therapeutic dialogue. It ends by determining whether and how novel syntheses of these are co-constructed through three distinguishable relational processes. These processes, described below, are distinguished by the type of resources therapists offer and that patients use in their developmental processes.
Similar to the responsiveness principle of Stiles et al. (1998), the DAPP suggests that to clarify how therapists and patients co-construct syntheses, which taken together represent therapeutic gains, and to distinguish developmental movement within the therapeutic process from blockage of such movement, it is important to ask three questions: a) what resources are therapists offering to patients?; b) how are patients receiving and using these resources?; and c) are therapists addressing whether patients are able to use the offered resources effectively, and adapting their offerings to patients’ capacities to use them?
The authors distinguish three broad types of therapeutic resources, each of which potentially leads to co-construction of novel syntheses in different ways. Attentional Support, whereby therapists help patients bring to and hold in their attentional field as wide a range of their own actions, experiences and reflections as possible, as well as the conflicts among them. This boosted attention fosters patients’ construction of novel syntheses. Interpretation, whereby therapists offer their own point of view to the patients as antitheses to the patients’ own understanding, and then therapists and patients work together to construct syntheses which integrate antithetical understandings. And Enactment, whereby therapists evoke, direct or promote patients’
25 novel actions and experiences, which then function as antitheses to patients’ prior repertoires, creating conflicts which can be transcended through novel syntheses. Although the terms above may be associated with different therapeutic traditions (e.g.,
Attentional Support with client-centred practice, Interpretation with traditional
psychoanalytic practice, and Enactment with behavioural and relational psychoanalytic practice), Basseches and Mascolo (2010) conceptualise these processes very broadly as “genotypes” and describe the wide range of phenotypic forms they tend to take in the contexts of different therapeutic approaches. They further claim, and illustrate through case analyses, that while therapeutic approaches may be differentiated in part by the degree of emphasis placed on these relational processes, these processes characterize “psychotherapy” in general, and all successful therapy depends on the integration of all three processes.
One tool of DAPP analysis is the Relational Activity Diagram that depicts therapeutically important movements and clarifies what happens in the therapeutic process that fosters (or hinders) developmental progression and outcomes. These diagrams combine the identification of a) micro-developmental steps (theses➔ antitheses, holding conflict, and constructing syntheses) and b) forms of therapeutic resources offered, with c) the analysis of co-constructive patterns between therapist and patient (i.e., which party tends to differentiate antitheses from theses, who tends to articulate statements that hold conflict, and who tends to first offer novel syntheses).
The DAPP was first developed between 2000 and 2002 and is based on two theoretical papers by Basseches (1997a, 1997b). For the last 13 years it has been used to study case material representing 15 different approaches to therapy, including Cognitive-Behaviour Therapy (Peters & Basseches, 2009), Short Term
Anxiety-26
Regulating Dynamic Therapy (Basseches & Mascolo, 2010), Emotion-Focused Therapy (Basseches & Dangelo-Perruci, 2011), and Couples Therapy from an Adlerian Perspective (Alvarez, Clapp, Basseches, Smidt, & Thomas, 2012), to name a few.
RESEARCH PRINCIPLES AND METHODOLOGIES IMPORTANT TO THE PRESENT STUDY
Process Research7
Elliott (2010) defines Process Research as “the study of the processes by which change occurs in psychotherapy, including both the in-therapy processes that bring about change and the unfolding sequence of client change (which changes occur first and lead to what subsequent client changes)” (p.123). Similarly, Basseches and Mascolo (2010) suggest adopting a developmental perspective for psychotherapy research which “provides a framework within which practitioners, theorists, and researchers can examine both the structural changes that occur in psychotherapy and the therapeutic
processes through which those changes come about” (p.25).
Thus, process research aims, nowadays, to study the relation between process and outcome instead of keeping them apart, especially as the distinction between the two is frequently blurred (Beutler, 1990; Hill & Corbett, 1993; Marmar, 1990; Stiles & Shapiro, 1989). As Knobloch-Fedders, Elkin and Kiesler (2014) state:
The change process paradigm emphasizes that the dichotomy between process and outcome must be transcended by focusing directly on change events occurring within sessions. In this paradigm, process measures are used not
7 For the history of Process Research the reader is reported to Hill and Corbett (1993) and
27 simply to describe what happens in psychotherapy sessions or to predict outcome, but to understand how change comes about. (p.4)
A further important consequence of adopting a developmental perspective and relating process and outcome is the movement from a focus on symptom reduction to a complementary focus on patients’ structural transformation. Basseches and Mascolo (2010) state:
The goal of promoting and analyzing psychological development directs the attention of practitioners, theorists, and researchers to the (positive) formation of novel structures of acting, thinking, and feeling as well as to the (negative) observations of symptom reductions that may result from such restructuring. By focusing upon what develops in psychotherapy in addition to what goes away, one is not only able to provide a richer analysis of the processes by which psychological “symptoms” are or are not mitigated, but also able to explore the ways in which psychotherapy and related social processes foster construction of more adequately organized forms of psychological and social functioning. (p.26)
Process research also has the potential to approximate researchers and clinicians and be more useful with regard to the clinical decisions of the latter. Stiles and Shapiro (1989), nonetheless, alert us to the abuse of what they call “the drug metaphor” even in process research, manifested, for example, in the search for active ingredients that therapists should provide, instead of stimulating responsiveness to patients’ needs, or trying to specify the best treatments and procedures, instead of contemplating the multitude of possible paths and goals to therapeutic success. Butler and Strupp (1986)
28
explain “the goal of psychotherapy research is shifted from the search for active ingredients toward efforts to understand how therapist qualities interact with patient characteristics to produce, or fail to produce, the interpersonal conditions necessary for therapeutic change” (p.30).
Greenberg (1991) provides another important consideration that suggests we have been concerned with finding general laws for psychotherapy and human change whereas specific models (context specific laws) would be more realistic and comprehensive.
Related to this consideration, Greenberg (1991) also suggests a third research approach (one that transcends the two opposing approaches – correlational and experimental) which he calls process analytic and “involves a study of in-situation performance” (p.7). Process research should imply a comprehensive analysis of what is going on throughout the therapeutic process. To engage in this third approach, Greenberg (1991) explains that “we need to adopt a combined rational-empirical methodology, as opposed to a purely rational or purely empirical approach” (p.9). This idea is similar to Shoham-Salomon’s (1990) suggestion of integrating theory-driven and discovery-oriented research in a “cyclical approach whereby inductive inquiry [discovery-oriented] feeds deductive research [theory-driven], which in turn guides induction in an ongoing circle of mutual enrichment” (p.300).
These ideas are linked to two important concepts: theory-building research and methodological pluralism.