Mechanical prosthetic valve disease is related with an increase
in depression and anxiety disorder
Yasemin Turker1, Kurtulus Ongel2, Mehmet Ozaydin3, Yasin Turker4, Funda Yildirim Bas5, Mehmet
Akkaya6
1Family Medicine Center, Duzce, 2University of Katip Celebi, Faculty of Medicine, Department of Family Medicine, İzmir, 3University of
Suleyman Demirel, Faculty of Medicine, Department of Cardiology, Isparta, 4Duzce University, Faculty of Medicine, Department of
Car-diology, Duzce, 5University of Suleyman Demirel, Faculty of Medicine, Department of Family Medicine, Isparta, 6Bezm-i Alem University,
Faculty of Medicine, Department of Cardiology, Istanbul; Turkey
Corresponding author: Yasemin Turker
Family Health Center Duzce Provincial Directorate of Health, No. 3, Düzce, Turkey
Phone: +90 505 654 61 70; Fax: +90 380 542 13 87 ;
E-mail: [email protected]
Original submission: 02 July 2014; Revised submission:
18 August 2014; Accepted:
28 August 2014.
ABSTRACT
Aim Patients with organic disease can present with psychiatric symptoms. We hypothesized that since patients with prosthetic heart valve require frequent hospital followup and are at higher risk for complications, the incidence of depression and anxiety is higher in these patients.
Methods This cross-sectional study prospectively studied 98 consecutive patients with mechanical prosthetic heart valve. All
patients fulilled prosthetic heart valve evaluation form, Beck
Depression Inventory (BDI) and Hamilton Anxiety Scale (HAS). Complete blood count, basic metabolic panel and echocardiogram results were collected for all the patients.
Results Using the BDI, there were 26 patients (27%) with no de-pression, 20 (20%) with mild dede-pression, 38 (39%) with mode-rate, 4 (4%) with severe and 10 (10%) patients with very severe depression. Avarege score was 18.3±11.4 on BDI and 19.1±11.1 on HAS. The depression level was positively associated with prot-hrombin time (p<0.001) and international normalized ratio (INR)
level (p<0.001). Hamilton Anxiety Scale was signiicantly corre -lated with comorbidities (r: 0.344; p=0.002), blood transfusion (r: 0.370; p<0.001), obesity (r: 0.319; p=0.007) and Beck Depression Scale was correlated with comorbidities (r: 0.328; p=0.002), in pa-tients with prosthetic heart valve disease.
Conlusion Patients with prosthetic heart valve have higher pre-valence of depression and higher scores of anxiety and depressi-on. Early recognition and appropriate treatment of depression and anxiety may decrease the morbidity in prosthetic heart valve dise-ase. Besides, use of new oral anticoagulant agents that do not need INR check, could decrease anxiety and depression in the future.
Keywords: anxiety, depression, heart valve diseases, comorbiditi-es, prothrombin time, international normalized ratio.
INTRODUCTION
Patients with organic disease can present with psychiatric symptoms. Depression is the most co-mmon psychiatric disorder accompanying organic
disorders and is a signiicant clinical syndrome af -fecting both mortality and morbidity in those pa-tients (1). Among the papa-tients with organic disor-ders, the prevalence of major depression was found to be 5-10% in inpatients and 9-16% in outpatients (2). Patron et al. found that 48% patients were de-pressed any time during their life after cardiac sur-gery (e.g. heart valve sursur-gery, coronary artery by-pass graft) (3). Mechanical prosthetic heart valves are commonly used nowadays for the treatment of heart valve diseases with proven utility for incre-asing life expectancy and quality of life. Patients with prosthetic heart valves constitute 28% of the population with heart valve disease and they need to take anticoagulation therapy lifelong and in-ternational normalized ratio (INR) level check at regular intervals. Besides, these patients may deve-lop structural heart disease over time (4).
We hypothesized that since patients with prosthe-tic heart valve require frequent hospital follow-up and are at higher risk for complications, the incidence of depression and anxiety is higher in these patients.
PATIENTS AND METHODS
Study design
The study was designed as cross-sectional and the patients with mechanical prosthetic heart valve, aged 18 or older, who were admitted to the Cardi-ology Outpatient Clinic, University of Suleyman Demirel, Faculty of Medicine, between March 2008 and August 2009, were consecutively enro-lled. With a tolerance of 5% error, assuming alpha 0.05 and beta 0.20, it was found that 100 patients
would be suficient to detect a signiicant differen -ce. Patients with mental retardation were excluded and all patients gave informed written consents.
All patients completed prosthetic heart valve evaluation form, Beck Depression Inventory (BDI) and Hamilton Anxiety Scale (HAS). In prosthetic heart valve evaluation form the data including patient’s age, gender, type of prosthetic valve, procedure date, need for repeated proce-dure, smoking status, comorbidities (hyperten-sion, obesity, diabetes, chronic renal failure),
history of bleeding, transfusion, cerebrovascular accident, myocardial infarction, congestive he-art failure, pulmonary disease or gastrointestinal disease were collected. Patients’ recent complete blood count, basic metabolic panel and echocar-diogram results were collected too.
Beck Depression Inventory
The Beck Depression Scale (BDS) is one of the most common scales used for assessment of mood disorders and depression, created by Aeron Beck in 1961 (5).It consists of 21 questions, 15
for emotional and 6 for somatic symptoms and i
-lled by the patient. In BDS, scoring ranges from 0-3 on each question. The total score is calculated by summation of all the patient’s responses, so the maximum possible sum is a score of 63. Hi-gher scores on the scale indicate a greater level of depressive symptoms, BDS 0-11 indicates no de-pression, 12-26 mild dede-pression, 17-29 moderate depression, 30-39 severe depression and above 40 indicates very severe depression (5).
Hamilton Anxiety Scale
The Hamilton Anxity Scale measures the severity of anxiety level and symptom distribution. It is a 14-item test including mood and somatic symp-toms administered by an interviewer. Each item
is rated on a ive-point Likert-type scale ranging
from 0-4, so the sum of the score range is be-tween 0-56. The patients must complete the test within 72 hours from the admission (6).
The study protocol was approved by the Ethics Committee of Suleyman Demirel University and all subject signed written consent forms.
Statistical analysis
Measured values are reported as mean ± standard deviation (minimum-maximum values). One-way ANOVA, Kruskal Wallis, chi-square test and student test were used to compare group differen-ces where appropriate. Spearman correlation test was used to identify correlation between continu-ous variables. Differences were considered
signi-icant at a p value of < 0.05.
RESULTS
dura-tion of the surgery for heart valve was 7.89 ± 5.7 years (1-25 year) before they were included into the study (Table 1). According to the BDS, there were 26 (27%) patients with no depression, 20 (20%) with mild depression, 38 (39%) with mo-derate, four (4%) with severe and 10 (10%) pati-ents with very severe depression. Avarege score was 18.3 ± 11.4 on BDS and 19.1 ± 11.1 on HAS.
in eight (8%) and obesity in nine (9%) patients. Arrhythmia was detected in 26 patients, 19 had
atrial ibrillation, one had atrial lutter, ive had
premature atrial contraction and one had prema-ture ventricular contraction.
Table 2 showed the comparison between depre-ssion level on BDS and patients complete blo-od count (CBC), coagulation parameters, fasting glucose, renal function test and
echocardiograp-hic indings. The depression level was positively
correlated with prothrombin time and INR le-vel. Prothrombin time was longer than expected in patients with mild and moderate depression (36±12.4 vs. 39±11.7, respectively), whereas it was shorter than expected in patients with very severe depression (21.8±8.2) (Table 2). Patients with severe depression were also found to have lower than expected INR levels (Table 2).
Howe-ver, BDS was not signiicantly correlated with
prothrombin time (p=0.446) and INR (p=0.919) (in correlation analysis).
Characteristic No (%) of patients/value at current visit
Number 98
Age, years 53.6±10.9
Gender (male) 54 (54.5)
AVR 10 (10%)
MVR 75 (77)
AVR and MVR 13 (13)
Beck Depression Inventrory 18.3±11.4
No depression 26 (27)
Mild depression 20 (20)
Moderate depression 38 (39)
Severe depression 4 (4)
Very severe depression 10 (10)
Hamilton Anxiety Scale 19.1±11.1
Cerebrovascular accident 3 (3)
CHF 2 (2)
COAH 2 (2)
Gastrointestinal bleeding 4 (4)
Epistaxis 19 (19.4)
Gingival bleeding 15 (15.3)
Blood transfusion 8 (8)
Hypertension 29 (30)
Diabetes mellitus 8 (8%)
Obesity 9 (9)
Arrhythmia 26 (26.5)
Atrial ibrillation 19 (19.4)
Atrial lutter 1 (1)
Premature atrial contraction 5 (5)
Premature ventricular contraction 1 (1)
Table 1. Characteristics of study participants
AVR, aort valve replacement; MVR, mitral valve replacement; COAH, chronic obtructive pulmanary disease; CHF, congestive heart failure
Depression level
Paremeters(n = 26)No (n = 20)Mild Moderate(n = 38) Severe(n = 4) severeVery (n = 10) p
Hb (g/dL) 12.6 ± 1.6 13.1 ± 1.6 12.5 ± 1.0 13.3 ± 1.3 13 ± 1.2 0.462 Glucose (mg/dL) 108 ± 71 90 ± 11 93 ± 9.3 96 ± 1.7 108 ± 19.7 0.474 PT (sec) 27.5 ± 8.6 36 ± 12.4 39 ± 11.7 28.5 ± 4.04 21.8 ± 8.2 < 0.001
INR 2.64 ±
0.7 3.19 ± 1.06 3.3 ± 0.99 2.09 ± 0.1 2.5 ± 0.41 < 0.001 BUN (mg/dL) 21.5 ± 6.1 17.2 ± 3.3 21.1 ± 6.4 17 ± 6.9 18.6 ± 4.6 0.535 Cr (mg/dL) 0.9 ± 0.1 0.8 ± 0.2 0.9 ± 0.2 1 ± 0.08 0.7 ± 0.3 0.212
EF (%) 60.3 ±
7.9 54.5 ± 11.5 58.4 ± 7.9 62.5 ± 2.8 58 ± 7.1 0.187 LA (mm) 44.9 ± 5.9 44.5 ± 3.5 46.3 ± 6.2 47 ± 2.3 41.2 ± 4.9 0.110
Table 2. Comparison between depression level and laboratory and echocardiographic data
EF, ejection fraction; Hb, hemoglobin; INR, international normalized ratio; LA, left atrium diameter; PT, prothrombin time; Cr, creatinine
Of those 98 patients, eight (8%) were 33-40, 31 (31%) 41-50, 36 (37%) 51-60, 13 (13%) 61-70 and 10 (10%) were 71-80 years of age. A compa-rison of patients by age groups did not show diffe-rence for either BDS (p=0.520) or HAS (p=0.469).
Medical history of the patients was signiicant for
cerebrovascular accident in three (3%) patients, congestive heart failure and chronic obstructive pulmonary disease in two (2%) patients each. Four patients had gastrointestinal bleeding, 19 had epistaxis and 15 patients had gingival blee-ding after the surgery. Eight patients had recei-ved blood transfusion due to anemia or bleeding. Among the cardiac risk factors, hypertension was present in 29 (30%) patients, diabetes mellitus
The depression levels were also compared with patients’ demographic and clinical features (Ta-ble 3). Patients with comorbidities accompa-nying prosthetic heart valve had more advanced degree of depression (p=0.005). Similary, chro-nic gastrointestinal disease was correlated with very severe stage of depression (p=0.001). Other
parameters did not show signiicant difference.
p = 0.001) and more anxious according to HAS (23.2 ± 11.7 vs. 15.0 ± 9.4; p = 0.001) than pa-tients without comorbidities. The presence of hypertension was associated with higher scores for both depression (24.9 ± 10.2 vs. 16.7 ± 10.6; p = 0.01) and anxiety (24.9 ± 10.2 vs. 16.7 ±
10.6; p = 0.01). There was no signiicant diffe
-rence between patients with and without diabetes for depression (p=0.272) and anxiety (p = 0.842). Gender difference, history of repeat procedure, cerebrovascular accident, congestive heart failu-re and smoking status wefailu-re also not in corfailu-relation to depression and anxiety.
History of bleeding by itself was not associated with depression and anxiety. However, while de-pression score was not different between patients with and without blood transfusion (p=0.235)
due to anemia or bleeding, patients with transfu-sion history were more anxious (32 ± 4.2 vs. 17.9 ± 10.8; p < 0.001). Similarly patients with obesi-ty were more anxious than non-obese ones (27.77 ± 7.83 vs. 18.24 ± 11.09; p=0.014).
Patients with arrhyhthmia had similar depression scores compared to the patients without arrhyt-hmia. Although the difference did not reach
statistical signiicance, patients with arrhythmia
tended to be more anxious than those without it (22.7 ± 12.7 vs. 17.8 ± 10.2; p=0.054). The pre-sence of gastrointestinal disease in the patients was correlated with both high depression (45 ± 10.0 vs. 17.8 ± 10.8; p=0.001) and anxiety (39 ± 10.0 vs. 18.7 ± 10.8; p=0.01) scores.
The Hamilton Anxiety Scale was signiicantly
correlated with comorbidities (r: 0.344; p=0.002), blood transfusion (r: 0.370; p<0.001), obesity (r: 0.319; p=0.007) and the Beck Depression Scale (r: 0.660; p<0.001) in patients with prosthetic heart valve disease. The Beck Depression Scale was correlated with comorbidities (r: 0.328; p = 0.002) in patients with prosthetic heart valve disease.
The Hamilton Anxiety Scale was not signiicantly
correlated with PT (p=0.423) and INR (p =0.789).
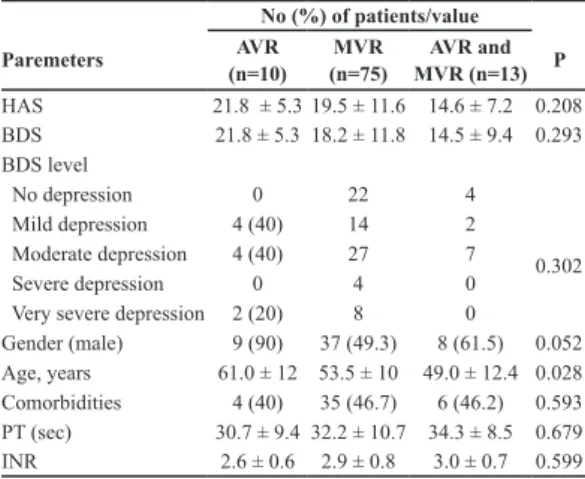
The type of heart valve surgery were aortic valve replacement (AVR) for 10 (10%) patients, mitral valve replacement (MVR) for 75 (77%) patients and both AVR and MVR for 13 (13%) patients. Table 4 showed the comparison between type of heart valve surgery and clinic and laboratory
data. There were no signiicant differences in
HAS, depression level and BDS between ARV, MVR and AVR and MVR.
DISCUSSION
In the present study, the level of depression and anxiety in patients with prosthetic heart valve and its relationship with the demographic and
clinical features was investigated. A signiicant
association between depression level and prot-hrombin and INR levels was found. The level of depression was more severe in patients having comorbidities and gastrointestinal disease. Besi-des, hypertensive patients were more anxious and depressive compared to non-hypertensive ones. Patients who had blood transfusion and obesity were more anxious.
Chronic diseases are long-term diseases that may cause psychiatric problems in their course (7-9).
No (%) of patients with depression level
Paremeters (n = 26)No (n = 20)Mild Moderate(n = 38) Severe(n = 4) severeVery (n = 10) p
Gender (male) 15 (58) 13 (65) 18 (47) 3 (75) 4 (40) 0.523
Smoker 1 (4) 3 (15) 0 0 2 (20) 0.058
Comorbidities 8 (30.7) 8 (40) 17 (44.7) 2 (50) 10 (100) 0.005
Heart Failure 2 (7.6) 1 (5) 3 (37.5) 0 0 0.873
Arrhythmia 6 (23.07) 7 (35) 7 (18.4) 2 (50) 4 (40) 0.385
DM 2 (7.6) 1 (5) 3 (7.8) 0 2 (20) 0.657
Obesity 2 (7.6) 0 5 (13.1) 0 2 (20) 0.338
HT 4 (15.3) 5 (25) 12 (31.5) 2 (50) 6 (60) 0.090
CVA 0 0 3 (7.8) 0 0 0.308
Bleeding 7 (29.9) 10 (50) 19 (50) 0 2 (20) 0.070
GIS disease 0 0 0 0 2 (20) 0.001
Repeat surgery 2 (7.6) 4 (20) 4 (10.5) 0 0 0.436
Table 3. Comparison between depression level and demo
-graphic and clinical features
GIS, gastro intestinal system; DM, diabetes mellitus; HT, hypertansi-on; CVA, cerebrovascular disease
No (%) of patients/value Paremeters (n=10)AVR (n=75)MVR MVR (n=13)AVR and P
HAS 21.8 ± 5.3 19.5 ± 11.6 14.6 ± 7.2 0.208
BDS 21.8 ± 5.3 18.2 ± 11.8 14.5 ± 9.4 0.293
BDS level
0.302
No depression 0 22 4
Mild depression 4 (40) 14 2
Moderate depression 4 (40) 27 7
Severe depression 0 4 0
Very severe depression 2 (20) 8 0
Gender (male) 9 (90) 37 (49.3) 8 (61.5) 0.052
Age, years 61.0 ± 12 53.5 ± 10 49.0 ± 12.4 0.028
Comorbidities 4 (40) 35 (46.7) 6 (46.2) 0.593
PT (sec) 30.7 ± 9.4 32.2 ± 10.7 34.3 ± 8.5 0.679
INR 2.6 ± 0.6 2.9 ± 0.8 3.0 ± 0.7 0.599
Table 4. Comparison between type of heart valve surgery and clinical and laboratory data
Depression and anxiety disorder are the most com-mon psychiatric diseases occurring in patients with somatic diseases and they usually coexist (10). Worsening in the quality of life, functional disabi-lity and direct biological effects of organic diseases are the main reasons for development of depression (11). Several studies have reported increased pre-valence of depression and anxiety in patients with chronic disease as compared to patients without chronic disease (12-16). It was determined that pa-tients undergoing heart operation experienced such physical and psychological problems as decrease in appetite, sleep disturbances, fatigue and activi-ty intolerance, anxieactivi-ty and depression within six months of being discharged (17). In our study, 27% of the patients with prosthetic heart valve did not have depression measured by the Beck Depression Inventory. In a study done by Bahar et al., age was reported to be correlated with higher anxiety and depression scores (15). On the contrary, Munir et al. found that majority of patients with anxiety and depression were aged between 20-49 years (18). In
the present study, we did not ind signiicant diffe -rence in neither the Beck Depression Inventory nor Hamilton Anxiety Scale by patient’s age.
Female gender has been shown to be a risk factor for the development of depression. Some studies have demonstrated that women have higher ave-rage depression scores than males (19-20). Gil-mour et al. found that females with depression had a higher risk for the development of heart disease while males did not (21).
The relationship between psychiatric disorders and irritable bowel syndrome has been subject of inte-rest for a long time (22). It has been shown that pa-tients with irritable bowel syndrome have a higher incidence of depression and anxiety disorder (23). In addition, patients with depression have also been reported to have higher incidence of gasto-rinteestinal disease (24). Coexistance of depression and irritable bowel syndrome has been attributed to increased sympathetic activity. Our results are in accordance with previous studies, showing that patients with gastrointestinal diseases were more depressive and anxious. These patients were also more likely to be in “very severe depression group” in the Beck Depression Inventory groups.
This study demonstrated a signiicant relationship
between the depression levels and the prothrom-bin time and INR levels. Longer prothromprothrom-bin time
than expected in patients with mild and moderate depression was found, whereas it was shorter than expected in patients with severe depression. Addi-tionally, INR levels were lower than expected in
the very severe depression group. These indings
may indicate that patients with more depression and anxiety have lower sense of responsibility to protect themselves from possible complications that may occur due to prosthetic heart valve dise-ase. It is reasonable to think that these patients do not have regular prothrombin time and INR check and hence cannot reach target values.
In the present study, the prevalence of depression and anxiety was higher in patients with comorbidi-ties accompanying prosthetic heart valve disease. Besides, the level of depression was more severe in these patients compared to patients without comor-bidities. Patients with chronic diseases are known to be more depressive and anxious (13,15,16). Sin-ce the study participants had chronic heart disease, comorbidities with this challenging heart problem make them more depressive and anxious.
A meta-analysis reported a signiicantly higher risk
for the development of hypertension in patients with high psychological stress levels. Moreover, it was claimed that this risk is comparable to well-known risk facors for the development of hyper-tension such as obesity and lack of physical acti-vity (25). Supporting the literature, patients with hypertension in this study were more depressive than without hypertension using the Beck Deprer-ssion Inventory. The Hamilton Scale anxiety scores were also higher in patients with hypertension.
Patients requiring blood transfusion following bleeding or due to anemia experienced intense anxiety in this study. Since patients with prosthe-tic heart valve need frequent follow-ups over a long period of time, the need for admission to the hospital for blood transfusion probably makes them more aggressive and anxious.
non-REFERENCES
1. Katon W, Ciechanowski P. Impact of major depressi-on depressi-on chrdepressi-onic medical illness. J Psychosom Res 2002; 53:859-63.
2. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry1992; 14:237-47.
3. Patron E, Messerotti Benvenuti S, Zanatta P, Pole-sel E, Palomba D. Preexisting depressive symptoms are associated with long-term cognitive decline in patients after cardiac surgery. Gen Hosp Psychiatry 2013; 35:472-9.
4. Otto CM, Prosthetic valves. In: Otto CM (Ed.). Val-vular Heart Disease. Philadelphia: WB Saunders, 1999: 380- 416.
5. Burns DD. Feeling Good. The New Mood Therapy. New York: Morrow, 1980.
6. Yazıcı MK, Demir B, Tanrıverdi N, Karaağaoğlu E, Yolaç P. Hamilton Anxiety Rating Scale: Interrater
Reliabilty and Validity Study. Turk Psikiyatri Derg 1998; 9:114-7.
7. Strain JJ, Lyons JS, Hammer JS, Fahs M, Lebovits A, Paddison PL, Snyder S, Strauss E, Burton R, Nuber G, et al. Cost Offset from a Psychiatric Consultation-liaion Intervention with Elderly Hip Fracture Patients. Am J Psychiatry 1991; 148:1044-9.
obese patients whereas obese patients were found to feel more anxious.
Prevalence of anxiety and depression is very co-mmon in patients with ischemic heart disease (28). Persistent symptoms of anxiety and depre-ssion increased substantially the risk of death in patients with ischemic heart disease (29). Patients with organic disease with major depressive disor-der have longer in-hospital stays, fail to comply with treatment of the disease and medication they are prescribed, and have increased mortality and morbidy rates. Similar correlation is also found in patients with anxiety. Van Hout et al. reported that presence of anxiety disorder increases mortality in men, however, mortality in women is not
increa-sed (30). Garield et al. reported that anxiety disor -ders, major depressive disorder, and co-occurring anxiety and major depressive disorder are associa-ted with incident heart failure in large cohort (31).
The depression and anxiety scores were not
si-gniicantly different among the prosthetic valve
type in this study. Relatively lower depression and anxiety detection in patients with both AVR and MVR may be associated with their younger age.
Ther are several limitations of the present study. The number of patients across the different
de-pression categories is unbalanced (only four pa-tients in severe depression), therefore, a more balanced sample size across the depression cate-gories would potentially allow for more robust comparison between these groups. The other li-mitation of study was that there was no control group of healthy individuals. Finally, patients did not have pre-surgery measurements of depressi-on and anxiety level to compare the difference between pre and post surgery changes.
In conclusion, it is crucial to identify depression and anxiety disorders of the patients with mecha-nical prosthetic valve disease, which can play an important role in treatment planning, and helps physicians predict the indication for treatment mo-dalities and good long-term outcomes. Early re-cognition and appropriate treatment of depression and anxiety may decrease the morbidity in prosthe-tic heart valve disease. Besides, use of new oral an-ticoagulant agents that do not need INR check, co-uld decrease anxiety and depression in the future.
FUNDING
No speciic funding was received for this study.
TRANSPARENCY DECLARATIONS
Competing interest; none to declare.
8. Sim K, Rajasoorya C, Lam KN, Chew LS, Chan YH. High prevalence of psychiatric morbidity in a medical intensive care unit. Singapore Medical Journal 2001; 42:522-5.
9. Gagnon LM, Patten SB. Major depression and its association with long-term medical conditions. Cana-dian Journal of Psychiatry 2002; 47:149-52. 10. Hirschfeld RM. The Comorbidity of Major
Depressi-on and Anxiety Disorders: RecognitiDepressi-on and Manage-ment in Primary Care. Prim Care Companion J Clin Psychiatry 2001; 3: 244-54.
11. Kılıcoglu A. Risk factors and etiology of depression
among elderly: a review. Anatolian Journal of Psychi-atry 2006; 7:49-54.
12. Ozmen E, Taşkin EO, Ozmen D, Demet MM. Which
psychiatric label is more stigmatizating? “ruhsal ha-stalik” or “akil hastaligi”. Turk Psikiyatri Derg 2004; 15:47-55.
13. Altan L, Bingöl U, Sagirkaya Z, Sarandöl A, Yurtku
-ran M. Anxiety and depression in rheumatoid arthritis patients. Turk J Rheumatol 2004; 19:7-13.
14. Hacıhasanoglu R, Yıldırım A. Depression among the
elderly in Erzincan nursing home and inluential fac
15. Bahar A, Tutkun H, Sertbas G. The determination of the level of anxiety and depression of old people who live in the nursing home. Anadolu Psikiyatri Derg 2005; 6:227-39.
16. Romao AP, Gorayeb R, Romao GS, Poli-Neto OB, dos Reis FJ, Rosa-e-Silva JC, Nogueira AA. High Levels of Anxiety and Depression have a Negative Effect on Quality of Life Women with Chronic Pelvic Pain. Int J Clin Pract 2009; 63:707-11.
17. Jaarsma T, Kastermans M, Dassen T, Philipsen H. Problems of cardiac patients in early recovery. J Adv Nurs 1995; 21:21-7.
18. Munir F, Khan HTA, Yarker J, Haslam C, Long H, Bains M, Kalawsky K. Self-Management of Health – Behaviors Among Older and Younger Workers with Chronic Illness. Patient Educ Couns 2009; 77:109-15. 19. Güz H, Yaman MA, Dilbaz N. Frequency of depre-ssion and psychiatric symptoms in elderly populati-on with physical illness. Türkiye’de Psikiyatri 2007; 9:44-9.
20. Yakar T, Baran A, Güngör S, Altinsoy B, Yalcinsoy
M, Can G, Akkaya E. The factors affecting Beck de-pression scale in asthmatic patients. Tuberk Toraks 2007; 55:11-7.
21. Gilmour H. Depression and risk of heart disease. He-alth Rep 2008; 19:7-17.
22. Creed F, Guthrie E. Psychological factors in the irrita-ble bowel syndrome. Gut 1987; 28:1307-18. 23. Lydiard RB. Irritable bowel syndrome, anxiety, and
depression: what are the links? J Clin Psychiatry 2001; 62(Suppl 8):38-45.
24. Garakani A, Win T, Virk S, Gupta S, Kaplan D, Ma-sand PS. Comorbidity of irritable bowel syndrome in psychiatric patients: a review. Am J Ther 2003; 10:61-7.
25. Ruthledge T, Hogan BE. A quantitative review of prospective evidence linking psychological factors with hypertension development. Psychosom Med 2002; 64:758-66.
26. Black DW, Goldstein RB, Mason EE. Prevalence of mental disorder in 88 morbidly obese bariatric clinic patients. Am J Psychiatry 1992; 149:227-34. 27. Britz B, Siegfried W, Ziegler A, Lamertz C,
Her-pertz-Dahlmann BM, Remschmidt H, Wittchen HU, Hebebrand J. Rates of psychiatric disorders in a cli-nical study group of adolescents with extreme obesity and in obese adolescents ascertained via a populati-on based study. Int J Obes Relat Metab Disord 2000; 24:1707-14.
28. Pająk A, Jankowski P, Kotseva K, Heidrich J, de
Smedt D, De Bacquer D; EUROASPIRE Study Gro-up. Depression, anxiety, and risk factor control in patients after hospitalization for coronary heart dise-ase: the EUROASPIRE III Study. Eur J Prev Cardiol 2013; 20:331-40.
29. Doering LV, Moser DK, Riegel B, McKinley S, Da-vidson P, Baker H, Meischke H, Dracup K. Persistent comorbid symptoms of depression and anxiety pre-dict mortality in heart disease. Int J Cardiol 2010; 145:188-92.
30. van Hout HP, Beekman AT, de Beurs E, Comijs H, van Marwijk H, de Haan M, van Tilburg W, Deeg DJ. Anxiety and the risk of death in older men and wo-men. Br J Psychiatry 2004; 185:399-404.
31. Garield LD, Scherrer JF, Hauptman PJ, Freedland