REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
MISCELLANEOUS
Do
the
severity
and
the
body
region
of
injury
correlate
with
long-term
outcome
in
the
severe
traumatic
patient?
Maylin
Koo
∗,
Israel
Otero,
Antoni
Sabaté,
Ruben
Martínez,
Augusto
Mauro,
Pilar
García,
Silvia
López
BellvitgeBiomedicalResearchInstitute,L’HospitaldeLlobregat,Spain
Received16August2012;accepted20March2013 Availableonline8October2013
KEYWORDS
Injuryseverityscore;
Abbreviatedinjury
score;
ShortForm-12;
HealthAssessment
Questionnaire; Outcome; Trauma
Abstract
Backgroundandobjectives: ToinvestigateiftheInjurySeverityScore(ISS)andtheAbbreviated InjuryScore(AIS)arecorrelatedwiththelong-termqualityoflifeinseveretraumapatients.
Methods:Patientsinjuredfrom2005to2007withanISS≥ 15weresurveyed16---24monthsafter injury.TheHealthAssessmentQuestionnaire(HAQ-DI)wasusedformeasuringthefunctional statusandtheShortForm-12(SF-12) wasusedfor measuringthehealth statusdividedinto itstwocomponents,thePCS(PhysicalComponentSummary)andtheMCS(MentalComponent Summary).TheresultsofthequestionnaireswerecomparedwiththeISSandAIScomponents. ResultsoftheSF-12werecomparedwiththevaluesexpectedfromthegeneralpopulation.
Results:Seventy-fourpatientsfilledthequestionnaires(responserate28%).Themeanscores were:PCS42.6± 13.3;MCS49.4± 1.4;HAQ-DI0.5± 0.7.Correlationwas observedwiththe HAQ-DIandthePCS(Spearman’sRho:−0.83;p<0.05)andnocorrelationbetweentheHAQ-DI andtheMCSneitherbetweentheMCSandPCS(Spearman’sRho=−0.21;and0.01respectively). Thecutaneous-externalandextremities-pelvicAISpunctuationwerecorrelatedwithThePCS (Spearman’sRho:−0.39and−0.34,p<0.05)andwiththeHAQ-DI(Spearman’sRho:0.31and 0.23;p<0.05).Thephysicalconditioncomparedwiththeregularpopulationwasworseexcept forthegroupsagedbetween65---74and55---64.
Conclusions:Patientswithextremitiesandpelvicfracturesaremorelikelytosufferlong-term disability.Theseverityoftheexternalinjuriesinfluencedthelong-termdisability.
©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](M.Koo).
Introduction
In 1976 the American College of Surgeons Committee on
Trauma categorized hospitals in Trauma-Centers; in
con-sequence since then a decrease of mortality has been
recognized.1However,other questionsarousedsuchasthe
long-term quality of life and outcome improvement of
traumapatients.2
In1999aninternationalconsensusconferenceremarked
theheterogeneityoftheavailableinstrumentsforthe
mea-surementofthequalityoflife.3,4 Severaltools havebeen
used:theShortForm-36questionnaire(SF-36)andtheShort
Form-12questionnaire(SF-12),theGlasgowOutcomeScale,
theFunctionalIndependenceMeasure,theQualityof
Well-beingScale, theHannover Score for Polytrauma Outcome
andtheEuroQOL-5D.2,5---7Each oneof themhasits
advan-tages and limitations, but none of them measure all the
dimensions that involve health status in trauma patients.
Aquestionnaireshouldsatisfythefollowingrequirements:
understandable,briefnessonitsaccomplishmentand
anal-ysis, validation in different languages, being of public
domain,lowcostuseandvalidatedforautoadministration
via e-mailor regularmailandbypersonalor phone
inter-view.Inaddition,itshouldhaveaworldwidediffusiontobe
abletoestablish comparisonsbetweendifferentgroupsof
patients indifferent countries.Basedonthese
character-isticsthereare twoquestionnaireswhich have been used
frequently:theHealthAssessmentQuestionnaire-Disability
Index(HAQ-DI)andtheSF-12.
The HAQ-DI questionnaire was initially used for
assessing rheumatic diseases,8,9 and afterwards
subse-quently extended to any kind of condition.10 The HAQ-DI
canberealizedinlessthan5min;ithasbeentranslatedto
morethan60differentlanguagesandvalidatedforitsuse
bytelephone.TheSF-12questionnaireisalsovalidatedto
beadministeredbytelephoneanditneedsonly2mintobe
finished.Itwasinitiallydesignedtorepresentthesummary
componentsoftheSF-36witha90%ofprecision,which
com-pletelyovercame11andithasbeenusedintheevaluationof
patientswhosuffered multipletrauma, pelvictraumatism
orworkplaceinjuries.12---16
Recent guidelines have been published by the
Euro-pean Consumer Safety Association17 grading the disability
of trauma patients, in base on a systematic review and
expert’sopinion.Fourdifferentassessingpointshavebeen
described:theacutephasewithinthefirstmonth;the
reha-bilitationphase,till2months;theadaptationphase,atthe
fourthmonth,andtherecoveryphase,upto6months.
Thehealthandqualityoflifeafterdischargehavebeen
associated to age, sex, comorbidity, the severity of the
traumatism and thelength of stay at the hospital.6,7,18---20
The severity of the traumatism is stratified according to
the Injury Severity Score index (ISS) which correlates to
mortality.21TheISSisananatomicalscoringsystembasedon
theAbbreviatedInjuryScale(AIS)thatgraduatesthe
sever-ityofthe injuriesin differentanatomicalregions.22 When
theISSis greaterthan 15asevere traumapatientcan be
predicted.23
Theaimofourstudywastodetermineifthelong-term
healthstatusofseveretrauma,measuredbytheHAQ-DIand
theSF-12correlatewiththeextendedinjuriesmeasuredby
theISS.
Methods
AfterHospitalEthicsCommitteeapproval,adatabasewas
created. All trauma patients who were attended in our
traumacenterdue toablunt orpenetrating injurywithin
theyears2005---2007were included.Patientswhohadan
ISS≥15,withan age ≥18 yearsandwhowere discharged
from the hospital were followed up. The data collected
werethedemographiccharacteristicsofpatients,thetype
ofinjury,theISS,andtheAIS.
The HAQ-DI questions were grouped into 8 categories
(dressing,rising,eating,walking,hygiene, reach,gripand
usual activities), each category was scored from 0 to 3
(0:without anydifficulty;1: withsome difficulty;2: with
much difficulty; 3: unable to do); afterwards the
aver-age of the 8 categories wasmade to obtain the score of
thequestionnaire. In case of the patient needing help or
using special devices on any of the categories a
correc-tion factor was applied. At least 6 of the 8 categories
must be answered or the questionnaire cannot be
com-puted. Scores were classified as 0 meaning no disability,
0---1milddisability,1---2moderatedisabilityand2---3severe
disability.8,9
TheSF-12included8categories(physicalfunction,
phys-icalrole, emotional role, social function, mental health,
generalhealth,bodypainandvitality).Thenumericalscore
obtainedineachcategorywascalculatedbythesumofthe
items,andconvertedtoascalefrom0(worstscore)to100
(bestscore).11Theresultsweredividedintotwomain
com-ponents,thePhysicalComponentSummaryandtheMental
Component Summary both validated in the Americanand
theSpanishpopulation,obtainingsimilarsummary
compo-nentweightsforbothpopulations.24Therearetwowaysof
estimating the summary components: the standard which
referstodatafromUSA, andthe specific where thedata
usedreferstoeach countryin particular; we selectedde
standardformasitisrecommendedforinternational
publi-cations.Summarycomponentswerecreatedreflectingthe
standard deviation from the average with a value of 50.
It wasconsidered a normal health status ifthe values of
thesummarycomponentswerebetween40and60;limited
healthstatusifthevalueswerebelow40;andgoodhealth
statusifthevalueswereabove60.
The results obtained with the SF-12 were compared
withthose expected from the general population,
strati-fiedaccordingtoage.Thepoweroftheeffectsizeofeach
populationwascalculated.
Thequestionnaireswereperformed16---24months
post-injury,by trained personnel via telephone; ifthe patient
didnotanswerthephoneatthefirstcall,threeextracalls
weremadeinmorning,afternoonandeveningtimes.Losses
infollowupwereconsideredifitwasnotpossibletogetin
touchwiththepatientorthepatientdidnotwanttoanswer
thesurveys.
The statistical analysis was performed using the SPSS
WIN15.0package.WeusedtheChi-squaretest(Yates
cor-rectionandFisherexact test) tocompare theproportions
ofrespondersandnon-responders. TheKruskal---Walliswas
used to compare the categorized scores of the different
questionnaires. The Spearman test was used to compare
therelationshipbetweenqualityoflifewiththeISSandthe
AIScomponents.The effectsizewasusedtocomparethe
scoresofthe responderswiththatof thereference
popu-lation.Dataareshownasmeanandstandard deviationor
medianandrangewhenindicated.Avalueofp≤0.05was
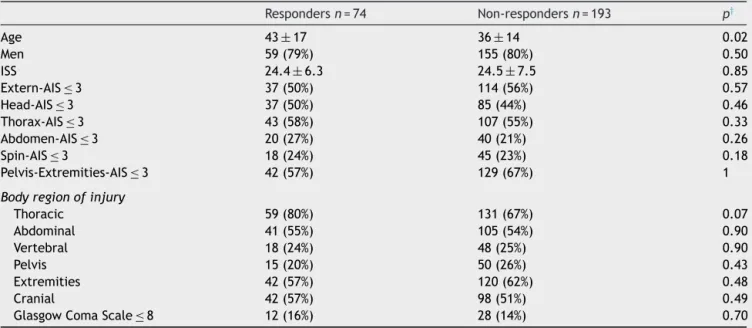
Table1 ComparisonofdemographiccharacteristicsandAISvaluesbetweenrespondersandnon-responderstothesurveys.
Respondersn=74 Non-respondersn=193 p†
Age 43±17 36±14 0.02
Men 59(79%) 155(80%) 0.50
ISS 24.4±6.3 24.5±7.5 0.85
Extern-AIS≤3 37(50%) 114(56%) 0.57
Head-AIS≤3 37(50%) 85(44%) 0.46
Thorax-AIS≤3 43(58%) 107(55%) 0.33
Abdomen-AIS≤3 20(27%) 40(21%) 0.26
Spin-AIS≤3 18(24%) 45(23%) 0.18
Pelvis-Extremities-AIS≤3 42(57%) 129(67%) 1
Bodyregionofinjury
Thoracic 59(80%) 131(67%) 0.07
Abdominal 41(55%) 105(54%) 0.90
Vertebral 18(24%) 48(25%) 0.90
Pelvis 15(20%) 50(26%) 0.43
Extremities 42(57%) 120(62%) 0.48
Cranial 42(57%) 98(51%) 0.49
GlasgowComaScale≤8 12(16%) 28(14%) 0.70
ISS,InjurySeverityScore;AIS,AbreviatedInjuryScale. † Statistic
2;dataexpressedasmean±standarddeviation,absolutevaluesand(percentage).
Results
A total of 267 patients with an ISS≥15 were discharged
from the hospital. In 160 cases there were no answers
becauseoferroneoustelephonenumberormorethanthree
callswithout response;24 patients refusedtoanswer the
questionnaires; in 5 cases there were an idiomatic
bar-rier; in 2 cases the patient had passed away and in 2
casesthemedicalconditionmadeimpossibleansweringthe
questionnaires.A total of 74 patients filledthe
question-naires.
Comparingthepatientswhoansweredthequestionnaires
withthosewhodidnot,thenon-responderpopulationwere
younger(36±14vs.43±17; p=0.02).Therewereno
dif-ferencesin thedemographicdata,theinjuredanatomical
regionsandintheAISregistered(Table1).
Themedianscoresandrangeswere46(11.8---60.9)forthe
PhysicalComponentSummary;51(12.9---74.2)fortheMental
ComponentSummary,and0.12(0---3)fortheHAQ-DI.
The ISS values were comparablefor thedifferent
cat-egories of the HAQ-DI and for the physical and mental
summarycomponentsoftheSF-12(Table2).
We obtained a negativecorrelation between the
HAQ-DI and the physical component of the SF-12 (Spearman’s
Rho=−0.83;p=0.000)andnocorrelationbetweenthe
HAQ-DI and the mental component of the SF-12 (Spearman’s
Rho=−0.21; p=0.07), neither between the mental and
physical componentsof the SF-12(Spearman’sRho=0.01;
p=0.9).
Analyzing the AIS components of the ISS (Table 3) we
found a significant negative-correlation between the PCS
andthe cutaneous-externalscore of theAIS andwiththe
extremities-pelvicscore.Likewise,wefoundpositive
signif-icantcorrelationofthesetwoscoreswiththeHAQ-DI;and
apositivecorrelationbetweenthePCSandthe
abdominal-pelviccontentsscoreoftheAIS.Therewasalsoacorrelation
betweentheAbdomenAISandthepelvicextremities
(Spear-man’sRho=−0.35;p=0.002).
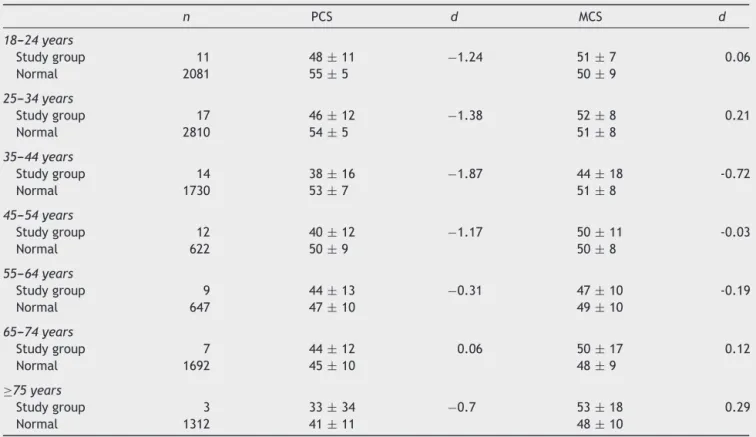
Whencomparingthephysicalandmentalhealthstatusof
ourtraumapatientswiththenormalvaluesofpopulation,
weobservedthatthephysicalconditionwasgloballyworse
inallageintervals,exceptinpatientsagedbetween55---64
and65---74,wheretheeffectsizewassmaller.Regardingto
thementalhealthstatus,thevaluesobtainedshowedamild
differenceintheintervalbetween35and44years,where
thementalhealthstatuswaslowerthanthenorm(Table4).
Table2 RelationbetweenlevelsoftheHealthAssessment Questionnaire,thePhysicalComponentSummaryofthe SF-12 andthe MentalComponentSummaryoftheSF-12with theISS(injuryseveritystore).
n ISS Pa HAQ-DI
Nodisability 36 26.5(16---45)
Milddisability 21 21(16---38) 0.22 Moderatedisability 12 23(17---34)
Severedisability 5 22(17---34)
PCS
GoodHealthStatus 3 16(16---26) 0.15 NormalHealthStatus 42 26(16---45)
LimitedHealthStatus 29 22(17---34)
MCS
GoodHealthStatus 12 21.5(17---29)
NormalHealthStatus 50 25(16---45) 0.68 LimitedHealthStatus 12 24(16---34)
HAQ-DI,HealthAssessmentQuestionnaire;PCS,Physical Compo-nentSummaryoftheSF-12;MCS,MentalComponentSummary oftheSF-12.
Dataexpressedasmedianandrange.
Table3 CorrelationbetweentheHealthAssessment Ques-tionnaire, the Physical Component Summary of the SF-12 andtheMentalComponentSummaryoftheSF-12withthe AbbreviatedInjuryScorecomponents.
PCSa MCSa HAQa
ISS 0.06 −0.09 −0.13
AIS-External −0.39* 0.01 0.31*
AIS-Head 0.09 −0.05 −0.05 AIS-Thorax 0.06 −0.12 −0.14 AIS-Abdomen 0.28* −0.54 −0.20
AIS-Spine −0.17 −0.05 0.12 AIS-Pelvis-Extr −0.34* 0.09 0.23*
PCS --- 0.01 −0.83*
MCS 0.01 --- −0.21
ISS,InjurySeverityScore;AIS-Pelvis-Ext,ExtremitiesandBony pelvis;AIS-Abdomen,Abdomenandpelviccontents;PCS, Physi-calComponentSummaryoftheSF-12;MCS,MentalComponent Summary ofthe SF-12; HAQ-DI, Health Assessment Question-naire.
a RhoofSpearmanCorrelation. * p≤0.05.
Discussion
After the application of the HAQ-DIand the SF-12to our
patients, we obtained values in the lower health status
range,with worse valuesin the physical component than
in the mental component. We evaluated the health
sta-tus 16---24 months post-injury; therefore the low values
obtainedweremeasuredafteralong periodof
rehabilita-tion.Themeasureofthelong-termqualityoflifeintrauma
patients should be considered when a complete
rehabili-tationisachieved.According tosomeauthors17,25 after12
monthsfrominjury a highpercentage of patientsshowed
afull recovery of their lesions.However, it is considered
bettertoevaluatethehealth statusafter24monthsfrom
thetraumatism,inordertoassureastablesituationofthe
disabilities.2,19
We couldnotobserveany relation betweenthe health
status and the ISS values. The ISS is based on
anatomi-calinjuries;for thisreasonanassociation tohealthstatus
can be expected. Nevertheless, the results of our study
were in accordance with the results published by other
authors.12,13,18,26However,someassociationbetweentheISS
andthephysicalcomponentofthelong-termhealthstatus14
andwiththeglobalqualityoflifeevaluated2---7yearsafter
thetraumatism,7hasbeen observed,aswellasarelation
oftheISSwiththephysicalcomponentofthequalityoflife
measuredimmediatelyaftertheinjury.13 Theglobal
inter-pretationofoppositepapersisdifficultandresultsarenot
comparable because of the different questionnaires used
andthedifferenttimeofmeasurement.
Wefoundasignificantcorrelationbetweenthelong-term
qualityoflifemeasuredtwicethroughthePhysical
Compo-nentSummaryandtheHAQ-DIwiththecutaneous-external
component and the extremities-pelvic ring component of
theISS.Therewasnorelationofthesetwocomponentswith
Table4 EvaluationoftheeffectsizeofthestudygroupwiththenormalpopulationmeasuredbytheSF-12.
n PCS d MCS d
18---24years
Studygroup 11 48± 11 −1.24 51± 7 0.06
Normal 2081 55±5 50±9
25---34years
Studygroup 17 46± 12 −1.38 52± 8 0.21
Normal 2810 54±5 51±8
35---44years
Studygroup 14 38±16 −1.87 44±18 -0.72
Normal 1730 53± 7 51± 8
45---54years
Studygroup 12 40±12 −1.17 50±11 -0.03
Normal 622 50± 9 50± 8
55---64years
Studygroup 9 44± 13 −0.31 47± 10 -0.19
Normal 647 47±10 49±10
65---74years
Studygroup 7 44± 12 0.06 50± 17 0.12
Normal 1692 45±10 48±9
≥75years
Studygroup 3 33± 34 −0.7 53± 18 0.29
Normal 1312 41± 11 48± 10
PCS,PhysicalComponentSummaryoftheSF-12;MCS,MentalComponentSummaryoftheSF-12;d,effectsizeofCohen(d=0.20---0.3 smalleffect;d=0.50mediumeffect;d≥0.80largeeffect).
theMentalComponent Summary.The associationbetween
pelvicand extremitiesinjuries withthe long-term quality
of life has been described by other authors,12,18,27
never-theless,theassociationwiththecutaneousregionhasnot
been recognized.The correlation of thecutaneous scores
withthelong-term qualityoflife canbe interpretedasa
reflection of theseinjuries by themagnitude of the
frac-turesintheextremities.Similarly,wewereabletoassociate
theAIS punctuations of the abdomen component andthe
pelvicringinjurywhichindicatestheassociationofserious
pelvicfractures withthe presenceof traumatized vessels
andotherintra-abdominalinjuries.Wealsofounda
corre-lationbetweentheabdominalcomponentoftheISSandthe
PhysicalComponentSummary,butnotwiththeHAQ-DI.
The correlation between the HAQ-DI and the Physical
ComponentSummary oftheSF-12; reinforcesthephysical
disabilityinourpatients.TheMentalComponentSummary
valuesofthe SF-12werenotcorrelated withthe physical
disabilitymeasuredbytheHAQ-DI.Thereforeboth
question-nairesaremeasuringdifferentcomponentsofthedisability
andit reinforcesthe importance of usingcomplementary
questionnairesfor measuringthe health status.The
HAQ-DI includes evaluation of precise movements and motor
activities of the upper and lower extremities.8---10,28
Nev-ertheless one of the weak points of this questionnaire is
thatitdoesnotmeasurethedisabilityrelatedtopsychiatric
problems,affectationofsensoryorgans,andsatisfactionof
thepatientorsocialintegration.Thesedeficienciescanbe
complementedwiththeapplication oftheSF-12
question-nairetakinginconsiderationbothsummarycomponents,the
physicallycomponentandthemental.
When comparedthe healthcondition ofourpopulation
withthepopulationstandard norms,weobservedthatthe
PhysicalComponent Summary valueswerelower thanthe
norm,andthisdifferencewashigherinthepopulationunder
54yearswhopresentedaworsephysicalstatus.Polinderet
al.,19 verifiedthat patients,onageunder65,presenteda
worselong-term quality of lifethan the older group,and
thatit wasinfluenced by thepresence of other illnesses.
Livingston et al.5 found a weak correlation of the health
statuswithage,buttheyalsopointedthatthepopulation
above65yearsevaluatedtheirqualityoflifeasbetterand
thismightberelatedtoalessexpectationabouthealththan
theyoungerpopulation.
The low response rate is one of the limitations of our
study,beingthispercentagevariableaccordingtothe
liter-atureandrangingbetween21%and88%.19,29Thisvariability
dependsonthemethodology used,12,14 but normally
long-term outcome studies, like ours, have a low response
rate.Polinder etal.19 at 24monthsfollow-upregistereda
responserateof21%.Inourstudy,wefoundnodifferences
in the trauma characteristics of the respondersand
non-responders, expecting therefore similar outcome in both
populations.
Weconclude,thatdeterminingthelong-termqualityof
life might help to identify those patients in whom there
wouldbenecessarymoreeffortandemphasisinthe
reha-bilitationandadjustmentprocesses;andalsomayhelp to
detectpreventiveapproachesdirectedtodiminishthe
post-traumaticdisability. Inourpopulation,thosewhosuffered
extremitiesand pelvic fracturesare morelikely tosuffer
long-termdisabilityandtheseverityoftheexternalinjuries
are also predictive for long-term disability of traumatic
patients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MacKenzieEJ,Rivara FP,Jurkovich GJ,NathensAB, FreyKP, EglestonBL,SalkeverDS,ScharfsteinDO.Anationalevaluation oftheeffectoftrauma-centercareonmortality.NEnglJMed. 2006;354:366---78.
2.Stalp M, Koch C,Ruchholtz S, et al. Standardized outcome evaluationafterbluntmultipleinjuriesbyscoringsystems:a clinicalfollow-upinvestigation2yearsafterinjury.JTrauma. 2002;52:1160---8.
3.Neugebauera E, Lefering R, Bouillonb B, Bullingerc M, Wood-Dauphineed S. Quality of life after multiple trauma. Aim and Scope of the Conference Restor Neurol Neurosci. 2002;20:87---92.
4.NeugebaueraE,BouillonbB,BullingercM,Wood-DauphineedS. Qualityoflifeaftermultipletrauma----summaryand recommen-dationsoftheconsensusconference.RestorNeurolNeurosci. 2002;20:161---7.
5.LivingstonDH,TrippT,BiggsC,LaveryRF. Afateworsethan death?Long-termoutcomeoftraumapatientsadmittedtothe surgicalintensivecareunit.JTrauma.2009;67:341---9. 6.HolbrookTL,HoytDB,AndersonJP.Theimportanceofgender
on outcome after major trauma: functional and psycho-logic outcomes in women versus men. J Trauma. 2001;50: 270---3.
7.Ulvik A, Kvale R, Wentzel-Larsen T, Flaatten H. Quality of life2---7years aftermajortrauma.Acta AnaesthesiolScand. 2008;52:195---201.
8.BruceB,FriesJF.TheHealthAssessmentQuestionnaire(HAQ). ClinExpRheumatol.2005;23:S14---8.
9.Bruce B, Fries JF. The Stanford Health Assessment Ques-tionnaire:dimensionsand practicalapplications.HealthQual Life Outcomes. 2003;1:20, this article is available from: http://www.hqlo.com/content/1/1/20
10.GillenM, Jewell SA, Faucett JA, Yelin E. Functional limita-tionsandwell-beingininjuredmunicipalworkers:alongitudinal study.JOccupRehab.2004;14:89---105.
11.VilagutG,FerrerM,RajmilL,RebolloP,Permanyer-MiraldaG, QuintanaJM,SantedR,ValderasJM,RiberaA,Domingo-Salvany A,AlonsoJ.TheSpanishversionoftheShortForm36Health Survey:adecadeofexperienceand newdevelopments. Gac Sanit.2005;19:135---50.
12.KielyJM,BraselKJ,WeidnerKL,GuseCE,WeigeltJA. Predict-ingqualityoflifesixmonthsaftertraumaticinjury.JTrauma. 2006;61:791---8.
13.BraselKJ,Roon-CassiniT,Bradley.Injuryseverity andquality oflife: whose perspective is important?J Trauma.2010;68: 263---8.
14.Harris IA, Young JM, Rae H, Jalaludin B, Solomon MJ. Pre-dictors of general health after major trauma. J Trauma. 2008;64:969---74.
15.GillenM, Jewell SA, Faucett JA, Yelin E. Functional limita-tionsandwell-beingininjuredmunicipalworkers:alongitudinal study.JOccupRehabil.2004;14:89---105.
16.TottermanA, GlottT, SøbergHL,Madsen JE,Røise O.Pelvic traumawithdisplacedsacralfracturesfunctionaloutcomeat oneyear.Spine.2007;3:1437---43.
studies measuring injury-related disability. J Trauma. 2007;62:534---50.
18.HoltslagHR,PostMW,LindemanE,VanderWerkenC.Long-term functional health statusof severely injuredpatients. Injury. 2007;38:280---9.
19.PolinderP,VanBeeckF,Essink-Bot MK,ToetH, LoomanCW, Mulder S, Meerding WJ. Functional outcome at 2.5, 5, 9, and 24 months after injury in the Netherlands. J Trauma. 2007;62:133---41.
20.HolbrookTL,HoytDB, AndersonJP.The impactofmajor in-hospitalcomplicationsonfunctionaloutcomeandqualityoflife aftertrauma.JTrauma.2001;50:91---5.
21.GuzzoJL,BochicchioGV,NapolitanoLM,MaloneDL,MeyerW, ScaleaTM.Predictionofoutcomesintrauma:anatomicor phys-iologicparameters?JAmCollSurg.2005;201:891---7.
22.LinnSh. Theinjury severity score-importanceand uses.Ann Epidemiol.1995:440---6.
23.BoydCR, TolsonMA,CopesWS. Evaluatingtrauma care:the TRISSmethod. Traumascore andtheinjury severityscore.J Trauma.1987;27:370---8.
24.VilagutG,ValderasJM,FerreraM,GarinaO,López-GarcíaE, Alonso J. Interpretaciónde los cuestionarios de saludSF-36 y SF-12 en Espa˜na: componentes físico y mental. MedClin. 2008;130:726---35.
25.Currens B. Evaluation of disability and handicap following injury.Injury.2000;31:99---106.
26.Palma JA, Fedorka P, Simko LC. Quality of life experi-encedbyseverelyinjuredtraumasurvivors.AACNClinIssues. 2003;14:54---63.
27.Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB. Outcomeaftermajortrauma:dischargeand 6-month follow-up results from the Trauma Recovery Project. J Trauma. 1998;45:315---23.
28.WildnerM,SanghalO,ClarckDE,DöringA,ManstettenA. Inde-pendent livingafterfracturesin theelderly.OsteoporosInt. 2002;13:579---85.