ABSTRACT
Purpose: To evaluate subjects submitted to supracricoid laryngectomy concerning vocal self-assessment, auditory-perceptual and acoustic analysis, and the impact of dysphonia on the quality of life. Methods: Twelve male subjects, who underwent supracricoid laryngectomy for carcinoma resection, mean age of 59.3 years, took part in this prospec-tive observational study. The auditory-perceptual analysis was performed through GRBASI scale in double blind. The acoustic analysis used the VOXMETRIA® software to obtain the fundamental frequency (f0), jitter, shimmer, glottal to noise excitation ratio and phonatory deviation diagram. The self-assessment and the impact of organic dysphonia on the quality of life of these subjects was observed through Voice-Related Quality of Life V-RQOL and Voice Handicap Index (VHI) protocols. Results: f0 ranged between 91.59 Hz and 260.05 Hz, shimmer and/or jitter measures were fairly altered confirming the results of the auditory-perceptual analysis that revealed a vocal deviation degree from moder-ate to intense, despite the subjects having considered their voices as good or reasonable. However the V-RQOL results showed 50.0% of the subjects presenting gross scores consistent with dysphonic voices. The Voice Handicap Index showed highest scores for the organic domain. Conclusion: The vocal deviation degree of subjects varied from moder-ate to intense, corroborating the acoustic analysis; nevertheless, subjects classified their voices as reasonable and good. Scores of V-RQOL and VHI revealed predominance of the physic and organic domains respec-tively, compatible with dysphonic voices. Further studies are necessary for a better understanding of the relation between vocal self-assessment and impact on quality of life of subjects with dysphonia resulting from laryngeal carcinoma.
Keywords: Dysphonia; Quality of life; Voice; Laryngectomy; Laryngeal Neoplasms
RESUMO
Objetivo: Avaliar sujeitos submetidos a laringectomia supracricóide quanto à autoavaliação da voz, análises perceptivo-auditiva e acústica e impacto da alteração vocal na qualidade de vida. Métodos: Estudo pros-pectivo,observacional, queenvolveu 12 sujeitos do gênero masculino, com disfonia orgânica, média de idade de 59,3 anos, que realizaram la-ringectomia supracricóide para exérese de neoplasia maligna de laringe. Foi realizada análise perceptivo-auditiva, por meio da escala GRBASI em duplo-cego. A análise acústica realizada através do software
VOX-METRIA®considerou parâmetros de frequência fundamental, jitter e shimmer, proporção harmônico–ruído e diagrama de desvio fonatório.
A autoavaliação vocal e o estudo do impacto da disfonia na qualidade de vida dos sujeitos ocorreram por meio de aplicação dos protocolos: Qualidade de Vida em Voz (QVV) e o Índice de Desvantagem Vocal (IDV). Resultados: Afrequência das vozes variou entre 91,59 Hz e 260,05 Hz e as medidas de shimmer e jitter mostraram-sealteradas,
comprovando as análises perceptivo-auditivas, que revelaram vozes com grau de desvio de moderado a intenso. A maioria dos sujeitos qualificou suas vozes como razoável ou boa. O QVV demonstrou escores brutos em níveis compatíveis com vozes disfônicas em 50,0%. O IDV mostrou predomínio do domínio orgânico. Conclusão: O grau de desvio vocal dos sujeitos mostrou-se entre moderado e intenso, confirmando parâme-tros acústicos, enquanto que os sujeitos qualificaram suas vozes como razoáveis ou boas. Os escores do QVV e IDV revelaram predomínio de domínios físico e orgânico, respectivamente, com parte dos sujeitos com escores compatíveis a vozes disfônicas. Sugerem-se estudos que busquem aprofundar o conhecimento entre autopercepção da voz e impacto na qualidade de vida de sujeitos com disfonia decorrente de carcinoma de laringe.
Descritores: Disfonia; Qualidade de Vida; Voz; Laringectomia; Neo-plasias Laríngeas
This study was at Speech Pathology Faculty, Pontifícia Universidade Católica de Campinas – PUC – Campinas (SP), Brazil, with FAPIC Reitoria scholarship scientific initiation.
(1) Faculty of Speech Pathology, Pontifícia Universidade Católica de Campinas – PUC – Campinas (SP), Brazil. (2) Academic of Medical Sciences Faculty, Pontifícia Universidade Católica de Campinas – PUC – Campinas (SP), Brazil. Conflict of interests: No
Author’s contribution: IBO main researcher, research advisor, data collection and analysis, article writing, article writing correction, article submission and procedures, ACVA literature research, initial version writing collaboration, data collection and analysis; DMS literature research, initial version writing collabora-tion, data collection and analysis
Correspondence address: Iára Bittante de Oliveira. Av. John Boyd Dunlop, s/n, Jardim Ipaussuruma, Campinas, São Paulo, Brazil, CEP: 13060-904. E-mail: [email protected]
Received: 2/20/2012; Accepted: 10/14/2013
Voice assessment and quality of life after supracricoid
laryngectomy
Avaliação de voz e qualidade de vida após laringectomia
supracricóide
INTRODUCTION
Larynx cancer is considered the most common head and neck malignant neoplasm, mainly occurring in male indi-viduals, with an incidence of 130.000 new cases a year in the world(1). It’s main symptom is dysphonia, once the glottis
region is generally more affected, followed by the supraglottis and subglottis regions(2). The most common histological type in
larynx is the spinocellular carcinoma, with a ratio of seven men to one woman(1) and a higher incidence from 50 years of age(3).
The stage and localization of the larynx tumor is what defi-nes the treatment(4). The neoplasm resection through
supracri-coid laryngectomy was initially described by Majer and Rieder, in 1959 and later by Labayle and Bismuth, around 1972, being considered a subtotal laryngectomy(5,6). It was idealized in order
to avoid total laryngectomy in patients with tumor, in which traditional partial procedures would be contraindicated, inclu-ding those advanced and recurrent from primary treatment(6).
Nevertheless, when a patient is submitted to this treatment, he may develop vocal disorders, once there is an alteration in the histological and geometrical architecture of the glottis(7)
that could damage oral communication and social interaction(4).
Cancer rehabilitation is a dynamic continuous process ai-ming at maximizing individual capacities within the disease’s limitations and handicaps(8). Thus, speech evaluation of a
pa-tient with vocal change due to partial laryngectomy should be included not only as routine, such as auditory-perceptual and acoustic analysis, but also as a well-being estimates, that may be measured by protocols that assess quality of life regarding voice(9).
Comparative studies of quality of life of patients submitted to partial and those submitted to total laryngectomy point that the last ones tend to have worse scores regarding quality of life, when compared to the first ones(4), besides low self-stem,
diminished interest in searching for happiness and absence of social well-being(5).
The concept of quality of life is broad, subjective and personal, and its assessment is a difficult attribution, once it varies according to each patient’s priorities(9). The measurement
of physical, psychological and social impacts is essential to establish rehabilitation and support parameters for patients(8).
The investigation of the patient self-perception regarding the disadvantages of vocal disorders has been valued(10). Protocols
for the assessment of impacts of dysphonia upon quality of life were adapted and validated for Brazilian Portuguese, such as the voice-related quality of life (V-RQOL) and the voice handicap index (VHI)(9,11).
After surgery, the larynx does not have specialized struc-tures that allow a constant and stable vibration, and the sound produced is usually followed by roughness and breathiness. The voice modification resulting from surgery was not consi-dered in a recent past, providing that there was an oncological success. Currently, it is known that it is an important parameter
to be analyzed, aiming the therapeutic process and the quality of life(12).
The auditory-perceptual and the acoustic analysis are the most frequently used tools for the assessment of voice. In the perceptual analysis, voices are judged by scales, usually GRBASI, which is used and known worldwide(13,14). Such scale,
initially presented as GRBAS, is a auditory-perceptual scale created by the Committee for Phonatory Function Tests of the Japan Society of Logopedics and Phoniatrics, and published by Hirano (1981)(15,16). Through the scale mentioned above it is
possible to determine: G = grade of dysphonia; R = roughness; B = breathiness; A = asthenia; and S = strain. The parameter “I”, for instability, was added later and relates quality of voice to its fluctuation degree, then forming GRBASI(15).
Roughness is present when there is periodicity of vibration, and the adduction of vocal cords is incomplete in the closure phase of the vibrating cycle. It is generally associated to organic lesions of larynx, changing the vibration pattern of the vocal cords mucosa, such as in cases of nodules, polyps, edemas and even neoplasms(17,18). The breathiness refers to the presence of
air scape heard during phonation; it causes the impression of a weak voice with reduced intensity(15,16), with a compatible
degree with the glottal closure conditions. Asthenic voice is related to weak intensity associated, or not, to neurological disorders symptoms(17). Strained voice is an unpleasant voice
characterized by restrict vibration of vocal cords mucosa and exaggerated contraction of laryngeal vestibules at the median and antero-posterior level(18).
The acoustic analysis provides measures related to the vibration pattern of vocal cords, the vocal tract shape and its changes in time. Results interpretation varies according to age, gender, phonation type, and vocal training(19). The following
pa-rameters are observed: fundamental frequency (f0), short-term frequency disturbance (jitter), long-term amplitude disturbance (shimmer), and glottal to noise excitation ratio.
It is important to know the vocal profile, as well as the impacts of voice upon quality of life of patients with vocal limitations resulting from larynx subtotal surgery, such as supracricoid.
This study aimed to assess subjects who underwent su-pracricoid laryngectomy, regarding vocal self-assessment, auditory-perceptual and acoustic analysis, correlating the impact of vocal disorder on their quality of life.
METHODS
dysphagia in order to improve vocal condition and, thus, were included in the study.
For the auditory-perceptual analysis, voice samples were collected in a digital system, with a headset microphone Plantronics positioned 10 centimeters from the subject’s mouth, and were directly stored in a notebook SonyVaio®, Windows XP. Voice samples were constituted by automatic speech emis-sion of numbers from 1 to 20 and of moths of the year. Voices were judged through the GRBASI scale, by a voice specialist speech pathologist who treats both, organic and functional dysphonia. Double blind method was used for such procedure and voices were randomized and copied in digital system in order to be presented to the speech pathologist judge. The voice judgment was graded in 0 for adapted voice; 1 for mild disorder; 2 for moderate; and 3 intense vocal disorder, with intra-evaluator reliability control.
The software Voxmetria® was used for the acoustic analy-sis, following the same procedure described above. Measures were extracted from voice sample of vowel-sustained /a/. All samples were organized in three seconds, disregarding the beginning and the end of the emission. Measures of frequency; shimmer; jitter; glottal to noise excitation ratio; and the pho-natory deviation diagram were considered.
For the assessment of quality of life regarding the voice, two protocols were used, the Voice-related quality of life (V-RQOL) and the Voice handicap index (VHI), aiming to improve knowledge of the impact of dysphonia upon the quality of life of the group.
The Voice-related quality of life questionnaire (V-RQOL) comprises ten questions, divided into physical (six questions) and social-emotional subscales (four questions), allowing the dysphonic person to self-assess his/her voice(16). Each item is
scored on a 5-point interval scale that reflects the severity of the problem. The highest possible score is 100 reflecting the highest quality of life. The Voice handicap index (VHI) comprises 30 questions concerning three domains: functional, organic and emotional. It searches to describe the effect that altered voices may have upon quality of life of people with dysphonia(12,19).
Questionnaire was applied individually and always with the presence of a researcher with previous training.
Results from VHI were analyzed based on score 100, the-refore there was a conversion of the score 120(11). Response
patterns were classified into positive or negative in all 30 questions. Questions with responses “never=0” or “almost never=1” were considered negative, and the ones with respon-ses “sometimes=2”, “almost always=3” or “always=4” were considered positive.
Statistical analysis used Chi-square test, Spearman Correlation and Cochran test, with a significance level of 5%.
Competences and limitations of each individual were respected, and ethic aspects were preserved. All participants signed the Informed Consent Term and the Ethics Committee of Pontifical Catholic University of Campinas (PUC) approved the study, protocol number 830/09.
RESULTS
The study group was composed by male subjects with or-ganic dysphonia after supracricoid laryngectomy, undergoing speech therapy to improve voice, after the compensation of dysphagia. The mean age was 59.3 years.
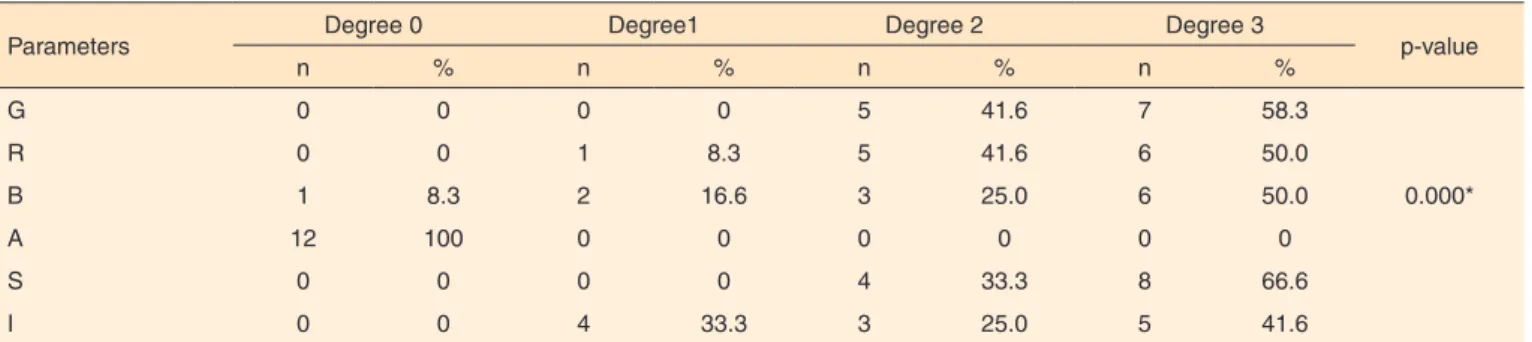
All subjects presented vocal deviation degree from mode-rate to intense, degrees 2, 3 and 4 respectively. Five (41.6%) of them were classified as moderate, and seven (58.3%) as intense. Regarding roughness of voice, only one subject presented degree 1, or mild. Breathiness was observed with predominance of mo-derate and intense degrees (75.0%). Strained voice was found from moderate to intense in 100% of subjects. The Chi-square test revealed p=0.000, showing statistical evidences between the GRBASI parameters and the vocal deviation degrees. Table 1 presents the results of perceptual analysis of patients’ voices.
Jitter is considered altered when values are above 0.6. Eleven patients (91.3%) presented altered jitter. Shimmer is considered altered when values are above 6.5. No subjects were within normality range. Regarding the glottal to noise excitation ratio, it was observed that nine subjects (75.0%) presented altered values, over 0.5; and concerning irregularity, it was observed altered values in all subjects. Table 2 shows the acoustic analysis results concerning jitter, shimmer and glottal to noise excitation ratio.
Table 1. Results of the perceptual analysis: GRBASI scale
Parameters Degree 0 Degree1 Degree 2 Degree 3 p-value
n % n % n % n %
G 0 0 0 0 5 41.6 7 58.3
R 0 0 1 8.3 5 41.6 6 50.0
B 1 8.3 2 16.6 3 25.0 6 50.0 0.000*
A 12 100 0 0 0 0 0 0
S 0 0 0 0 4 33.3 8 66.6
I 0 0 4 33.3 3 25.0 5 41.6
Significant values (p≤0.05) – Chi-square test
All phonatory deviation diagrams were altered: 10 (83.0%) were in the right upper quadrant and two (16.6%) were in the right lower quadrant, both with increased and vertical density. Regarding the quality of life protocols, it was possible to verify that, of the five subjects (41.5%) that assessed their voices as good, four presented brute scores over 80 and one presented score below 49. For six subjects (50%) who classified their voices as reasonable, two presented elevated score (over 80) and four were between 50 and 79. In summary, 50% of the
subjects presented brute scores compatible to dysphonic voices. As regards to the self-assessment of voice, item of V-RQOL protocol, five subjects (41,5%) reported good quality voices, six (50%) classified them as reasonable and one as bad. The coefficient found in the Spearman correlation was 0.3853 and the p-value was p=0.216. The V-RQOL results, with brute scores distributed in three intervals, are presented in Table 3.
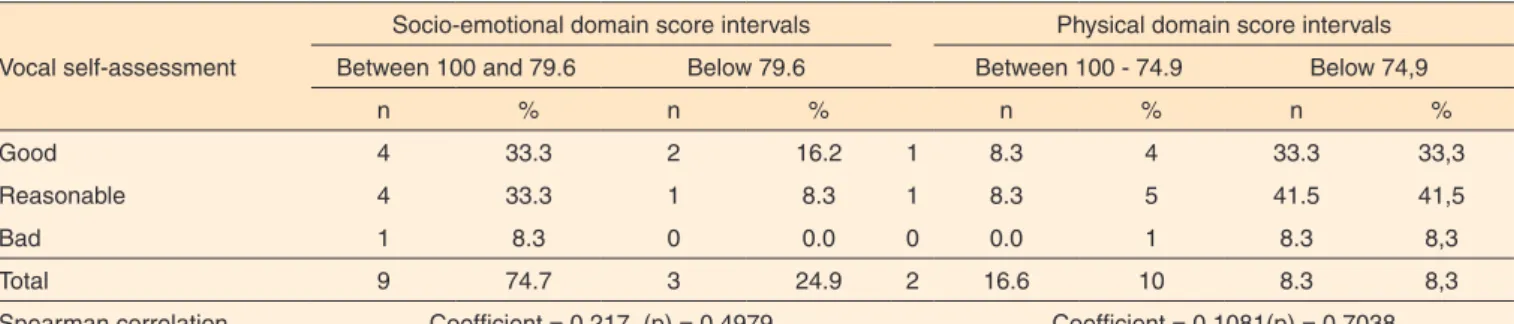
According to a study(9), the socioemotional and physical
domains of V-RQOL may present scores below 70.6 and 62.7 respectively in case of voices considered dysphonic. The ave-rage score of the physical domain was 47.9 and of the socioe-motional domain was 80.7, indicating a propensity for higher prejudice in the physical domain. The Spearman correlation did not show statistical evidences to prove the correlation between the vocal self-assessment and the evaluated domain.
Finally, the question with higher average, pointed by the most subjects as a problem, was question number 1, referring to difficulty in speaking loudly and being heard in noisy environ-ments, with answers varying from 2 to 5. The group average for this question was 3.1. The second question with higher average (2.4) was question 3, “I don’t know how my voice is going to come out when I start speaking”. Table 4 presents scores of V-RQOL concerning the socioemotional and physical domains. Appendix 1 presents the scores of VHI regarding the func-tional, organic and socioemotional domains. Usually, the total score is 120, 40 for each domain. However, in this study, there was a conversion for base 100, as suggested by study(11). The
higher the result, the worse is the disadvantage and, thus, data reveal that two subjects (16.6%) presented scores compatible to dysphonic voices (over 47.4). Specifically in the functio-nal and emotiofunctio-nal domains, three subjects (24.9%) and two
Table 2. Results of acoustic analysis: jitter, shimmer GNE ratio
Subject
Fundamental Frequency
(F0) Hz
jitter shimmer GNE ratio
1 182.79 5.48 26.36 0.16
2 159.64 1.76 16.96 0.22
3 104.25 3.02 17.43 0.37
4 Non
extracted
16.85 38.97 0.2
5 101.75 18.86 47.71 0.45
6 256.76 13.57 49.5 0.59
7 Non
extracted
16.47 47.65 0.4
8 91.59 14.67 26.68 0.09
9 179.77 17.01 29.72 0.2
10 134.16 4.12 21.84 0.67
11 134.34 0.24 8.02 0.95
12 260.05 16.47 46.13 0.28
Averages 160.51 10.71 31.41 0.38
Note: GNE = glottal to noise excitation ratio
Table 3. Comparison between scores of V-RQOL and Vocal self-assessment
Interval of scores of V-RQOL
Self-assessment of vocal quality
Spearman Correlation
Good Reasonable Bad
n % n % n %
100 - 80 4 33.3 2 16.6 0 0.0
Coefficient=0.3853 p=0.216
79-50 0 0.0 4 33.3 1 8.3
Below 49 1 8.3 0 0.0 0 0.0
Total 5 41.6 6 50.0 1 8.3
Table 4. Results of socio-emotional and physical domains of the V-RQOL protocol associated to the subjects’ vocal self-assessment
Vocal self-assessment
Socio-emotional domain score intervals Physical domain score intervals
Between 100 and 79.6 Below 79.6 Between 100 - 74.9 Below 74,9
n % n % n % n %
Good 4 33.3 2 16.2 1 8.3 4 33.3 33,3
Reasonable 4 33.3 1 8.3 1 8.3 5 41.5 41,5
Bad 1 8.3 0 0.0 0 0.0 1 8.3 8,3
Total 9 74.7 3 24.9 2 16.6 10 8.3 8,3
Spearman correlation Coefficient = 0.217 (p) = 0.4979 Coefficient = 0.1081(p) = 0.7038
subjects (16.6%), respectively, presented scores compatible to dysphonic voices. In the organic subscale, no subjects pre-sented such score.
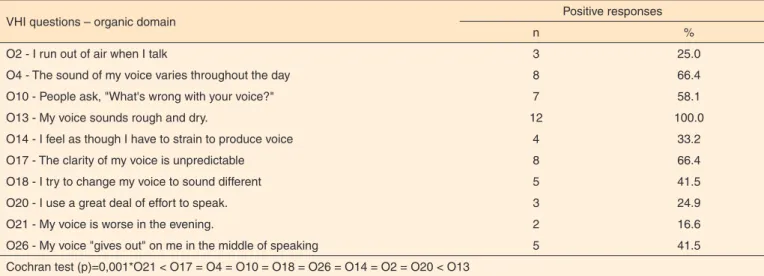
The organic domain was chosen to be highlighted as the one presenting higher number of positive responses among subjects. Positive responses were: 2 “sometimes”, 3 “almost always” and 4 “always”. Questions with responses “never” or “almost never” were discarded. It was observed that questions O4, O10, O13 and O17 presented higher indexes of positive responses, varying from 58.1% to 100%. The Cochran test showed statistical significance. Question O13 had a number of positive responses significantly higher than the other questions. Finally, it can be highlighted that the functional domain of the VHI had 39 positive responses, the organic domain, 57 and the emotional domain, 30. Table 5 shows results of VHI regarding the organic domain.
DISCUSSION
The sample of subjects enrolled in this study was constituted by male patients from 46 to 71 years of age, mean age of 59.3 years, in agreement with the literature that indicates a higher predominance of male patients(1,3).
The perceptual analysis revealed predominance of overall degree of vocal deviation between moderate to intense, reaffir-ming the study that verified, through the GRBASI scale, that most patients (75%) submitted to LSC presented degree 3 of vocal deviation(13).
The rough quality of voice found in the study group also agreed with a study that involved 13 subjects submitted to par-tial laryngectomy with vocal deviation degree from moderate to intense, undergoing speech therapy previously to the study(14).
This condition may be present in organic dysphonias, including the ones caused by neoplasms(17). Breathiness may affect the
voice intensity(17,18) and it is also associated to glottal closure
conditions. Such findings of perceptual analysis empower the results obtained by both protocols of quality of life used in this study, in which most subjects pointed difficulties related to the use of voice intensity. Considering the V-RQOL, question 1, related to the difficulty in speaking loudly and being heard in noisy situations, was pointed by all subjects. The VHI questions from the functional domain (F3 and F12), regarding difficul-ties to be heard in noisy environments and be asked to repeat oneself, were also pointed by most subjects.
Strained quality of voice was found from moderate to inten-se degrees in all subjects, mostly due to the effort to speak(20),
and irregularity was found in all voices, varying from mild to intense. The strained voice is an unpleasant voice characterized by restrict vibration of vocal cords mucosa and exaggerated contraction of the laryngeal vestibules(14), and there may be
breaks in the sonority(18). According to a study performed
with patients submitted to supracricoid laryngectomy, the supraglottic voice acquired, besides the expected roughness, also presents strain and breathiness, and patients complain of tiredness when speaking(20)..
Authors of studies performed with patients submitted to partial laryngectomy point that all subjects were pleased with their voices(14), partially agreeing with the results of the present
study, since most of them classified their voices as reasonable or good, and only one subject judged his/her voice as bad.
The acoustic evaluation of voices revealed that almost all subjects presented altered jitter measures. According to a study, measures of jitter identify short-time frequency disturbance, and tend to be higher in cases of vocal cords disorder(19). This
was observed in this study, once only one subject presented this parameter within the normality range, and the average of the group was 10.71.
Regarding the shimmer, parameter that identifies long-term amplitude disturbance, a study indicates that it is frequently associated to noise in vocal production and tend to be higher
Table 5. Voice handicap index: subjects’ positive responses for organic domain
VHI questions – organic domain Positive responses
n %
O2 - I run out of air when I talk 3 25.0
O4 - The sound of my voice varies throughout the day 8 66.4
O10 - People ask, "What's wrong with your voice?" 7 58.1
O13 - My voice sounds rough and dry. 12 100.0
O14 - I feel as though I have to strain to produce voice 4 33.2
O17 - The clarity of my voice is unpredictable 8 66.4
O18 - I try to change my voice to sound different 5 41.5
O20 - I use a great deal of effort to speak. 3 24.9
O21 - My voice is worse in the evening. 2 16.6
O26 - My voice "gives out" on me in the middle of speaking 5 41.5
Cochran test (p)=0,001*O21 < O17 = O4 = O10 = O18 = O26 = O14 = O2 = O20 < O13
in cases of breathiness(19). Again, there is a relation with the
present study, once subjects presented altered values regarding this parameter, also agreeing with the perceptual analysis that pointed out breathiness for most voices. Laryngectomy, even the partial ones, result in important vocal disorders once there are changes in the histological and geometrical architecture of the glottis, reflecting in the jitter and shimmer expression, and thus the sound produced is normally accompanied by roughness and breathiness(12), which was expressively pointed out in the
perceptual analysis, as previously discussed.
The phonatory deviation diagram allows the two-dimen-sional description and the graphic demonstration of vocal characteristics related to irregularity of the sound wave(21). In
the horizontal axe, there are three parameters associated to irre-gularity of the sound wave (jitter, shimmer and correlation co-efficient), and in the vertical axe, the glottal to noise excitation ratio (GNE). In the present study, all voices were distributed in the lower right and upper right quadrants, confirming a research that verified that voices with worse degree of deviation were distributed in these same quadrants(21).
The analysis of the V-RQOL and VHI responses suggests lower expectations regarding the quality of life when a subject is facing a larynx neoplasm diagnosis(22). Nevertheless, it was
observed that the V-RQOL revealed scores compatible to dys-phonic voices for half of the subjects of this research.
Analyzing the responses given to the V-RQOL protocol, it was observed that subjects submitted to supracricoid laryngeal surgery presented greater impairment in their quality of life related to the physical domain. Such fact was evidenced by questions: “difficulty to speak loudly or to be heard in noisy si-tuations”, pointed by 91.3% of subjects as a problem, “clarity of the voice is unpredictable”, reported by 66.4%, and “having to repeat oneself in order to be understood”, mentioned by 58.1%. The total score of the V-RQOL varied from 42.5 to 95.0. Thus, it is possible to infer that the impact of dysphonia after supracricoid laryngectomy upon quality of life presented important variation among subjects. It should be highlighted that literature shows that the way that a voice problem is felt is very complex and changes from one subject to another(9,23).
Concerning the self-assessment of voice, 91.3% of subjects reported positive responses, considering their voices good or reasonable. This fact agrees with the literature that indicates reduction of the impact on quality of life when comparing subjects submitted to partial and to total laryngectomy(8,10,14).
The VHI showed predominance of the organic domain, followed by the functional, and the lowest mean score obser-ved in the emotional domain. Through this protocol, it was observed that the majority of the group did not present scores compatible to dysphonic voices, except from two subjects with higher scores. However, when verifying question by question, difficulties of the organic nature emerged, implying in quality of life despite the scores. The whole group (12 subjects) pointed question O13 as a problem, regarding the self-perception of the
voice as “rough and dry”. Questions O4 and O17 were pointed by 66.6% of the group, regarding “the voice sound varies throu-ghout the day” and “the clarity of the voice is unpredictable”. Such questions outline the subjects’ difficulties in dealing with their vocal limitation on a daily basis. The perceptual analysis consolidated such fact, since almost all subjects felt roughness in moderate and intense degrees. This consonance strengthens the importance of perceptual analysis performed by the spe-cialist, and the listening to the patient’s impressions regarding his/her own voice(24). It seems clear that, even though subjects
classified their voices as reasonable or good, they also felt they were altered by referring “voice rough and dry” and “varying throughout the day” (question O4), and “unpredictable clarity of the voice” (question O17). Nevertheless, perhaps the fact that subjects knew they had larynx cancer may have lead them to see their vocal limitations under another prism, thus presenting a higher satisfaction index regarding their voice, considering it reasonable or good.
The alterations realized by subjects, however, did not lead them to affirm that the voice problem “limits their lives”, since question F16, that investigates this aspect, was reported by only three subjects (24.9%). Subjects also did not affirm that “my voice makes me feel incompetent” (E29) or “I’m ashamed of my voice problem”, responses presented by only one subjects in each question.
Although literature review(24,25) has concluded that “none of
the quality of life tools currently used in the voice field contem-plates the essential criteria for its development”, a qualitative analysis of questions from V-RQOL and VHI may enable an understanding by the clinician of the dimension involved in its different aspects that may compromise quality of life of dysphonic people.
In this study, the validity of knowing the voice related qua-lity of life of subjects submitted to partial laryngectomy resided much more in the individual analysis of questions rather than in the final score of the protocols. When analyzing questions with higher scores individually, it is possible to realize where the subjects’ difficulties are present, even if the overall scores are not suggestive of significant impairment of quality of life, as seen in this study.
CONCLUSION
The perceptual voice analysis of this study’s subjects reveals moderate and intense degrees of deviation, confirming acoustic analysis, in which the studied parameters were fairly altered, and the phonatory deviation diagram revealed predominance of voices in the right upper quadrant, compatible to highly impaired voices. Nevertheless, despite such analysis, subjects classified their voices as reasonable and good.
limitations due to the larynx malignant neoplasm surgery, especially when there is a correlation between questions of the quality of life protocols and other speech evaluations.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the Head and Neck Service of the Maternity Hospital Celso Pierro, Pontifícia Universidade Católica de Campinas, represented by PHD Professor José Francisco Salles Chagas.
REFERENCES
1. Rodrigues RB, Motta RR, Machado SMS, Cambruzzi E, Zettler EW, Zettler CG, et. al. Valor prognóstico da correlação imunoistoquímica do Ki-67 e p53 em carcinomas epidermóides da laringe. Rev Bras Otorrinolaringol. 2008;74(6):855-9.
2. INCA. Instituto nacional do Câncer. Laringe. [Internet] 2013 [citado 2013 Out 31]. Disponível em: http://www2.inca.gov.br/wps/wcm/ connect/tiposdecancer/site/home/laringe.
3. Dedivitis RA, França CM, Mafra ACB, Guimarães FT, Guimarães AV. Características clínico-epidemiológicas no carcinoma espinocelular de boca e orofaringe. Rev Bras Otorrinolaringol. 2004;25;70(1):35-40.
4. Braz DSA, Ribas MM, Dedevits RA, Nishimoto IN, Barros APB. Quality of life and depression in patients undergoing total and partial laryngectomy.Clinics. 2005; 60(2):135-42.
5. Marioni G, Marchese-Ragona R, Ottaviano G, Staffieri A. Supracricoid laringectom: is it time to define guidelines to evaluate functional results? A review. Am J Otolaryngol. 2004;25(2):98-104. 6. Nemr NK, Carvalho MB, Köhle J, Leite GCA, Rapoport A,Szeliga
RMS.Estudo funcional da voz e da deglutição na laringectomia supracricóide. Rev Bras Otorrinolaringol. 2007;73(2):151-55. 7. Ganly I, Patel SG, Matsuo J, Singh B, Kraus DH, Boyle J, et
al. Analysis of postoperative complications of open partial laryngectomy. Head Neck. 2009;(31)3:338-45.
8. Silva A, Abrahão V, Rudnicki T. A inter-relação entre qualidade de vida e adequação social em laringectomizados. Rev SBPH. 2009;(12)1:17-30.
9. Gasparini G, Behlau M. Quality of life: validation of the Brazilian version of the Voice-Related Quality of Life (V-RQOL) measure. J Voice. 2009;23(1):76-81.
10. Kasama ST, Brasolotto AG. Percepção vocal e qualidade de vida. Pró-Fono. 2007;(19)1:19-28.
11. Behlau M, Oliveira G, Santos LMA, Ricarte A. Validação no Brasil de protocolos de auto-avaliação do impacto de uma disfonia. Pró-Fono. 2009;21(4):326-32.
12. Makeieff M, de la Breteque A, Guerrier B, Giovanni A. Voice handicap evaluation after supracricoid partial laryngectomy. Laryngoscope. 2009;119(4):746-50.
13. Saito K, Araki K, Ogawa K, Shiotani A. Laryngeal function after supracricoid laryngectomy. Otolaryngology Head Neck Surg. 2009;140(4):487-92.
14. Köhle J, Camargo Z, Nemr K. Análise perceptivo-auditiva da qualidade vocal de indivíduos submetidos a laringectomias parciais verticais pela auto-avaliação dos indivíduos e pela avaliação fonoaudiológica. Rev CEFAC. 2004;6(1):67-76.
15. Gama ACC, Santos LLM, Sanches NA, Côrtes MG, Bassi IB. Estudo do efeito do apoio visual do traçado espectrográfico na confiabilidade da análise perceptivo-auditiva. Rev CEFAC. 2011;13(2):314-21. 16. Hirano M. Clinical examination of voice. New York: Springer Verlag;
1981. p. 81-4.
17. Colton RH, Casper JK, Leonard R. Compreendendo os problemas de voz: uma perspectiva fisiológica ao diagnóstico e ao tratamento. Rio de Janeiro: Revinter; 2010.
18. Behlau M, Rodrigues S, Azevedo R, Gonçalves MI, Pontes P. Avaliação e terapia de voz. In: Lopes Filho OC. Tratado de Fonoaudiologia.São Paulo: Roca; 1997.
19. Beber BC, Cielo CA. Características vocais acústicas de homens com voz e laringe normais. Rev CEFAC. 2011;13(2):340-51.
20. Fouquet ML, Vieira TPG, Murata CJM, Gonçalves AJ. Efeito imediato da técnica de firmeza glótica nas laringectomias parciais horizontais supracricoides: estudo inicial. Rev Soc Bras Fonoaudiol. 2012;17(3):346-50.
21. Madazio G, Leão S, Behlau M. The phonatory deviation diagram: a novel objective measurement of vocal function. Folia Phoniatr Logop. 2011;63(6):305-11.
22. Oridate N, Homma A, Suzuki S, Nakamaru Y, Suzuki F, Hatakeyama H, et al. Voice-related quality of life after treatment of laryngeal cancer. Arch Otolaryngol Head Neck Surg.2009;135(4):363-8. 23. De Lima MAG, Barbosa LNF, Sougey EB.Avaliação do impacto na
qualidade de vida em pacientes com câncer de laringe. Rev SBPH. 2011;14(1):18-40.
24. Branski RC, Cukier-Blaj S, Pusic A, Cano SJ, Klassen A, Mener D, et al. Measuring quality of life in dysphonic patients: a systematic review of content development in patient-reported outcomes measures. J Voice. 2010;24(2):193-8.
Appendix 1. Scores of the Voice Handicap Index protocol: Brute, Functional, Organic and Emotional
Subjects Brute score Functional domain Organic domain Emotional domain
1 6.7 1.7 5.0 0.0
2 23.3 5.0 15.8 2.5
3 13.3 3.3 6.7 3.3
4 8.3 1.7 3.3 3.3
5 17.5 5.0 10.0 2.5
6 50.0 18.3 15.0 16.7
7 33.3 11.7 14.2 7.5
8 7.5 0.0 7.5 0.0
9 46.7 19.2 20.8 6.7
10 55.0 19.2 20.8 15.0
11 23.3 5.8 8.3 9.2
12 15.0 6.7 5.0 3.3
Averages 25.0 8.1 11.0 11.0