1. Health Ministry Erzurum Regional Training and Research Hospital, Dermatology, Erzurum/ TURKEY
2. Ataturk University School of Medicine, Rheumatology, Erzurum/TURKEY
What affects the quality of life in
patients with Behcet’s disease?
ACTA REUMATOL PORT. 2014:39;46-53
AbstrAct
Aim: The aim of this study was to evaluate the possi-ble associations between quality of life (QoL) and so-ciodemographic features, disease characteristics and the Behcet’s Disease (BD) disease activity of the patients with BD.
Patients and Methods: One hundred and seven pa-tients with BD were included in this study. Sociode-mographic features including age, gender, education level of the patients and the disease characteristics in-cluding disease duration, disease onset age, the histo-ry BD clinical involvements were recorded. In patients with BD, the BD Current Activity Form was used for the evaluation of disease activity. The short form-36 (SF-36) QoL scale was used to evaluate the QoL in pa-tients with BD. The Student t test, analysis of variance and Spearman’s correlation matrix were used for the statistical analysis.
Results: Men showed higher mean scores of role-phy-sical and bodily pain domains of SF-36 than women did (p <0.000 and 0.001). Patients over 41 years of age had higher mean general health scores and university graduates patients had higher mean mental health sco-res than the other groups (p <0,01). Patients with a di-sease duration more than 5 years and patients have a younger disease onset age showed lower general health score than the others (p <0,01). Also patients with an anamnesis of uveitis, genital ulceration, erythema no-dosum, thrombophlebitis, joint and gastrointestinal system involvement showed lower QoL than the pa-tients without these complaints (p <0,05 and p <0,01). In the analysis of disease activity physical subscores of SF-36 were found to be correlated with fatigue, oral
ul-Mehmet Melikoğlu1, Meltem Alkan Melikoglu2
ceration and joint involvement (p <0,01). Bodily pain showed a correlation with fatigue, headache and more highly with joint involvement (p <0,01 and p <0,001 respectively). General health was correlated with GIS and eye involvement and vitality was found to be cor-related with fatigue, patient’s and doctor’s impression of disease activity (p <0,01). Mental and emotional scores were correlated with oral- genital ulceration, eye and joint involvements (p <0,01).
Conclusion: In addition to demografic features and cli-nical involvements, BD disease activity can affect QoL in patients with BD. These results highlight the impor-tance of managing the symptoms and the disease acti-vity effectively in order to improve QoL in BD.
Keywords: Behcet’s Disease; Quality of life; Disease activity.
IntroductIon
Behçet’s disease (BD) is a vasculitis described by Turkish physician Hulusi Behçet in 1937 as a triple-symptom complex consisting of apthous ulcers of the mouth and
genital and relapsing uveitis1. In addition to the typical
triad, BD may involve cardiovascular, pulmonary, neu-rological, articular, and gastrointestinal systems. As a chronic multisystem disorder, it may cause a variety of clinical problems leading to temporary or permanent
functional disability2. The symptoms may be separated
by long or short intervals, occur simultaneously or in sequence, and exhibit a pattern of exacerbation and re-mission. They not only affect the physical and mental health of patients negatively, but they also affect their quality of life (QoL) by causing several physical im-pairments. QoL can be defined as it encompasses being able to satisfy one’s own basic needs, being satisfied with life, showing an adequate level of social interac-tion, allocating time to fun, feeling good emotionally
and physically, being good at interpersonal relation -ships, having self-esteem as well as previous
expe-riences3. Evaluations of health related QoL could assist
the optimal approach to the patient with a better un-derstanding of the behaviors and the psychological reactions of the patients as well as the difficulties they experience with adjusting to the disease and
develo-ping effective codevelo-ping mechanisms4. In recent years,
there has been a growing interest in the assessment of QoL, particularly in chronic disabling conditions, in-cluding BD. Since BD negatively affects patients phy-sically, mentally and socially, decrease in the QoL sig-nificantly may be expected in patients with BD related to these conditions. Previous studies have shown that QoL in patients with BD was negatively affected by the
disease itself or by the impact of the symptoms4-8.
The aims of this study were; to evaluate the asso-ciation between QoL and sociodemographic features of the patients (age, gender, education level); the disease characteristics (disease duration, disease onset age, cli-nical involvements) and the BD disease activity.
pAtIents And methods pAtIents
One hundred and seven patients with BD who fulfil-led the criteria of the International Study Group for BD were included in this study after obtaining the
in-formed consent from all participants9. Patients with
psychosomatic or psychiatric disorders and any other chronic diseases were excluded from the study. Also dependence on alcohol or other substances and any psychotropic drug usage were considered as exclusion criteria.
clInIcAl Assessments
For the evaluation of the sociodemographic features, age, gender, education level of the patients were re-corded. Also the disease characteristics including di-sease duration, didi-sease onset age, the history BD clinical involvements (uveitis, oralgenital ulceration, ery -thema nodosum, thrombophlebitis, pustules, arthral-gia, arthritis, major vessel involvement, gastrointestinal and central nervous system involvement) were inves-tigated. In patients with BD, the BD Current Activity Form (BDCAF), which scores the history of clinical features have been present during the 4 weeks prior to the day of assessment, was used for the evaluation of
disease activity10. With this activity form, fatigue,
hea-dache, oral-genital ulceration, skin lesions, joint in-volvement, gastrointestinal system inin-volvement, cen-tral nervous system involvement, major vessel invol-vement, patient’s impression of disease activity (last 28 days and the same day) and doctor’s impression of di-sease activity were evaluated in our study. A Turkish version of BDCAF has been tested and validated for our
population11.
Also, the short form-36 (SF-36) QoL scale was used to evaluate the QoL in patients with BD. This scale is one of the best known and most widely used QoL ins-truments that have been used in a wide range of disea-ses. It consists of 8 subcategories: (a) Physical Func-tioning (10 items), (b) Social FuncFunc-tioning (2 items), (c) Role Physical (4 items), (d) Role Emotional (3 items), (e) Mental Health (5 items), (f) Vitality (4 items), (g)
Bo-dily Pain (2 items), (h) General Health (5 items)12. The
score can range from 0 to 100, where 0 and 100 stood for the lowest and highest QoL respectively. The scale was evaluated taking the last 4 weeks into account. A Turkish version of the scale has been validated for our
population13.
stAtIstIcAl AnAlysIs
All statistical analysis was performed using the SPSS 20.0 software package program. The Student t test, ana-lysis of variance and Spearman’s correlation matrix were used to compare the data and to evaluate the pos-sible correlations between the scores of disease activi-ty and QoL. Statistical significance was determined at p<0.05.
results
After exclusion of five patients due to tyroid dysfunc-tion and antidepressant usage, one hundred and two patients with BD were evaluated in this study.
The QoL scores of the patients were investigated and the means and standard deviations for the SF-36 QoL subscales were calculated as follows: physical function 60,22±18,26; role-physical 44,70 ±17,79; bodily pain 47,70±24,12; general health 47,74± 21,27; vitality/ /fatigue 39,98± 21,28; social function 62,24±24,26; role-emotional 32,02± 18,42 and mental health 49,92± 13,22.
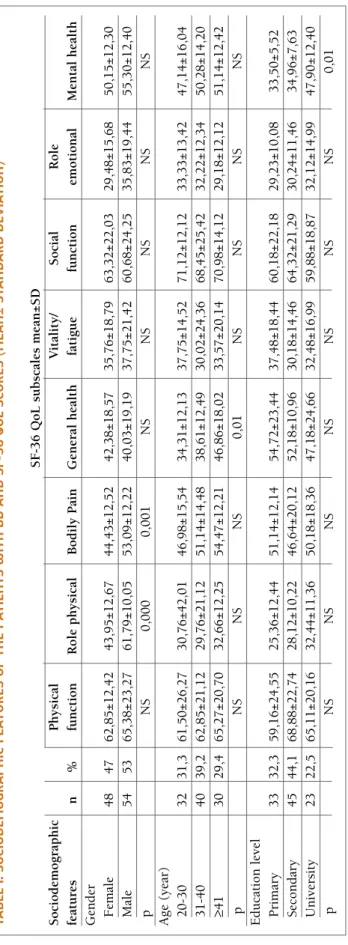
socIodemogrAphIc feAtures
The age, gender and education level were analyzed as sociodemographic features of the patients. There were
48 female and 54 male patients. Men showed higher mean scores of role-physical and bodily pain than wo-men did (p <0.000 and 0.001 respectively). The age range of the patients was 20 and 51 years (35,01± 7,85 year± SD). 32 patients were between 20 and 30 years of age, 40 patients were between 31-40 years of age and 30 were 41 or older. Patients over 41 years of age had a higher mean general health score than other age groups (p < 0.01). The education levels were primary school for 33 patients, secondary school for 45 and university for 23 patients. University graduates had a higher mean mental health score than the other groups while other groups had similar scores (p <0, 01). The sociodemographic features and SF-36 QoL scores of the patients were showed in Table I.
dIseAse chArActerIstIcs
The disease characteristics including disease duration, disease onset age, and the history BD clinical involve-ments were investigated. The disease duration of the patients was 84, 20 ± 48, 37 months with a range 24 and 240 months. Patients with disease duration more than 5 years showed significantly lower general health scores than the other patients (p <0,01). Also disease onset age of the patients was ranged from 17 to 40 year-old (28,15± 5,63 year-old) and patients have a younger disease onset age showed lower general health score than the others (p < 0.05). The history of pre-vious BD clinical involvements was investigated by yes or no questions. With this evaluation, all patients had current oral ulcers or previous oral ulceration history due to the classification criteria used. 32 patients had genital ulceration, 30 patients had uveitis, 50 patients erythema nodosum, 44 patients had thrombophlebi-tis, 50 patients had pustules, 28 patients had joint volvement, 13 patients had gastrointestinal system in-volvement, 5 patients had major vessel inin-volvement, and 5 patients had central nervous system involvement (current or previous involvements). Since oral ulcera-tion history was present in all patients and involve-ments of major vessels and central nervous system were present only in a few patients, we did not evaluate the significance of QoL in these patients. The other di-sease characteristics and SF-36 QoL scores of the pa-tients were showed in Table II.
dIseAse ActIvIty
The disease activity of the patients with BD and its re-lation with QoL were also evaluated. Physical function and role physical scores were found to be correlated
with fatigue, oral ulceration and joint involvement (p<0,01). Bodily pain component showed a correla-tion with fatigue, headache and more highly with joint involvement (p<0,01 and p<0,001 respectively). Ge-neral health was correlated with GIS and eye involve-ments and vitality was found to be correlated with fa-tigue, patient’s and doctor’s impression of disease acti-vity (p<0,01). In addition to mental health and eye in-volvement correlation, role emotion and mental health scores were also showed a correlation with oral- geni-tal ulceration and joint involvement (p<0,01). Since there were only a few patients with major vessel in-volvement and central nervous system inin-volvement in our study, they were not included in analysis. The re-lation with the other scores of BDCAF and SF-36 subs-cores were shown in Table III.
dIscussIon
In recent years, QoL assessment has became a valua-ble component of the evaluation process of a patient especially in chronic disabling conditions. To deter-mine the factors impair the QoL of a patient with a chronic condition may help in the management of the disease. Most previous studies have shown that BD may decrease the QoL of the patients by affecting them
physically, mentally and socially4-7. These
investiga-tions have revealed the impact of several features of BD on QoL. In this study, we investigated the factors affect the QoL in patients with BD. As possible related factors to QoL in BD, we analysed the sociodemo-graphic features, disease characteristics and disease ac-tivity of the patients.
In sociodemographic features we found significant differences in groups created according to gender, age and education levels of the patients. Role physical and bodily pain subscores of SF-36 QoL scale were signi-ficantly lower in female patients than the male ones. These results found to be similar with previous studies showing more impaired pain and physical QoL sub
-scores in female patients with BD4,6,14. This difference
between men and women could be attributed to the different gender roles, physiological and hormonal dif-ferences or different coping strategies for living with
BD2,15. Patients more than 41 years of age were found
to have higher scores of general health than the youn-ger groups in our study. This result may contribute the previous studies indicate that BD may be less severe as
tA b le I. s o cI o d em o g r A p h Ic f eA tu r es o f th e p A tI en ts w It h b d A n d s f-3 6 Q o l sc o r es ( m eA n ± st A n d A r d d ev IA tI o n ) S F -3 6 Q o L s u b sc al es m ea n ± S D S o ci o d em o g ra p h ic P h y si ca l V it al it y / S o ci al R o le fe at u re s n % fu n ct io n R o le p h y si ca l B o d il y P ai n G en er al h ea lt h fa ti g u e fu n ct io n em o ti o n al M en ta l h ea lt h G en d er F em al e 4 8 4 7 6 2 ,8 5 ± 1 2 ,4 2 4 3 ,9 5 ± 1 2 ,6 7 4 4 ,4 3 ± 1 2 ,5 2 4 2 ,3 8 ± 1 8 ,5 7 3 5 ,7 6 ± 1 8 ,7 9 6 3 ,3 2 ± 2 2 ,0 3 2 9 ,4 8 ± 1 5 ,6 8 5 0 ,1 5 ± 1 2 ,3 0 M al e 5 4 5 3 6 5 ,3 8 ± 2 3 ,2 7 6 1 ,7 9 ± 1 0 ,0 5 5 3 ,0 9 ± 1 2 ,2 2 4 0 ,0 3 ± 1 9 ,1 9 3 7 ,7 5 ± 2 1 ,4 2 6 0 ,6 8 ± 2 4 ,2 5 3 5 ,8 3 ± 1 9 ,4 4 5 5 ,3 0 ± 1 2 ,4 0 p N S 0 ,0 0 0 0 ,0 0 1 N S N S N S N S N S A g e (y ea r) 2 0 -3 0 3 2 3 1 ,3 6 1 ,5 0 ± 2 6 ,2 7 3 0 ,7 6 ± 4 2 ,0 1 4 6 ,9 8 ± 1 5 ,5 4 3 4 ,3 1 ± 1 2 ,1 3 3 7 ,7 5 ± 1 4 ,5 2 7 1 ,1 2 ± 1 2 ,1 2 3 3 ,3 3 ± 1 3 ,4 2 4 7 ,1 4 ± 1 6 ,0 4 3 1 -4 0 4 0 3 9 ,2 6 2 ,8 5 ± 2 1 ,1 2 2 9 ,7 6 ± 2 1 ,1 2 5 1 ,1 4 ± 1 4 ,4 8 3 8 ,6 1 ± 1 2 ,4 9 3 0 ,0 2 ± 2 4 ,3 6 6 8 ,4 5 ± 2 5 ,4 2 3 2 ,2 2 ± 1 2 ,3 4 5 0 ,2 8 ± 1 4 ,2 0 ≥4 1 3 0 2 9 ,4 6 5 ,2 7 ± 2 0 ,7 0 3 2 ,6 6 ± 1 2 ,2 5 5 4 ,4 7 ± 1 2 ,2 1 4 6 ,8 6 ± 1 8 ,0 2 3 3 ,5 7 ± 2 0 ,1 4 7 0 ,9 8 ± 1 4 ,1 2 2 9 ,1 8 ± 1 2 ,1 2 5 1 ,1 4 ± 1 2 ,4 2 p N S N S N S 0 ,0 1 N S N S N S N S E d u ca ti o n l ev el P ri m ar y 3 3 3 2 ,3 5 9 ,1 6 ± 2 4 ,5 5 2 5 ,3 6 ± 1 2 ,4 4 5 1 ,1 4 ± 1 2 ,1 4 5 4 ,7 2 ± 2 3 ,4 4 3 7 ,4 8 ± 1 8 ,4 4 6 0 ,1 8 ± 2 2 ,1 8 2 9 ,2 3 ± 1 0 ,0 8 3 3 ,5 0 ± 5 ,5 2 S ec o n d ar y 4 5 4 4 ,1 6 8 ,8 8 ± 2 2 ,7 4 2 8 ,1 2 ± 1 0 ,2 2 4 6 ,6 4 ± 2 0 ,1 2 5 2 ,1 8 ± 1 0 ,9 6 3 0 ,1 8 ± 1 4 ,4 6 6 4 ,3 2 ± 2 1 ,2 9 3 0 ,2 4 ± 1 1 ,4 6 3 4 ,9 6 ± 7 ,6 3 U n iv er si ty 2 3 2 2 ,5 6 5 ,1 1 ± 2 0 ,1 6 3 2 ,4 4 ± 1 1 ,3 6 5 0 ,1 8 ± 1 8 ,3 6 4 7 ,1 8 ± 2 4 ,6 6 3 2 ,4 8 ± 1 6 ,9 9 5 9 ,8 8 ± 1 8 ,8 7 3 2 ,1 2 ± 1 4 ,9 9 4 7 ,9 0 ± 1 2 ,4 0 p N S N S N S N S N S N S N S 0 ,0 1 N S : n o t si g n if ic an t
significantly higher mental health scores in university graduates patients than the others similar with another study’s results about QoL
in patients with BD4. It might be due to be more
aware about the disease course or higher so-cioecenomical status.
We also analysed the disease characteristics itself as posible factors related to QoL in BD. Due to the younger disease onset age and lon-ger disease duration parameters related to lo-wer general health score, it may be thought that chronicity in BD may contribute the impaire-ment of QoL. Also we investigated the current or previous BD clinical involvements as possi-ble related factors in QoL in patient with BD. In several previous studies QoL in BD was found to be affected by oro-genital ulcers
es-pecially in emotional and social aspects4,18,19.
We could not compare the patients with or wi -thout oral lesion history in our study since all patients had oral ulceration anamnesis due to the diagnosis criteria. However, similar to pre-vious studies we also found impaired emotio-nal and mental scores in patients with current or previous genital ulceration. Although there was no significant difference between QoL subscores of patients with or without pustular lesions, we also determined lower social func-tion scores in patients with erythema nodosum and lower physical function scores in patients with thrombophlebitis. Parallel with our re-sults, previous studies investigating the cuta-neous manifestations of BD indicated that oral and genital ulcers not only cause deterioration in personal relationships but also have an im-portant impact in the limitation of QoL in
pa-tients6,8,18,20. This may be due to the negative
ef-fect of oral lesions on motor functions such as speaking, swallowing and chewing, and nega-tive effect of genital lesions on extension of pain, perception of self-image and diminished
sexuality6,21.
In our study we also demontrated lower sco-res of physical function, social function and bo-dily pain in patients with articular involve-ment. Previous studies also showed that joint involvement in BD affects considerably pa-tients’ QoL due to pain, swelling and
move-ment difficulties4,6,7,22. Uveitis as one of the
tA b le II . d Is eA se c h A r A ct er Is tI cs A n d s f-3 6 Q o l sc o r es o f th e p A tI en ts SF -3 6 Q o L s u b sc al es M ± S D D is ea se P h y si ca l V it al it y / S o ci al R o le ch ar ac te ri st ic s n % fu n ct io n R o le p h y si ca l B o d il y P ai n G en er al h ea lt h fa ti g u e fu n ct io n em o ti o n al M en ta l h ea lt h D is ea se d u ra ti o n 0 -5 y ea r 3 0 2 9 ,4 3 3 ,5 7 ± 2 4 ,3 4 7 0 ,1 0 ± 2 4 ,5 9 5 5 ,5 6 ± 2 6 ,3 7 4 4 ,3 6 ± 1 7 ,1 7 3 7 ,2 3 ± 2 1 ,2 5 6 5 ,3 8 ± 2 4 ,8 5 2 9 ,3 6 ± 1 5 ,2 3 4 7 ,2 3 ± 1 6 ,3 3 6 -1 0 y ea r 2 9 2 8 ,4 3 5 ,7 6 ± 1 8 ,7 4 6 6 ,5 7 ± 2 2 ,1 3 4 9 ,2 3 ± 2 4 ,2 1 3 8 ,1 0 ± 1 5 ,1 1 3 0 ,2 1 ± 2 3 ,3 4 6 2 ,4 5 ± 2 2 ,1 4 3 3 ,3 3 ± 1 9 ,4 4 5 0 ,4 2 ± 2 4 ,1 2 1 1 -1 5 y ea r 1 8 1 7 ,6 3 7 ,3 5 ± 2 0 ,1 4 6 0 ,6 8 ± 3 2 ,0 3 5 2 ,1 2 ± 2 2 ,1 4 3 3 ,5 5 ± 1 1 ,8 4 3 5 ,5 6 ± 1 8 ,7 6 6 0 ,1 2 ± 2 1 ,1 6 3 0 ,1 4 ± 1 5 ,8 7 4 9 ,2 3 ± 2 6 ,1 2 1 6 -2 0 y ea r 2 5 2 4 ,5 3 2 ,1 4 ± 1 2 ,2 5 6 8 ,2 2 ± 2 2 ,1 2 5 4 ,2 3 ± 1 4 ,3 5 3 3 ,0 8 ± 1 0 ,1 1 3 3 ,2 4 ± 2 0 ,1 5 6 4 ,4 5 ± 2 3 ,5 8 3 1 ,1 5 ± 2 4 ,1 2 5 2 ,1 3 ± 1 4 ,1 2 p N S N S N S 0 ,0 1 N S N S N S N S D is ea se o n se t ag e ≤2 0 y ea r-o ld 1 8 1 7 ,6 6 5 ,2 1 ± 2 4 ,1 2 6 5 ,4 5 ± 2 9 ,2 3 4 8 ,8 8 ± 2 2 ,1 5 2 8 ,2 2 ± 1 0 ,1 9 3 1 ,1 8 ± 2 2 ,1 4 6 0 ,1 2 ± 2 2 ,1 4 3 3 ,4 2 ± 1 1 ,1 5 5 6 ,2 3 ± 2 2 ,1 8 2 1 -3 0 y ea r-o ld 4 4 4 3 ,1 6 3 ,4 7 ± 2 3 ,8 8 6 0 ,1 2 ± 2 3 ,9 8 4 6 ,6 4 ± 1 8 ,4 1 3 6 ,7 2 ± 1 4 ,2 0 3 3 ,6 5 ± 2 1 ,1 8 6 4 ,4 2 ± 2 1 ,4 8 2 9 ,1 2 ± 1 0 ,0 9 5 0 ,1 9 ± 1 9 ,9 5 ≥3 1 y ea r-o ld 3 8 3 7 ,2 6 7 ,3 2 ± 2 0 ,1 9 5 9 ,8 6 ± 2 2 ,1 8 5 1 ,1 2 ± 1 2 ,4 4 3 9 ,1 8 ± 1 5 ,4 9 3 0 ,1 9 ± 2 2 ,2 2 6 2 ,1 2 ± 1 9 ,1 5 3 1 ,1 4 ± 1 4 ,5 4 5 4 ,5 2 ± 2 1 ,1 6 p N S N S N S 0 ,0 5 N S N S N S N S G en it al u lc er at io n (+ ) 3 2 3 1 ,4 5 9 ,8 2 ± 2 6 ,2 4 4 7 ,7 4 ± 1 5 ,8 2 4 9 ,1 2 ± 1 2 ,4 4 4 2 ,1 8 ± 2 4 ,4 5 3 4 ,1 8 ± 2 1 ,1 4 5 9 ,9 7 ± 2 4 ,1 2 3 8 ,7 9 ± 1 8 ,2 0 3 6 ,4 0 ± 1 2 ,9 6 (-) 7 0 7 0 ,6 6 2 ,7 6 ± 2 4 ,1 9 5 1 ,1 8 ± 1 1 ,1 4 5 2 ,1 7 ± 2 1 ,1 7 4 4 ,7 8 ± 1 9 ,4 8 3 9 ,4 5 ± 1 9 ,9 8 6 1 ,1 4 ± 1 9 ,4 9 4 6 ,9 3 ± 2 0 ,5 2 4 3 ,1 1 ± 1 5 ,3 0 p N S N S N S N S N S N S 0 ,0 5 0 ,0 5 U v ei ti s (+ ) 3 0 2 9 ,4 4 9 ,9 7 ± 1 2 ,2 5 3 8 ,8 7 ± 2 4 ,7 2 3 9 ,9 4 ± 2 1 ,1 6 4 3 ,2 8 ± 1 9 ,9 2 3 2 ,1 8 ± 1 9 ,0 8 5 6 ,2 6 ± 1 8 ,1 2 3 2 ,1 4 ± 2 1 ,0 6 3 3 ,9 6 ± 1 2 ,6 4 (-) 7 2 7 0 ,6 5 1 ,1 4 ± 1 0 ,0 9 4 1 ,1 4 ± 2 1 ,1 4 4 1 ,1 8 ± 1 9 ,9 2 4 6 ,7 2 ± 2 0 ,0 2 4 1 ,1 6 ± 2 0 ,1 6 5 9 ,4 7 ± 2 0 ,0 2 4 1 ,1 8 ± 1 9 ,4 8 4 3 ,9 4 ± 1 4 ,8 3 p N S N S N S N S N S N S N S 0 ,0 1 E ry th em a n o d o su m (+ ) 5 0 4 9 ,0 5 8 ,1 2 4 9 ,9 2 ± 2 4 ,1 6 5 0 ,2 6 ± 2 4 ,1 6 4 8 ,4 2 ± 1 2 ,2 4 4 2 ,2 4 ± 1 8 ,8 2 5 9 ,6 6 ± 2 4 .2 3 3 2 ,2 4 ± 1 2 ,2 4 5 2 ,1 4 ± 1 9 ,9 2 (-) 5 2 5 0 ,9 6 1 ,1 6 5 2 ,2 1 ± 1 9 ,9 2 5 3 ,0 4 ± 1 8 ,8 2 5 1 ,1 8 ± 1 4 ,4 2 3 9 ,3 8 ± 1 4 ,9 8 6 9 .9 7 ± 1 2 ,6 5 3 6 ,5 4 ± 1 8 ,5 1 4 9 ,9 8 ± 2 0 ,0 9 p N S N S N S N S N S 0 ,0 5 N S N S T h ro m b o p h le b it is (+ ) 4 4 4 3 ,1 5 7 .4 8 ± 2 1 .1 5 5 1 ,1 4 ± 1 8 ,9 2 4 0 ,2 4 ± 1 7 ,8 2 3 7 ,1 0 ± 1 1 ,1 1 3 7 ,5 6 ± 1 9 ,7 6 6 3 ,4 2 ± 1 9 ,4 8 3 3 ,1 2 ± 1 8 ,4 4 4 8 ,8 3 ± 2 2 ,1 2 (-) 5 8 5 6 ,8 6 7 .1 7 ± 2 2 .1 9 4 8 ,9 8 ± 2 1 ,0 9 4 1 ,3 8 ± 1 7 ,9 8 3 6 ,5 5 ± 1 4 ,8 7 3 4 ,2 4 ± 2 1 ,1 5 6 0 ,1 2 ± 1 7 ,1 5 2 9 ,1 4 ± 1 5 ,2 7 5 2 ,0 3 ± 1 4 ,1 8 p 0 ,0 5 N S N S N S N S N S N S N S P u st u le s (+ ) 5 0 4 9 ,0 4 8 ,9 7 ± 1 3 ,2 5 3 8 ,4 7 ± 2 3 ,7 2 5 0 ,2 2 ± 2 3 ,1 6 4 0 ,1 8 ± 2 0 ,4 5 3 1 ,1 8 ± 1 9 ,8 8 5 5 ,2 6 ± 1 7 ,1 2 3 2 ,4 2 ± 1 2 ,1 5 5 0 ,1 9 ± 2 0 ,9 5 (-) 5 2 5 0 ,9 5 1 ,5 6 ± 1 0 ,9 9 4 1 ,4 4 ± 2 1 ,1 8 5 3 ,2 4 ± 1 8 ,9 2 4 3 ,7 8 ± 1 8 ,4 8 4 1 ,0 2 ± 2 0 ,6 6 5 8 ,4 7 ± 2 1 ,0 2 2 9 ,8 2 ± 1 1 ,0 9 5 3 ,5 2 ± 2 1 ,1 9 p N S N S N S N S N S N S N S N S co n ti n u es i n t h e n ex t p a ge
expected to affect the QoL in patients. It has been shown that general health is more affected than visual
functioning in patients with Behcet uveitis23. Also
sco-res of mental health domain of SF-36 was found to be significantly worse in BD patients with eye
involve-ment in a previous study22. Similar with these results,
we found lower mental health scores in patients with eye involvement anamnesis in our study. Systemic in-volvement may be a major factor associated with im-paired QoL patients with BD as it may lead, not only to severe morbidity but also to increased mortality in the disease. Since there were only a few patients with major vessel involvement and central nervous system involvement in our study, we could not evaluate the QoL in these patients. However, we demonstrated lo-wer scores of general health domain of SF-36 in pa-tients with GIS involvement similar with previous
stu-dies5.
We also investigated the relation between disease activity and QoL in BD. The heterogeneous nature of the disease exspression of BD makes it difficult to achieve a single score for disease activity. Because BDCAF does not have an overall activity score, i.e. a composite index, deduced from the individual scores for different organ systems, we evaluated the possible
correlations for each parameter of the scale24. With this
evaluation disease activity in fatigue subscore was found to be realated with physical function, role phy-sical, bodily pain, and vitality/fatigue subscores of SF-36. In a previous study Gilworth et al demonstra-ted that more than 80 % of the patients with BD think that they do not have enough energy to perform daily
activities8. In another study, fatigue was found to be
one of the most related factors to physical domains of
QoL in patients with BD6. Also paitents with BD
suffe-ring from fatigue was shown to have lower QoL scores related to hindered performance in daily activities, de-creases in physical performance, incompetence in
completing routine tasks4. It can be cocluded that
fa-tigue is one of the most common symptoms related to lower QoL scores in patients with BD. Headache com-ponent of BDCAF showed a correlation with impaired QoL score in bodily pain domain of SF-36 in our stu-dy. Similar with our result, headache was found to be
a factor affecting QoL in previous studies5,6.
In the analysis of possible relations between BD di-sease activity and QoL domains, we demonstrated im-portant correlations. In these aspects, we found corre-lations between disease activity scores of skin lesions, GIS, eye and joint involvements and QoL scores. Al
-tA b le II . c o n tI n u A tI o n S F -3 6 Q o L s u b sc al es M ± S D D is ea se P h y si ca l V it al it y / S o ci al R o le ch ar ac te ri st ic s n % fu n ct io n R o le p h y si ca l B o d il y P ai n G en er al h ea lt h fa ti g u e fu n ct io n em o ti o n al M en ta l h ea lt h Jo in t in v o lv em en t (+ ) 2 8 2 7 ,4 5 8 ,1 6 ± 1 4 .1 3 4 8 ,8 2 ± 2 3 ,1 6 4 3 ,2 2 ± 1 5 ,2 4 4 2 ,2 8 ± 1 8 ,9 2 3 5 ,1 8 ± 2 0 ,1 4 5 6 .4 5 ± 1 5 .1 5 3 8 ,1 4 ± 2 2 ,0 6 5 1 ,1 4 ± 1 9 ,4 2 (-) 7 4 7 2 ,5 7 0 .9 7 ± 2 2 ,6 5 5 2 ,1 1 ± 1 8 ,9 2 4 9 ,1 2 ± 1 2 ,1 5 4 6 ,0 2 ± 2 0 ,1 2 3 8 ,4 5 ± 2 1 ,9 8 6 6 .1 7 ± 1 9 .1 9 4 1 ,7 8 ± 1 9 ,1 8 4 8 ,9 8 ± 2 1 ,0 9 p 0 ,0 5 N S 0 ,0 5 N S N S 0 ,0 5 N S N S G as tr o in te st in al in v o lv em en t (+ ) 1 3 1 2 ,7 4 3 5 ,3 5 ± 2 1 ,1 4 5 9 ,1 2 ± 1 3 ,9 8 4 9 ,2 6 ± 2 2 ,1 6 3 9 ,1 6 ± 1 1 ,1 9 3 7 ,1 8 ± 1 9 ,1 4 5 7 ,2 6 ± 1 2 ,1 2 3 3 ,4 2 ± 1 4 ,1 5 5 1 ,1 9 ± 1 9 ,9 5 (-) 8 9 8 7 ,2 3 2 ,5 4 ± 1 1 ,2 5 5 7 ,8 6 ± 2 1 ,1 8 5 1 ,0 4 ± 1 2 ,8 2 4 5 ,8 6 ± 1 7 ,5 2 3 9 ,1 2 ± 2 0 ,0 8 5 9 ,4 7 ± 2 0 ,0 2 3 0 ,8 8 ± 1 2 ,3 9 5 3 ,0 2 ± 2 0 ,0 2 p N S N S N S 0 ,0 1 N S N S N S N S N S : n o t si g n if ic an t
though other systemic in-volvements couldn’t be evaluated in our study, di-sease activity scores of GIS involvement had a corre-lation with impaired QoL. Disease activity scores of joint involvement was the most related factor to phy-sical domains and pain in our study. This result can support the previous
stu-dies6. Also doctor’s and
patient’s impression of di-sease activity scores sho-wed correlations with vi-tality. It can be concluded that not only the clinical involvement in the disea-se courdisea-se, but also the di-sease activity of the invol-vement affect the QoL in patients with BD. As men-tioned above BD manifes-taitons have been indica-ted as important relaindica-ted factors to QoL in BD. How -ever, data on the BD di-sease activity and its core-lation with QoL are extre-mely limited. Our results indicating correlations between disease activity scores and QoL in BD may contribute the importance of our study. The main weakness of our study was the inability of the evalua-tion of QoL in patients with large vessel and seve-ral systemic involvements due to inadequate number of the cases although it is reasonable to expect im-portant impact of systemic involvement on QoL. How -ever the indication of a correlation between disea-se activity score in GIS in-volvement and QoL might
G IS i n v o lv em en t I: n au se a o r v o m it in g o r ab d o m in al p ai n G IS i n v o lv em en t II : d ia rr h ea w it h a lt er ed o r fr an k b lo o d * p <0 ,0 1 ; * * p <0 ,0 0 1 tA b le II I. th e co r r el A tI o n s b et w ee n b d cA f A n d s f-3 6 s u b sc o r es S F -3 6 Q o L s u b sc al es M ± S D V it al it y / S o ci al R o le P h y si ca l R o le p h y si ca l B o d il y P ai n G en er al h ea lt h F at ig u e fu n ct io n em o ti o n al M en ta l h ea lt h B D C A F fu n ct io n ( r) (r ) (r ) (r ) (r ) (r ) (r ) (r ) F at ig u e -0 ,3 6 0 * -0 ,3 2 8 * -0 ,2 1 9 * 0 ,0 9 -0 ,3 1 2 * 0 ,1 3 0 ,1 6 0 ,2 6 H ea d ac h e -0 ,1 1 0 ,2 1 -0 ,2 8 3 * -0 ,1 2 0 ,2 7 0 ,2 1 0 ,1 5 0 ,2 5 O ra l u lc er at io n -0 ,2 4 6 * -0 ,2 4 3 * 0 ,2 8 0 ,1 3 0 ,1 2 0 ,1 7 -0 ,2 4 0 * -0 ,2 3 8 * G en it al u lc er at io n 0 ,0 9 0 ,1 3 0 ,2 1 0 ,1 6 -0 ,1 7 0 ,0 0 7 -0 ,2 8 8 * -0 ,2 7 7 * E ry th em a n o d o su m /s u p er fi ci al -0 ,2 8 0 ,0 1 0 ,1 8 0 ,0 9 0 ,1 3 0 ,2 9 0 ,2 1 0 ,0 7 th ro m b o p h le b it is P u st u le s 0 ,2 8 0 ,1 6 0 ,2 3 0 ,1 6 0 ,1 0 0 ,1 7 0 ,1 3 0 ,2 1 A rt h ra lg ia -0 ,3 1 4 * -0 ,3 8 2 * * -0 ,3 8 8 * * 0 ,2 3 0 ,1 9 0 ,0 9 -0 ,3 0 4 * -0 ,3 1 2 * A rt h ri ti s -0 ,3 0 2 * -0 ,3 7 2 * * -0 ,3 6 6 * * 0 ,1 3 -0 ,1 2 0 ,0 9 -0 ,2 8 8 * -0 ,3 0 2 * G IS i n v o lv em en t I 0 ,0 9 0 ,2 1 0 ,1 3 -0 ,3 0 2 * 0 ,1 7 0 ,1 9 0 ,1 3 0 ,0 7 G IS i n v o lv em en t II 0 ,2 8 0 ,0 9 0 ,1 2 -0 ,3 5 5 * 0 ,1 7 0 ,1 1 0 ,2 1 0 ,0 9 E y e in v o lv em en t 0 ,2 1 0 ,0 7 -0 ,2 2 -0 ,3 1 1 * 0 ,1 0 0 ,2 1 0 ,1 2 -0 ,3 0 9 * P at ie n t’s i m p re ss io n o f d is ea se 0 ,2 8 0 ,1 3 -0 ,2 1 0 ,1 2 -0 ,3 2 0 * 0 ,0 7 0 ,0 9 0 ,1 7 ac ti v it y l as t 2 8 d ay s P at ie n t’s i m p re ss io n o f d is ea se 0 ,1 7 0 ,1 5 0 ,1 1 0 ,1 5 -0 ,3 0 2 * 0 ,1 6 0 ,0 8 0 ,0 9 ac ti v it y ( to d ay ) D o ct o r’s i m p re ss io n 0 ,1 9 0 ,1 8 0 ,1 1 0 ,0 9 -0 ,2 8 8 * 0 ,1 1 0 ,2 1 0 ,1 7 o f d is ea se a ct iv it y
suggest similar relations with other systemic involve-mets. Further studies evaluating such cases will clari-fy the relationships between QoL and disease activity of systemic involvements in patients with BD.
In conclusion; in addition to demografic features and clinical involvements, BD disease activity can af-fect QoL in patients with BD. These results highlight the importance of managing the symptoms and the di-sease activity effectively in order to improve QoL in BD.
correspondence to
Mehmet Melikoğlu
Erzurum Bölge Eğitim ve Araştırma Hastanesi, Dermatoloji, Erzurum Türkiye
E-mail: [email protected]
references
1. Behçet H. Uber rezidivierende aphthouse durch ein virüs ve-rursachte Geschwuere am Mund, am Auge und an den Geni-talien. Dermatol Monatsschr 1937; 105:1152–1157. 2. Tursen U, Gurler A, Boyvat A. Evaluation of clinical findings
ac-cording to sex in 2313 Turkish patients with Behçet’s disease. Int J Dermatol 2003; 42:346–351.
3. Melikoglu MA, Melikoglu M. The Influence of Age on Behcet’s Disease Activity. The Eurasian Journal of Medicine 2008; 40: 68-71.
4. Canpolat O, Yurtsever S. The Quality of Life in Patients with Behcet’s Disease. Asian Nurs Res 2001;5:229-235.
5. Bernabe E, Marcenes W, Mather J, Phillips, C, Fortune F. Im-pact of Behçet’s syndrome on health-related quality of life: In-fluence of the type and number of symptoms. Rheumatology 2010;49:2165-2171.
6. Bodur H, Borman P, Özdemir Y, Atan Ç, Kural G. Quality of life and life satisfaction in patients with Behçet’s disease: Rela-tionship with disease activity. Clin Rheumatol 2006;25:329--333.
7. Gür A, Saraç AJ, Burkan YK, Nas K, Çevik R. Arthropathy, qua-lity of life, depression, and anxiety Behçet’s disease: relation ship between arthritis and these factors. Clin Rheumatol 2006;25:524-531.
8. Gilworth G, Chamberlain MA, Bhakta B, Haskard D, Silman A, Tennant A. Development of the BD-QoL: A quality of life mea-sure specific to Behçet’s disease. J Rheumatol 2004;31:931-937. 9. International Study Group for Behcet’s Disease. Criteria for the diagnosis of Behcet’s Disease. Lancet 1990; 335:1078–1080.
10. Bhakta BB, Brennan P, James TE, Chamberlain MA et al. Beh-çet’s disease: evaluation of a new instrument to measure clini-cal activity. Rheumatology 1999; 38:728–733.
11. Hamuryudan V, Fresko I, Direskeneli H, Tennant MJ et al. Eva-luation of the Turkish translation of a disease activity form for Behçet’s syndrome. Rheumatology 1999;38:734–736. 12. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item
Short--Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health cons-tructs. Med Care 1993;31: 247–263.
13. Kocyigit H, Aydemir O, Fisek G, Olmez N, Memis A: Validity and reliability of Turkish version of Short form 36: A study of a patients with romatoid disorder. Journal of Drug and Thera-py (in Turkish). 1999; 12:102-106.
14. Uguz, F, Dursun, R, Kaya N, Çilli AS. Emotional symptoms and quality of life in Behçet Disease patients. Journal of Anatolian Psychiatry (in Turkish). 2006; 7:133-139.
15. Tanriverdi N, Ta kintuna, Dürü C, Ozdal P, Ortaç S, Firat E. Health-related quality of life in Behçet patients with ocular in-volvement. Jpn J Ophthalmol 2003;47:85-92.
16. Alpsoy E, Donmez L, Onder M, et al. Clinical features and na-tural course of Behcet’s disease in 661 cases: a multicentre stu-dy. Br J Dermatol 2007; 157: 901-906.
17. Karincaoglu Y, Borlu M, Toker SC, Akman A, Onder M, Gunasti S, et al. Demographic and clinical properties of juvenile-onset Behcet’s disease: A controlled multicenter study. J Am Acad Der-matol 2008; 58: 579-584.
18. Blackford S, Finlay AY, Roberts DL. Quality of life in Behçet’s syndrome: 335 patients surveyed. Br J Dermatol 1997;136:293. 19. Kılınc Y, Yıldırım M, Ceyhan A. (2009). Quality of life in Beh-çet disease patients. Journal of University of Süleyman Demi-rel (ın Turkish). 2009; 16: 6-10.
20. Mumcu G, Hayran O, Ozalp DO, Inanc N, Yavuz S, Ergun T, Direskeneli H. The assessment of oral health-related quality of life by factor analysis in patients with Behcet’s disease and re-current aphthous stomatitis. J Oral Pathol Med 2007;36:147--152.
21. Al-Otaibi LM, Porter SR, Poate TW. Behçet\’s disease: a review. J Dent Res 2005;84:209-22.
22. Ertam I, Kitapcioglu G, Aksu K, Keser G, Ozaksar A, Elbi H, Unal I, Alper S. Quality of life and its relation with disease se-verity in Behçet\’s disease. Clin Exp Rheumatol 2009;27:18-22. 23. Onal S, Savar F, Akman M, Kazokoglu H. Vision- and Health--Related Quality of Life in Patients with Behcet Uveitis. Arch Ophthalmol 2010;128:1265-1271.
24. Melikoglu MA, Melikoglu M. The relationship between disea-se activity and depression in patients with Behcet didisea-seadisea-se and rheumatoid arthritis. Rheumatol Int 2010;30: 941-946.