http://www.sci-africpublishers.org
Full Length Research Paper
Functional Ability in Institutionalized Elders in
Northeastern Brazil
*Ivana Daniela César
1, Maria Vieira de Lima Saintrain
2, Carlos Roberto Silveira Corrêa
1, Siulmara
Cristina Galera
2, Suzanne Vieira Saintrain
2, Anya Pimentel Gomes Fernandes Vieira
3.
1
State University of Campinas, 2University of Fortaleza, 3Researcher at Oswaldo Cruz Foundation
*Corresponding Author’s e-mail: [email protected]
Accepted April 14th, 2015
---ABSTRACT
Demographic changes are happening all over the world. As both the proportion of older people and the length of life increase, key questions arise. The institutionalization grows according to the increased life expectancy, significantly increasing the need for care, which is not always carried out effectively, leaving many elders without adequate monitoring and consequently with poor health. Authors emphasize that the feeling of helplessness, often triggered by institutionalization, may give rise to situations where lack of care fosters dependence making it useful and necessary to investigate the functionality of this population. Therefore, the objective of this study was to compare the data on the functional status of elders in 2007 with those obtained in 2010 in a long-term care institution. A cohort study conducted with institutionalized elders in two stages. The first assessment occurred from April to June 2007; the second stage from August to October 2010. Data were obtained through: (a) a questionnaire on socio-demographic data and general health (b) Katz Scale of Independence in Activities of Daily Living; (c) Pfeffer`s Functional Assessment questionnaire. Data were analyzed using the Statistical Package for the Social Sciences 19.0 (SPSS Co., Chicago, USA) with a significance level of 5%. Of all the 190 elders in the initial study, 106 remained and were assessed in the two periods of the research. In the first study, ages ranged from 60 to 103 years (mean 74.0 ±9.9) and in the second from 63 to 106 years (mean 77.5 ±9.2). Prevalent diseases were: hypertension (27.3%), dementia (17.9%) and diabetes mellitus (8.5%). The data from the years 2007 and 2010 showed statistical difference in activities like: bathing (p=0.005), transferring (p=0.008), eating (p=0.003), handling medicines (p=0.032), able to walk alone (p=0.031) and could be safely left alone (p=0.046). Conclusively, In a 3-year period, the decrease in functional performance of daily activities, besides being influenced by the process of aging and chronic degenerative diseases, may also be influenced by the strong welfare of institutionalization that prevents the implementation and performance of daily activities of elders with a consequent decrease in their quality of life.
Key words: Epidemiology, Functioning, Elderly, Activities of Daily Living, Institutionalization.
---BACKGROUND
Demographic changes are happening all over the world. As both the proportion of older people and the length of life increase, key questions arise. Will population aging be accompanied by a longer period of good health, a sustained sense of well being, and extended periods of social engagement and productivity, or will it be associated with more illness, disability, and dependency?
[1]
.The beginning of senior years in developing countries is at age 60. However, it is observed that people with the same
The institutionalization of the elderly population grows according to the increased life expectancy, significantly increasing the
need for care [3], which is not always carried out effectively, leaving many elders without adequate monitoring and consequently
with poorer health if compared to that of the non-institutionalized elders [4].
According to the model of the international Classification of Functioning, Disability and Health (ICF), disability results from the interaction of the dysfunction presented by the person (either organic and/or structure of the body), with the limitation of activities and restriction in social participation, and environmental factors, which can act as facilitators or barriers to the performance of
these activities and participation [5-7].
Indeed, the functional capacity is defined as the ability to perform activities of daily living (ADL) independently and autonomously, including the activities of transference, self-care and participation in recreational and educational activities, i.e., the ability to maintain physical and mental abilities to a life with quality. The best reason for being physically active is that it helps to
maintain an individual’s independence and ability to do the same things through life [7].
Authors emphasize that the feeling of helplessness, often triggered by institutionalization, may give rise to situations where
lack of care fosters dependence [8] making it useful and necessary to investigate the functionality of this population [9].
Therefore, inquiring the conditions of health and functional capacity of elderly Brazilians enables the characterization, measurement and explanation of the profiles and health-disease problems of this population; the identification of their needs and priorities; the evaluation of the impact caused by interventions and also the development of strategies for promotion, prevention and control of health hazards and evaluation of the implementation of these actions.
Based on the foregoing, the objective of this research was to compare the data on the functional status of elders in 2007 with those obtained in 2010 in a long-term care institution for elders.
METHODS
A cohort study conducted at the Long Term Care Institution for Elders (LTCI) Lar Torres de Melo, in Fortaleza- Ceará, Brazil, observing a Comprehensive Geriatric Assessment (CGA), which included Index of Independence in Activities of Daily Living (ADL) and Instrumental Activities of daily living (IADL).
Lar Torres de Melo is a charity institution aimed at providing shelter, medical and social assistance to needy seniors. At the time of the research there were about 220 elders at this institution.
Data were obtained through: (a) questionnaire on socio-demographic data (age, gender) and general health (systemic disease); (b) Katz Index of Independence in Activities of Daily Living adapted to the reality of the study population by Lino et al.
[10]
, which evaluates the performance of six functions, considering the basic ADL (bathing, dressing, toileting, transferring, continence and eating), with scores ranging from 0 to 6 (where 0- corresponds to total independence, 1- dependence to a function and 6 - dependence to all six functions), classifying the elders as independent or dependent; and c) Pfeiffer Functional Activities
Questionnaire [11], which considers the skills in eleven instrumental activities of daily living (IADL) (handling money, shopping,
making coffee and not forgetting to turn off the stove, preparing food, keeping up with community or neighborhood events, paying attention, remembering engagements, handling medications, taking a walk outside the neighborhood without getting lost and staying at home alone safely). This review obeys the following scoring: 0 - ability to develop activity, 1 - presents some difficulty, 2 - needs help, 3 - not capable. Sum score equals to or above six are recommended to indicate possible cognitive impairment.
This study assessed elders living in a long-term care institution in two stages. In the first stage the data collection was performed from April to June 2007 and in the second stage, the same elders were reassessed from August to October 2010. This study was performed in two stages in order to evaluate ADL and IADL in institutionalized elders.
The data were analyzed using the SPSS 19.0 (SPSS Co. Chicago, USA). The statistical analysis was performed using Pearson’s chi-square test with a significance level of 5%.
Without any conflicts of interest, the Ethics Committee of the Federal University of Ceará - Brazil, protocol No. 164/05 - COMEPE, approved the study. An authorization form was signed by the trustee responsible for the LTCI where the research took place, and all participants and/or guardians signed a free consent form.
RESULTS
Of the 190 elders participating in the study, in a period of three years, 56 died and 28 were deinstitutionalized, resulting in a sample of 106 elders who were analyzed in the two periods of the research.
Table 1: Description of the level of dependence for the activities of daily living in elders. Fortaleza, 2007-2010.
Activity Years Independent Need help p-value¹
N % N %
Bathing 2007 88 83.8 17 16.2 0.005
2010 71 67.0 35 33.0
2007 77 73.3 28 26.7
0.114
Dressing up 2010 67 63.2 39 36.8
Toileting 2007 75 71.4 30 28.6 0.203
2010 67 63.2 39 36.8
Transferring 2007 82 78.1 23 21.9 0.008
2010 65 61.3 41 38.7
Continence 2007 72 68.6 33 31.4 0.497
2010 68 64.2 38 35.8
Eating 2007 96 91.4 09 8.6 0.003
2010 81 76.4 25 23.6
1
Chi-square test.
Regarding IADL, the activities handling medications (p= 0.032), being able to walk alone (p=0.031) and being at home alone safely (p= 0.046) were the ones that showed significant differences between the years evaluated with an increased dependence (Table 2).
Table 2: Description of the scoring for instrumental activities of daily living in elders. (Fortaleza, 2007-2010).
Activity years score Average p-value¹
rating
Able to handle money 2007 120 1.14 0.093
2010 155 1.46
Able to go shopping alone 2007 119 1.13 0.056
2010 159 1.50
Able to heat up the water and turn off the stove 2007 137 1.30 0.143
2010 168 1.58
Able to prepare food 2007 139 1.32 0.170
2010 168 1.58
Updated with events 2007 122 1.16 0.224
2010 148 1.40
Able to pay attention, understand and discuss 2007 117 1.11 0.062
news 2010 156 1.47
Able to remember dates, appointments, holidays 2007 118 2.05 0.095
2010 153 1.44
Able to handle medications 2007 157 1.50 0.032
2010 198 1.87
Able to walk alone 2007 102 0.97 0.031
2010 146 1.38
Can be safely left alone 2007 105 1.00 0.046
2010 146 1.38
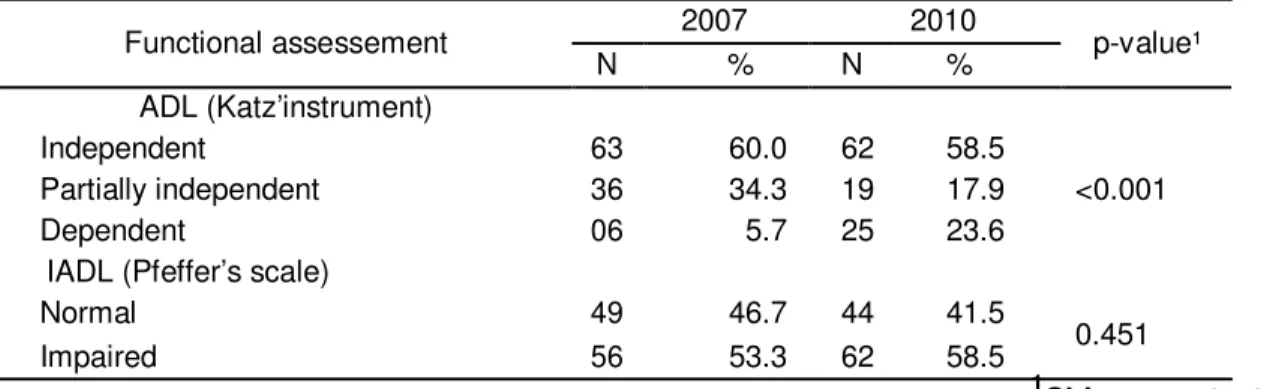
Table 3: Comparative analysis of the functional status – 2007/2010.
Functional assessement 2007 2010 p-value¹
N % N %
ADL (Katz’instrument)
Independent 63 60.0 62 58.5
Partially independent 36 34.3 19 17.9 <0.001
Dependent 06 5.7 25 23.6
IADL (Pfeffer’s scale)
Normal 49 46.7 44 41.5
0.451
Impaired 56 53.3 62 58.5
1
Chi-square test.
Considering the functional status, there was significant difference (p< 0.001) only for ADL evaluated by Katz Index. In instrumental activities evaluated by Pfeiffer Scale, the functional status did not change significantly (p=0.451), although some items had previously demonstrated significant variation (Table 3).
In order to evaluate if there was any baseline difference between those seen again and those lost to follow-up, as well as to investigate if there was any influence by age and sex in the difference seen in the group at the two-study period, a series of statistical tests were performed. Pearson chi-square test was utilized in categorical variables and independent-t-test was used in
continuous variables. It was observed that women participated more in the two evaluations than men (x2; p=0.040); the race was
also different between those who participated in the two evaluation (x2; p=0.047), where white and mulatto were more present in
both moments than yellow and blacks; those who work participated more in both stages of the research than those who do not
work (x2; p=0.050); marital status, know how to read and religion were not different in the group that only participated in the first
stage of the study or participated in both stages (x2; p=0.899, p=0.355 and p=0.645 respectively). Age and years of study also did
not interfere in the participation of elders in the two stages of the research (independent-t-test, p=0.364 and p=0.585 respectively). Of the 190 elders participating in the study, in a period of three years, 56 died and 28 were deinstitutionalized, resulting in a sample of 106 elders who were analyzed in the two periods of the research.
During the first period, age ranged from 60 to 103 years (mean 74.0 ± 9.9), with a predominance of males: 100(52.6%) and in the second period age ranged from 63 to 106 years (mean 77.5 ± 9.2), this time with a female predominance [59 (55.7%)].
The most prevalent diseases were hypertension (27.3%), dementia (17.9%) and diabetes mellitus (8.5%).
Regarding functionality, there was a significant difference in some ADL (bathing, transferring and eating) when comparing 2007 data with those obtained in 2010. There was a significant worsening in these items (Table 1).
Regarding IADL, the activities handling medications (p= 0.032), being able to walk alone (p=0.031) and being at home alone safely (p= 0.046) were the ones that showed significant differences between the years evaluated with an increased dependence (Table 2).
Considering the functional status, there was significant difference (p< 0.001) only for ADL evaluated by Katz Index. In instrumental activities evaluated by Pfeffer Scale, the functional status did not change significantly (p=0.451), although some items had previously demonstrated significant variation (Table 3).
In order to evaluate if there was any baseline difference between those seen again and those lost to follow-up, as well as to investigate if there was any influence by age and sex in the difference seen in the group at the two-study period, a series of statistical tests were performed. Pearson chi-square test was utilized in categorical variables and independent-t-test was used in
continuous variables. It was observed that women participated more in the two evaluations than men (x2; p=0.040); the race was
also different between those who participated in the two evaluation (x2; p=0.047), where white and mulatto were more present in
both moments than yellow and blacks; those who work participated more in both stages of the research than those who do not
work (x2; p=0.050); marital status, know how to read and religion were not different in the group that only participated in the first
stage of the study or participated in both stages (x2; p=0.899, p=0.355 and p=0.645 respectively). Age and years of study also did
not interfere in the participation of elders in the two stages of the research (independent-t-test, p=0.364 and p=0.585respectively).
DISCUSSION
The feminization of the elderly population [12], as already observed by the Brazilian Institute of Statistics and Geography (IBGE),
showing a total of 11,434,487 women and 9,156,112 men in the population above 60 years of life in the country [13], was also
found in this study.
requiring more attention [14]. It is known that the health status score declines with age, and that the score for males is higher than
for females. Women live longer than men on average, but have poorer health status [6] .
As stated in the results, with regards to the prevalence of diseases that affect the population, national and international studies corroborate these findings. In Brazil, studies in two LTCI also found that most prevalent chronic diseases were:
hypertension, mild psychiatric disorders, depression and diabetes mellitus [15]. The study with institutionalized elders in Madrid [16]
and the survey by the National Center for Health Statistics, in order to characterize the residents in LTCI in the United States of
America, found similar data [17]. Knowing that the functional decline of elders is related to chronic illness progression [18] is
possible to propose a link between the chronic diseases and the quality of daily life, which in turn is related to quality of life. Therefore, it is important to focus on the treatment of those illnesses in the elderly population, as it may limit not only their physical capacity, but also their overall well-being.
When analyzing health conditions, there was much difficulty in obtaining data, either by the lack of knowledge of the elders as by the lack of proper registration in medical records, demonstrating the need for a more efficient system of notification and registration in the institution. The prevalence of the reported diseases, which are associated with the lifestyle of the residents, suggests the need of actions directed to healthy living habits, such as medical assistance and social support to assure the control of medicines, exercise for the cognitive function and for functional activities.
It is important to note that most of the patients included in the two periods of the research do not need assistance for ADL, despite demonstrating that as time went by (2007 - 2010), there was a significant increase in the number of dependent elders.
Although most of the residents are considered independent to perform ADL, many of them have their functional performance impaired because professionals and/or caregivers undertake activities for them in order to get better and faster progress in the service – for instance, instead of having the elders take a shower by themselves and helping them only if necessary, professionals/caregivers shower them so that they can finish faster. A research has shown that physical activity is an important
factor for preventing elders from loss of independence [19].
This attitude lies under the reduced number of professionals in LTCI, given the fact that the institution where this research took place has only 17 caregivers (who take turns during day and night for about 220 elders), a fact that certainly happens in other LTCI due to lack of financial resources to meet this demand.
The activities: bathing, transferring and eating showed significant differences in comparison with the two periods studied, a fact found in studies that have verified that bathing is found to be the most dependable activity (76.3%) after nutrition (95%) [20]. Transferring, which is represented by mobility and functional level, i.e., moving from bed to chair and back, is among the most
important and necessary factors for an independent life [21].
At the same understanding, Dawin et al. [22] found that nutrition among institutionalized elders is the activity that showed
greater dependence. However, even at the international level, there is paucity of studies on the causes and factors associated with the decline of functional capacity in LTCIs needed to help understand the process and plan strategies directed to their
detection [18]. According to those authors function decline is common in nursing homes, and are more likely to happen due to
progression of chronic illnesses rather than the developing of acute illnesses. Therefore, prevention of functional decline may be possible through improved management of falls and chronic medical conditions, as well as establishment of rehabilitation and quality care in the homes, which should also be performed in institutions located in Brazil.
The instrumental activities handing medications (p=0.032), able to walk alone (p=0.031) and being at home alone safely (p=0.046) presented a significant difference, showing that the assistentialist profile of the institution jeopardizes the elders empowerment regarding their health/disease process, as well as carrying out their activities freely and on their pace. A research considers the assistencialism of the institution a strong contributing factor to greater remoteness of the social environment and the
consequent tendency to functional dependency [14].
The comparison of the elders’ functional state in 2007 and 2010 enabled the observation of changes in the ability to perform basic activities and instrumental activities of daily living, which are more elaborate and require a more preserved cognitive state. The elderly had an increase in the degree of dependence; however there was a significant difference only for activities of daily living (ADL) (Table 3).
These data contribute to identify the needs and also plan actions for the LTCI, where the inability to perform ADL and IADL is
found to cause institutional problems. This is explained by Guccione [23], who says that more than 90% of institutionalized elders
need help in taking a shower.
Some limitations should be considered in this study. Although its primary goal was to assess the functionality of institutionalized elders in a 3-year period, variables like systemic diseases, fall, depressive symptoms, loneliness, lack of physical activity, among others, were not compared. Likewise, the relationship between curative and preventive actions occurred with the elderly was not assessed during the study period. Additionally, the cause of death of the 56 elders between the two periods of the study could not be identified precisely (as their files have been handed to their families after their death). These are important variables in the functional transitions and deserve further study.
To Maciel and Guerra [24], the elder’s need for assistance to perform basic activities of life, such as eating, bathing,
Finally, it can be concluded that the functional state of institutionalized elders in 2007 and 2010 showed a decrease in functional performance of activities of daily living, mainly by women. The assistentialist nature of the institutionalization may have favored the functional decline of the elderly, whereas the excessive aid has the potential to impede the implementation and performance of daily duties.
The dependency observed highlights the importance of actions that address health education for the elderly and multidisciplinary intervention in order to break the unhealthy lifestyle, progress of chronic-degenerative diseases and consequently the reduction of functionality. Therefore, measures such as the deployment of leisure activities, physical exercises and training of employees should be developed to this group in order to assist them in maintaining their autonomy and independence, hence favoring the delay of functional decline in long-term care institutions.
Thus, it is necessary to formulate institutional strategies to delay that functional decline, prompting the Gerontology and Geriatric class to plan a differentiated care that shall promote improvements for this population.
Competing interests: None
Authors’ Contributions: IDC and MVLS devised the research project, performed data collection, literature review and analysis and composed the letter. CRSC, SCG, SVS and APGFV helped developing the research project, data analysis and final revision of the manuscript.
Acknowledgments: We thank the elders who participated in the research as well as the institution Lar Torres de Melo for permitting this research to take place at their dependencies.
REFERENCES
[1] Suzman R; Beard J. Global Health and Aging (Preface). WHO. National Institute on Aging. National Institutes of Health. NIH Publication 2011; no. 11-7737.
[2] Mazo GZ, Lopes MA, Benedetti TB. Atividade física e o idoso: concepção gerontológica. 2ª ed. Porto Alegre: Sulina, 2004. [3] Reis SCGB, Higino MASP, Melo HMDM, Freire MCM. Condição de saúde bucal de idosos institucionalizados em
Goiânia-GO, 2003. Rev Bras Epidemiol 2005; 8(1):67-73.
[4] Costa, EHM, Saintrain MVL, Vieira APGF. Autopercepção da condição de saúde bucal em idosos institucionalizados e não institucionalizados. Ciência & Saúde Coletiva 2010; 15(6): 2925-2930.
[5] World Health Organization. Active Ageing: A Policy Framework.WHO/NMH/NPH/02.8. Madrid, Spain, April 2002.
[6] World Health Organization. Global Health and Aging. National Institute on Aging.National Institutes of Health.U.S. Department of Health and Human Services. NIH Publication 2011; no. 11-7737.
[7] State Government of Victoria. Well for Life Improving emotional wellbeing for older people in residential aged care Wellbeing, Integrated Care and Ageing Division, Victorian Government Department of Health, Melbourne, Victoria; March 2011. Available: www.health.vic.gov.au/agedcare. Access: April, 2014.
[8] Araújo MO, Ceolim MF. Avaliação do grau de independência de idosos residentes em instituições de longa permanência. Rev Esc Enferm USP 2007; 41(3): 378-85.
[9] Freire Júnior RC, Tavares MFL. A promoção da saúde nas instituições de longa permanência: uma reflexão sobre o processo de envelhecimento no Brasil. Rev Bras Geriat e Gerontol 2006; 9(1): 83-92.
[10] Lino VTS, Pereira SEM, Camacho LAB et al. Adaptação transcultural da Escala de Independência em Atividades da Vida Diária (Escala de Katz). Cad Saúde Pública 2008; 24(1):103-112.
[11] Pfeffer RI, Kurosaki TT, Harrah CH, Chance JM, Filos S. Measurements of functional activities in older adults in the community. J Gerontol 1982; 37:323 – 329.
[12] Nascimento AJR, Rabêlo FCE. Memória e envelhecimento: narrativas sobre questões de gênero e do mundo do trabalho. Soc e Cultura 2008; 11(2): 333-342.
[13] Brasil. Instituto Brasileiro de Geografia e Estatística (IBGE). Sinopse do Censo Demográfico 2010. Ministério do Planejamentoegestão,Brasil.Available:http://www.ibge.gov.br/home/estatistica/populacao/censo2010/default_sinopse.shtmAc ess: Octobre, 2011
[14] Pedrazzi EC, Rodrigues RAP, Schiaveto FV. Morbidade referida e a capacidade funcional de idosos. Cienc Cuid Saude 2007; 6(4): 407-413
[15] Oliveira DLC, Goretti LC, Pereira LSM. O desempenho de idosos institucionalizados com alterações cognitivas em atividades da vida diária e mobilidade: estudo piloto. Rev Bras Fisioter 2006; 10(1): 91-96.
[16] Damián J, Valderrama-Gamab E, Rodríguez-Artalejoc F, Martínmorenod JM. Estado de salud y capacidad funcional de lapoblación que vive em residencias de mayoresen Madrid. Gac Sanit 2004; 18(4): 268-274.
[18] Ang YH, Au SYL, Yap LKP, Ee CH. Functional decline of the elderly in a nursing home. Singapore Med J 2006; 47(3): 219-224.
[19] Hirvensalo M, Rantanen T, Heikkinen E. Mobility difficulties and physical activity as predictors of mortality and loss of independence in the community-living older population. J Am Geriatr Soc 2000; 48(5):493-8.
[20] Pavarini SCI, Neri AL. Compreendendo Dependência, Independência e Autonomia no Contexto Domiciliar: Conceitos Atitudes e Comportamentos. In: Duarte Y, Diogo M. (orgs.), Atendimento domiciliar. Um enfoque gerontológico. São Paulo: Atheneu, 2000. pp. 49-70.
[21] Prata MG, Scheicher ME.Correlação entre o equilíbrio e o nível de independência funcional em idosos. São Paulo Med J 2012; 130(2): 97-101
[22] Davim RMB, Torres GV, Dantas SMM, Lima VM. Estudo com idosos de instituições asilares no município de Natal/RN: características socioeconômicas e de saúde. Rev Latino-Am Enfermagem 2004; 12(3): 518-524.
[23] Guccione AA. Fisioterapia Geriátrica. Tradução José Eduardo Ferreira de Figueredo; Marcelo Alves Chagas. 2ª ed. Rio de Janeiro: Guanabara Koogan, 2002.