0
Index
Abstract
1
1. Introduction
3
1.1. Tumor necrosis factor-alpha Inhibitors
4
1.2. Immunogenicity
5
1.2.1. Anti-drug antibodies
6
1.2.2. Pharmacokinetics
7
1.3. Bridging ELISA
9
2. Aims
10
3. Material and Methods
12
3.1. HTRF principals
13
3.2. Materials
14
3.3. Procedure
15
4. Results
16
4.1. Standard curve
17
4.2. Cut point determination
18
4.3. Infliximab quantification
20
4.4. HTRF and bridging ELISA correlation
21
5. Discussion and Conclusions
23
1
Abstract
Biologic therapies revolutionized the treatment of autoimmune diseases in the last years. Typically, they target important disease mediators. Tumor necrosis factor-alpha (TNF-α) antagonists constitute a very prescribed group of biologic agents as they are indicated for the treatment of common immune-mediated diseases, such as rheumatoid arthritis, juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease and ulcerative colitis. With the increasing use of TNF-α inhibitors it has been noticed that they have an important immunogenic potential that can compromise long-term outcomes in chronically treated patients. The production of anti-drug antibodies seems to cause secondary therapeutic failure in many patients. One of the effects of anti-drug antibodies is the enhancement of drug clearance. Drug clearance, in turn, varies among individuals, reflecting different pharmacokinetic profiles. Determination of serum anti-TNF-α drug trough levels is though very informative and could support treatment decisions. However, immunologic assays to determine drug serum concentrations are not readily available in clinical practice. In order to investigate a potentially reliable and practical new technique for detection and quantification of anti-TNF-α biologic agents, homogeneous time-resolved fluorescence resonance energy transfer (HTRF) technique was tested for determination of serum infliximab concentrations. Although presenting some limitations related with fluorescence reading conditions, this technique proved to give results close to the concentrations obtained by the widely used bridging enzyme-linked immunosorbent assay (ELISA). In addition, it has the advantage of being much easier and faster to perform. Thus, HTRF technique can be optimized and become a valuable laboratorial tool to guide treatment decisions in autoimmune patients with anti-TNF-α therapy failure.
2
Resumo
As terapias biológicas revolucionaram o tratamento das doenças autoimunes nos últimos anos. Tipicamente têm como alvos mediadores importantes no mecanismo das doenças. Os antagonistas do fator de necrose tumoral-α (TNF-α) são um grupo de agentes biológicos muito prescrito, pois estão indicados no tratamento de doenças imuno-mediadas comuns, tais como artrite reumatoide, artrite idiopática juvenil, artrite psoriática, espondilite anquilosante, doença de Crohn e colite ulcerosa. Com o uso frequente de inibidores do TNF-α, tem-se tornado evidente que estes agentes têm um potencial imunogénico importante, que pode comprometer o prognóstico a longo prazo dos doentes cronicamente tratados. A produção de anticorpos anti-fármaco parece causar falência terapêutica secundária em muitos doentes. Um dos efeitos dos anticorpos anti-fármaco é o aumento da eliminação do fármaco. A eliminação do fármaco, por sua vez, varia entre indivíduos, refletindo diferentes perfis farmacocinéticos. A determinação dos níveis séricos mínimos do agente anti-TNF-α é assim muito informativa e pode auxiliar nas decisões terapêuticas. Contudo, os testes imunológicos para determinar as concentrações séricas do fármaco não estão facilmente disponíveis na prática clínica.
De forma a investigar uma nova técnica potencialmente fidedigna e prática para a deteção e quantificação dos agentes biológicos anti-TNF-α, foi testada a técnica por HTRF (homogeneous time-resolved fluorescence resonance energy transfer) para a determinação de concentrações séricas de infliximab. Apesar de apresentar algumas limitações relacionadas com as condições de leitura da fluorescência, esta técnica provou obter resultados próximos das concentrações obtidas por ELISA (enzyme-linked immunosorbent assay) bridging. Adicionalmente, tem a vantagem de ser de execução muito mais fácil e rápida. Deste modo, a técnica por HTRF poderá ser otimizada e tornar-se uma valiosa ferramenta laboratorial para orientar as decisões terapêuticas em doentes autoimunes com falência da terapêutica anti-TNF-α.
3
Introduction
4
1.
Introduction
1.1.
Tumor necrosis factor-alpha inhibitors
Inflammatory rheumatic diseases comprise a variety of conditions and syndromes with diverse degrees of severity, overall provoking poor quality of life and premature death. They are more prevalent in developed countries and constitute a huge burden to health care systems (Helmick 2008, Jacobs 2011). The incidence of inflammatory rheumatic diseases in Western countries is estimated to be 5-7% (Kuek 2007). Biologic therapies brought new perspectives in the treatment of immune-mediated diseases as they block specific targets that are important players in the disease physiopathology. Monoclonal antibodies in particular, used in the treatment of many refractory inflammatory rheumatic diseases, have proved to be effective in the reduction of disease-associated activity scores.
Amongst the biologic therapies, tumor necrosis factor-alpha (TNF-α) blocking drugs are the most prescribed as they constitute a therapeutic option in many immune-mediated diseases, namely rheumatoid arthritis, juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease and ulcerative colitis (Saad 2010). There are five TNF-α inhibitors currently in the Portuguese market (Table 1): 1) infliximab is a chimeric anti-TNF-α immunoglobulin (Ig) G1, 25% murine and 75% human, administered intravenously; 2) adalimumab is a fully human anti-TNF-α IgG1, administered by subcutaneous injection; 3) etanercept is a fully human fusion protein constituted by the fragment crystallisable (Fc) of human IgG1 and the soluble TNF-α receptor, administered by subcutaneous injection; 4) certolizumab is a pegylated fragment antigen binding (Fab) of a humanized anti-TNFα antibody, administered subcutaneously or intravenously; 5) golimumab is a fully human anti-TNF-α IgG1, administered by subcutaneous injection. Infliximab (IFX) was the first of its group getting market approval (Taylor 2010).
5
IFX ADA ETA CZP GLM
Structure Chimeric IgG1 Fully human IgG1 Fully human fusion protein of IgG1 Fc and soluble TNF-α receptor 2 Pegylated Fab of a humanized anti-TNF-α antibody Fully human IgG1 Mechanism of action Neutralizes tmTNF-α and sTNF-α Neutralizes tmTNF-α and sTNF-α Inhibits TNF-α/β and cell surface receptors bounding; inhibits LT-α Neutralizes tmTNF-α and sTNF-α Neutralizes tmTNF-α and sTNF-α
Half-life 8-10 days 10-20 days 3-6 days 11-14 days 7-20 days
Administration route i.v. s.c. s.c. i.v. or s.c. s.c. Dosage for autoimmune diseases 3-10mg/Kg at 0, 2 and 4 weeks and then every 8 weeks 40mg every one or two weeks 50mg once weekly or 25mg twice weekly 400mg at 0, 2 and 4 weeks and then 200mg every 2 weeks or 400mg every 4 weeks 3mg/Kg once monthly
Table 1: Properties of TNF-α inhibitors. IFX – infliximab; ADA – adalimumab; ETA – etanercept;
CZP – certolizumab pegol; GLM – golimumab; TNF – tumor necrosis factor; tmTNF-α – transmembrane TNF-α; sTNF-α – soluble TNF-α; LT – lymphotoxine; i.v. – intravenous; s.c. subcutaneous.
1.2.
Immunogenicity
Although TNF-α blockers dramatically improved the above mentioned disease-related outcomes, some patients do not respond to therapy (primary therapeutic failure) and others experience a loss of efficacy over time (secondary therapeutic failure). Loss of response has been attributed mainly to immunogenicity and drug pharmacokinetics (Pascual-Salcedo 2011, Bartelds 2011). Immunogenicity is also responsible for other adverse events, namely infusion reactions in the case of intravenously administrated drugs and injection site reactions in subcutaneous formulations, thus influencing both efficacy and safety of anti-TNF-α drugs.
6 The core mechanism of immunogenicity is the production of antibodies against TNF-α antagonists. To reduce the immunogenic potential of anti-TNF-α agents, companies decreased its murine content: chimeric anti-TNF-α monoclonal antibody is more immunogenic than fully human anti-TNF-α monoclonal antibodies, and this is more immunogenic than the soluble TNF-α receptor-Fc fusion protein (de Vries 2009, Aikawa 2010, Krieckaert 2012). However, many other factors may contribute to immunogenicity. These factors can be categorized as drug-related and patient/disease-related factors. The main drug-patient/disease-related factors are previous exposure to similar or related proteins, dose and duration of treatment, route of administration (intravenous administration reduces the likelihood of an immune response), and product related drivers (drug post-translational modification, excipients formulation, production and purification processes, storage conditions, structural alterations, immune-complex formation). Patient and disease-related factors are poorly understood, but certain concomitant medications also seem to influence immunogenicity (Kriechaert 2012, Mulleman 2011).
1.2.1. Anti-drug antibodies
Anti-drug antibodies (ADAb) can be neutralizing or non-neutralizing. Neutralizing ADAb reduce drug efficacy through interference with TNF-α binding site (van Schouwenburg 2013). Non-neutralizing ADAb bind to anti-TNF-α agents without interfering with the TNF-α binding site. In this manner they do not directly reduce drug efficacy but they can contribute to therapeutic failure through immune-complex formation. Drug-ADAb immune-complexes also increase the drug clearance rates (van der Laken 2007). In rare cases, conversely, ADAb can prolong drug half-life. Globally, the main effects of ADAb are enhanced clearance and neutralization of therapeutic antibodies, allergic reactions and cross-reactivity with endogenous proteins. Screening of ADAb has been used in preclinical, clinical and post-marketing studies to address immunogenicity. Enzyme-linked immunosorbent assay (ELISA) has been the preferred technique for this purpose. Standard direct and indirect ELISAs were improved and nowadays bridging ELISA is a widely used method. However, there is high variability of ADAb detection
7 among studies and it is not possible to monitor ADAb formation in routine clinical practice. In fact, the method is not yet standardized and has important limitations such as the levels of rheumatoid factor in the serum and the concomitant presence of the anti-TNF-α drug (Aarden 2008, Hart 2011).
1.2.2. Pharmacokinetics
Once ADAb detection techniques are not completely reliable, immunogenicity studies usually include pharmacokinetic data. In fact, several studies showed an inverse relationship between drug levels and ADAb formation: trough levels of TNF-α inhibitors may be lower in patients with ADAb (Wolbink 2006, Bartelds 2007, van Kuijk 2010).
Immunogenicity can have a big impact in long-term outcomes and patients with chronic inflammatory diseases are the most likely to be affected as they are exposed to repeated administrations of the drug, over long periods. Ideally, there should be an individualized treatment planned in accordance with different tools that would allow to assess the likelihood and severity of drug-related immunogenicity, as well as its expected side effects. Such a regimen would allow to determine changes in drug dosage and/or frequency of administration, and even the switch to an alternative biological therapy, either another TNF-α inhibitor or a drug with a different target
(Keystone 2009, Jamnitski 2011). Since drug immunogenicity is closely related to its pharmacokinetics, trough serum drug levels are very informative. Additionally, other factors than immunogenicity, such as gender and body size, influence TNF-α blockers pharmacokinetics (Ordás 2012).
Regarding infliximab, for example, the optimal trough level is not known. The existent evidence shows that infliximab must be always detectable to be therapeutic and some studies suggest that trough levels inferior to 4µg/mL may not be in the therapeutic window (Takeuchi 2009, Seow 2010). Having the limitations of the analytical methods in mind, the available pharmacokinetic data for infliximab can be summarized as follows. After administration of 5 mg/kg of infliximab, the plasma concentration of free
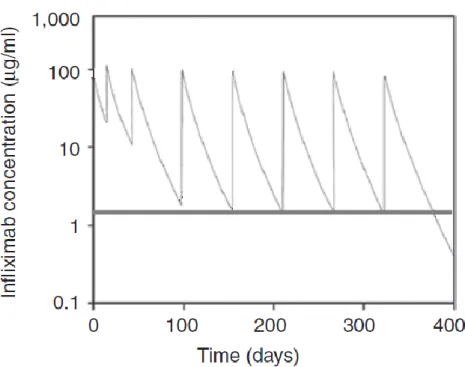
8 infliximab remained in the same order as Cmax (118 µg/ml, range: 71-283 µg/ml) for approximately 24 hours. The concentrations then declined exponentially with a half-life of 8-10 days. Detectable concentrations of free infliximab have been observed for up to 28 weeks (mean 12 weeks) after the recommended dose regimen. Clearance of free infliximab was about 11 ml/h (range 3-40 ml/h). No clinically significant dose or time dependencies have been observed in the pharmacokinetics of free infliximab. There are no specific studies regarding metabolism or excretion of infliximab in humans. Since infliximab can be expected to be eliminated in a similar manner as native antibodies, this is considered to be acceptable. Furthermore, no studies of the pharmacokinetics of infliximab have been performed in patients with impaired organ functions (Zhu 2005, Nestorov 2005, EMEA 2012).
Figure 1: example of concentration vs. time curve of infliximab (adapted from
Ordás 2012). Serum infliximab concentrations below the horizontal line are probably out of the therapeutic window.
9 Since pharmacokinetics and immunogenicity are not predictable, trough drug levels should be measured in each patient serum immediately before periodical drug administration (Rutgeerts 2010). Many authors argue they should be routinely determined (Afif 2010, Ducourau 2011, Plasencia 2012) because it would be benefic for the patients who receive a personalized therapeutic scheme and, given the high costs of biologic therapies, serum drug level monitoring would probably be cost-effective (Krieckaert 2012).
1.3.
Bridging ELISA
Bridging ELISA is the method most frequently used to detect anti-TNF-α drugs and to quantify its levels. It has several advantages as it uses widely available equipment and expertise, and many centers even have automated systems. It is also sensitive and specific. However, bridging ELISA also presents some relevant disadvantages: a) it is not standardized among laboratories (Casteele 2012); b) involves repetitive steps of washing and incubation which are time-consuming and may remove low affinity antibodies. Therefore its use is limited outside research centers.
10
Aims
11
2.
Aims
In order to have optimized therapeutic regimens, pharmacokinetic profile of TNF-α antagonists should be obtained in every patient chronically treated. While this is not a generalized practice in the clinical context, research laboratories conduct pharmacokinetic studies using mainly bridging ELISA to measure serum drug levels. This is a multi-step and time-consuming technique that requires technology expertise. These are probably the reasons why it is not readily available in routine clinical practice.
Considering the pros and cons of bridging ELISA, other methods may prove to be more useful to measure anti-TNF-α drugs in the serum of patients with immune-mediated diseases. HTRF is a technique widely used to study biomolecules interaction, single molecules conformation and cells organization. To date, there is no evidence in the literature of HTRF use for monoclonal antibodies quantification. It is here hypothesized that HTRF can be a new technique for biologic TNF-α antagonists quantification.
The main aim of this work is to demonstrate the proof-of-concept that HTRF can detect and measure infliximab trough levels in the serum of autoimmune patients. Additionally, it is probably easier to perform than the currently used techniques.
12
Materials and Methods
13
3.
Materials and Methods
3.1.
HTRF principals
Fluorescence (or Fӧrster) resonance energy transfer (FRET) is a nonradiative energy transfer that occurs between two fluorescent molecules, a donor and an acceptor. Energy transfer occurs only when the donor and acceptor are close and the energy transfer efficiency (E) is given by the following formula:
E = 1/1+(R/Ro)6
where Ro is the Fӧrster distance (or critical transfer distance) and R is the distance between donor and acceptor.
The energy goes from donor molecules to acceptor molecules through dipole-dipole coupling. The donor is initially in its electronic excited state after being exposed to an energy source, secondly the energy transfer occurs, and finally the acceptor emits flurescence at a given wavelength. The donor element must consist is a macrocyclic lanthanide ion, Europium cryptate (Eu3+cryptate) or Terbium cryptate (Tb2+cryptate). Acceptors consist in small organic structures derived from algae pigments (d2) or in synthetic molecules. The maximum distance that allows the fluorophores to react is dependent on the molecular size and conformation of the labeled molecules. As such, the techniques employing FRET are referred as sensitive, because they are able to detect molecules in close proximity, safe, because they use a nonradiative reaction, and fast to perform, because there is no need for separation steps (e.g. washing). The FRET reaction was further ameliorated and nowadays investigators may use time-resolved FRET (TR-FRET) and homogeneous TR-FRET (HTRF). These improved techniques brought the possibility of eliminating the short-lived background fluorescence related to other sample components, by delaying the fluorescence measurement after excitation.
14 HTRF is currently used, for example, for detection of biomolecular interactions and for single-molecule studies to elucidate conformational changes (Schuler 2008, Piston 2007, Sahoo 2011). It has also being increasingly used in drug development studies due to its potential to discover new therapeutic targets (Degorce 2009).
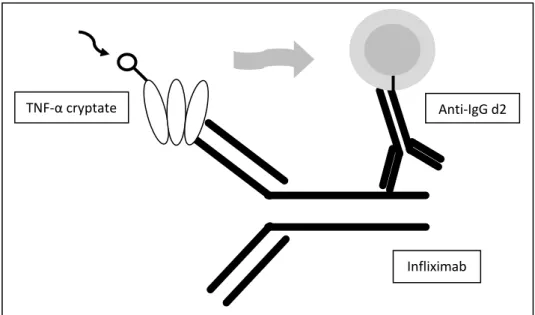
Figure 2: HTRF for detection and quantification of infliximab uses a TNF-α cryptate
donor and a anti-IgG d2 aceptor.
Our assay will be developed for the quantitative determination of anti-IFX antibodies. It is based on the principle of HTRFtechnology, where assays yield a distance-related signal. Anti-IFX antibodies are detected by a system of an anti-human IgG monoclonal antibody (mouse-anti human IgG MAb) and TNF-α, one labeled with d2, the other one with Eu3+ cryptate.
3.2.
Materials
Commercial infliximab (RemicadeTM) was used in successive dilutions to obtain a standard calibration curve. Serum samples from drug-naïve healthy controls and from patients with an autoimmune disease treated with IFX were analysed. The reagents
TNF-α cryptate Anti-IgG d2
15 were provided by Cisbio International (France), and were reconstituted and diluted according to the instructions of the manufacturer (Cisbio: www.htrf.com) in dilution buffer (provided with the kit). For fluorescence readings a Tecan spectrophotometer was used. Tecan’s Infinite F200 is equipped with a sophisticated and ingenious mirror system containing a dichroic mirror with a break point at 510nm, which permits optimal excitation in the UV range and thus enables HTRF measurements in the Infinite F200.
3.3.
Procedure
1- In a 96 well white plate, 5uL of sample, 10 uL of TNF-α cryptate at 50nM concentration, and 10uL of anti-IgG d2 at 50nM concentration were pipetted to each well. Before pipetting, samples were kept cold in an ice recipient and reagents were at room temperature.
2- The plate was maintained at room temperature and protected from direct light until reading. The liquid in the wells remain colorless.
3- Fluorescence was read ten minutes after the addition of reagents by
Tecan Infinite F200. HTRF measurements were set up using the ‘multi labelling’ function of Tecan i-control software. The Eu3+ cryptate (donor) was excited at 320 nm (bandwidth 25 nm). The cryptate and d2 (acceptor) emissions were detected at a wavelenght near 600 nm.
16
Results
17
4.
Results
4.1.
Standard curve
Every method that uses spectrophotometry technology to determine concentrations of a given molecule starts by obtaining a standard curve. This is created through standard concentrations of the study molecule and respective optical density (OD) values. The data is then computed to verify linearity. The resultant formula permits to calculate concentrations from OD values.
To obtain the standard curve, eight successive dilutions of infliximab in the concentration range of 0.39-50 µg/mL were tested (figure 3). The procedure was repeated three times. The OD values obtained show some variability that increase with concentration.
Figure 3: Standard curve of infliximab concentrations. From the graph it can be
seen that doubling infliximab concentration doubles the optical density (OD) values obtained by HTRF. The variation in OD values reflects the three-fold measurements.
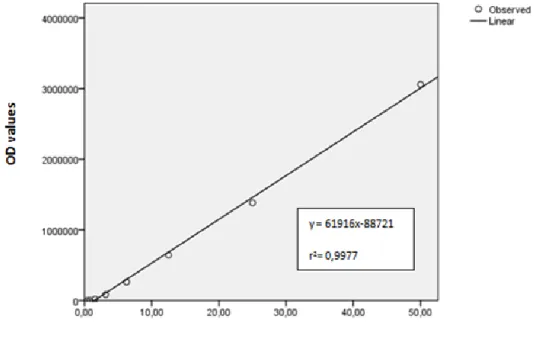
18 Using a linear regression model, a graph was generated to show the relationship between OD values and infliximab concentrations (figure 4). The linear regression curve and the r2 value show linearity.
Figure 4: Linear regression curve. The data were analyzed by a linear regression
model. A positive correlation exists between infliximab concentrations and optical density (OD) values.
4.2. Cut point determination
Ideally, HTRF technique does not emit signal in the absence of infliximab. However, background fluorescence can exist and give positive results. Hence, it is necessary to determine the cut point above which the result is considered positive, using negative controls.
The serum of 31 drug-naïve healthy donors was analyzed in three repetitions and the results are shown in figures 5 and 6. Although HTRF signal is absent, there is also a variation that is probably related with the adaptations made in the fluorescence reader to perform HTRF.
19
Figure 5: Optical density (OD) values of negative controls. Negative controls show OD
values below zero although some variation exists between the three measurements of each sample.
20
Figure 6: Infliximab detection in negative controls. The cut-off value of infliximab
concentration for HTRF detection is zero, as indicated by the dashed line.
4.3.
Infliximab quantification
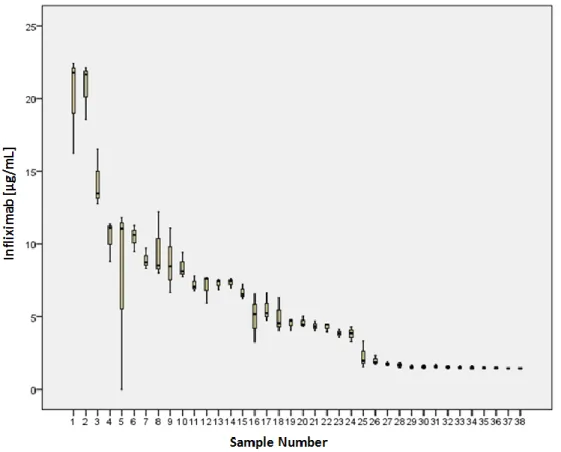
Serum samples containing infliximab previously quantified through bridging ELISA were analyzed by the HTRF technique. The analysis of 34 samples of serum from patients with immune-mediated diseases treated with infliximab gave the trough drug levels (Figure 7). Serums 1-4 are internal positive controls created by dilution of infliximab in infliximab-naïve serum. All the samples were tested three times. As in previous observations, the variation of results is greater in higher infliximab concentrations. Serum 5 showed one variant measurement (zero) that was excluded from calculations.
Figure 7: Infliximab concentrations in positive serums. Sampes 1-4 are internal controls.
21
4.4.
HTRF and bridging ELISA correlation
Globally, HTRF and bridging ELISA infliximab concentrations show a positive correlation (p value < 0.01). The mean levels of serum IFX were slightly higher with bridging ELISA than with HTRF (mean ± SD = 6.13 ± 5.44 vs. 6.63 ± 5.44). Interestingly, the tendency in the positive control samples (samples 1-4) seems to be different from the other samples (Figure 8).
Figure 8: Correlation between HTRF and bridging ELISA measurements of serum
infliximab levels. HTRF – homogeneous time-resolved fluorescence resonance energy transfer. ELISA – enzyme-linked immunosorbent assay.
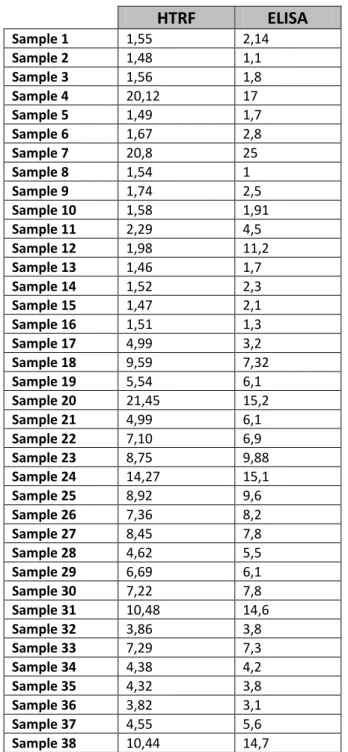
22 HTRF ELISA Sample 1 1,55 2,14 Sample 2 1,48 1,1 Sample 3 1,56 1,8 Sample 4 20,12 17 Sample 5 1,49 1,7 Sample 6 1,67 2,8 Sample 7 20,8 25 Sample 8 1,54 1 Sample 9 1,74 2,5 Sample 10 1,58 1,91 Sample 11 2,29 4,5 Sample 12 1,98 11,2 Sample 13 1,46 1,7 Sample 14 1,52 2,3 Sample 15 1,47 2,1 Sample 16 1,51 1,3 Sample 17 4,99 3,2 Sample 18 9,59 7,32 Sample 19 5,54 6,1 Sample 20 21,45 15,2 Sample 21 4,99 6,1 Sample 22 7,10 6,9 Sample 23 8,75 9,88 Sample 24 14,27 15,1 Sample 25 8,92 9,6 Sample 26 7,36 8,2 Sample 27 8,45 7,8 Sample 28 4,62 5,5 Sample 29 6,69 6,1 Sample 30 7,22 7,8 Sample 31 10,48 14,6 Sample 32 3,86 3,8 Sample 33 7,29 7,3 Sample 34 4,38 4,2 Sample 35 4,32 3,8 Sample 36 3,82 3,1 Sample 37 4,55 5,6 Sample 38 10,44 14,7
Table 2: Serum infliximab concentrations (µg/mL) obtained with HTRF and
bridging ELISA methods. HTRF - homogeneous time-resolved fluorescence resonance energy transfer. ELISA – enzyme-linked immunosorbent assay.
23
Discussion and Conclusions
24
5.
Discussion and Conclusions
Despite being very immunogenic, infliximab is benefic for many patients with immune-mediated diseases. Furthermore, adverse effects associated with immunogenicity are still a matter of debate. Secondary therapeutic failure of long-term treatments seems to be the most challenging problem as it is influenced by many factors and there is still no way to predict it. It is therefore understandable the boom that has characterized research in the immunogenicity of TNF-α inhibitors in the last few years.
To better understand the factors implicated, immunogenicity should be searched for every patient receiving anti-TNF-α biologic therapies. However, this is far from reality. Several authors tried to determine the relationship between immunogenicity and clinical outcomes by performing assays to detect ADAb or through pharmacokinetic studies. The majority of them used bridging ELISA techniques, which are currently only available for use in research laboratories.
For all the reasons stated above, assays for ADAb detection are not reliable predictors of immunogenicity, but pharmacokinetic profiles may be a useful tool to clarify secondary therapeutic failures of anti-TNF-α agents. Thus, it would be very advantageous to find a technique at least as sensitive and specific as bridging ELISA, but faster, simpler to perform, and preferentially cheaper, that would allow periodically to determine drug trough levels in the serum, in every-day clinical practice. Our experiment demonstrates the proof-of-concept for HTRF as a new technique to detect infliximab. Although widely used to study protein-protein interactions and single protein conformations, HTRF was never applied as a monoclonal antibody quantification test. Additionally, it could improve the throughput of pharmacokinetic studies.
In accordance with the criteria for the HTRF Reader Control Kit, the Infinite F200 in combination with the 510 dichroic mirror meets all performance parameters that are relevant for HTRF-compatible readers and is thus regarded as HTRF-certified. In
25 addition, IFX can be reliably and sensitively quantified in the Infinite F200. In summary, the results of the Reader Control Kit, show that the Infinite F200 with an integrated 510 dichroic mirror is a perfectly suited detection instrument for the measurement of various HTRF assays formats.
HTRF results were close to those obtained through bridging ELISA, and the HTRF technique is much easier to perform. However, some unexpected difficulties were found. The main disadvantage of the HTRF technique is the need for fluorescence measurements within 10 minutes after the mixture of the sample with the reagents. This increases the variability of the results and limits the number of samples tested that can be measured in one reading, unless an automated system is available. Another problem initially found was the variability amongst different commercial infliximab samples that were previously submitted to a dialysis procedure. This issue was overcome by using untreated commercial infliximab. Finally, once the correlation between bridging ELISA and HTRF infliximab concentration in the internal positive controls (known dilutions of infliximab in infliximab-naïve serum) seems to vary, there is a possibility that other serum components interfere with HTRF results.
Some of the above mentioned difficulties could be overcome, for example through automated systems, hopefully in a near future. In this way, a HTRF test could give results only minutes after blood collection and easily help in clinical decisions. Exemplifying, if the values of infliximab concentration obtained in this experiment represent infliximab trough levels in patients with therapeutic failure, samples 25-38 could reflect an inefficacy of treatment related with such low values. In this case, infliximab dose escalation would be an option. Conversely, if the remaining samples were from patients with therapeutic failure, dose escalation strategy would not be grounded since infliximab trough levels are high. In this situation the switch to another biologic drug should be equated.
This work is not the first trying to find alternative techniques to bridging ELISA (Wang 2012). However, HTRF had never been experimented for quantification of a monoclonal antibody and seems to be the simplest and the fastest method. As such, it is worth trying to improve HTRF conditions. If optimized and available for routine
26 clinical practice, rapid HTRF tests would help to find efficient drug regimens, to enhance therapeutic success, to reduce adverse events, and eventually to decrease therapeutic-associated costs.
27
References
28
References
Aarden L, Ruuls SR, Wolbink G. Immunogenicity of anti-tumor necrosis factor antibodies – toward improved methods of anti-antibody measurement. Current Opinion in Immunology. 2008; 20:431-435.
Afif W, Loftus EV, Faubion WA, et al. Clinical utility of measuring infliximab and human anti-chimeric antibody concentrations in patients with inflammatory bowel disease. American Journal of Gastroenterology. 2010; 105:1133-1139.
Aikawa ME, Freire de Carvalho J, Almeida Silva CA, Bonfá E. Immunogenicity of Anti-TNF-α Agents in Autoimmune Diseases. Clinical Reviews in Allergy and Immunology. 2010; 38:82-89.
Alpha B, Lehn J, Mathis G. Energy transfer luminescence of europium (III) and terbium (III) cryptates of macrobicyclic polypyridine ligands. Angewandte Chemie International Edition in English. 1987; 26(3):266-267.
Bartelds GM, Krieckaert CL, Nurmohamed MT, et al. Development of antidrug antibodies against adalimumab and association with disease activity and treatment failure during long-term follow-up. The Journal of American Medical Association. 2011; 305(14):1460-1468.
Bartelds GM, Wijbrandts CA, Nurmohamed MT, et al. Clinical response to adalimumab: relationship to antiadalimumab antibodies and serum adalimumab concentrations in rheumatoid arthritis. Annals of the Rheumatic Diseases. 2007; 313:578-585.
Casteele NV, Buurman DJ, Sturkenboom MGG, et al. Detection of infliximab levels and anti-infliximab antibodies: a comparison of three different assays. Alimentary Pharmacology and Therapeutics. 2012; 36(8):765-771.
Committee for Medical Products for Human Use (CHMP), European Medicines Agency (EMA), Assessment report – infliximab, 2012 (Procedure: EMEA/H/C/000240/II/0150).
29 Degorce F, Card A, Soh S, et al. HTRF: a technology tailored for drug discovery – a review of theoretical aspects and recent applications. Current Chemical Genomics. 2009; 3:22-32.
de Vries MK, van der Horst-Bruinsma IE, Nurmohamed MT, et al. Immunogenicity does not influence treatment with etarnecept in patients with ankylosing spondylitis. Annals of the Rheumatic Diseases. 2009; 68(4):531-535.
Ducourau E, Mulleman D, Paintaud G, et al. Antibodies toward infliximab are associated with low infliximab concentration at treatment incitiation and poor infliximab maintenance in rheumatic diseases. Arthritis Research and Therapy. 2011; 13:R105.
Hart MH, de Vrieze H, Wouters D, et al. Differential effect of drug interference in immunogenicity assays. Journal of Immunological Methods. 2011; 372:196-203.
Helmick CG, Felson DT, Lawrence RC, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States – Part I. Arthritis and Rheumatism. 2008; 58(1):15-25.
Jacobs P, Bissonnette R, Guenther L. Socioeconomic Burden of Immune-Mediated Inflammatory Diseases – Focusing on Work Productivity and Disability. The Journal of Rheumatology. 2011; 88:55-61.
Jamnitski A, Bartelds GM, Nurmohamed MT, et al. The presence or absence of antibodies to infliximab or adalimumab determines the outcome of switching to etanercept. Annals of the Rheumatic Diseases. 2011; 70:284-288.
Keystone E, Emery P, Peterfy CG, et al. Rituximab inhibits structural joint damage in patients with rheumatoid arthritis with an inadequate response to tumor necrosis factor inhibitor therapies. Annals of the Rheumatic Diseases. 2009; 68:216-221.
Krieckaert CL, Jamnitski A, Nurmohamed MT, Kostense PJ, Boers M, Wolbink G. Comparison of Long-Term Clinical Outcome With Etanercept Treatment and
30 Adalimumab Treatment of Rheumatoid Arthritis With Respect to Immunogenicity. Arthritis and Rheumatism. 2012; 64(12):3850-3855.
Krieckaert C, Nair SC, Nurmohamed MT, et al. Evaluating the cost-effectiveness of personalized treatment with adalimumab using serum drug level and anti-adalimumab antibodies in rheumatoid arthritis patients. Annals of the Rheumatic Diseases. 2012; 71(Suppl 3):104.
Krieckaert CL, Nurmohamed MT, Wolbink GJ. Methotrexate reduces immunogenicity in adalimumab treated rheumatoid arthritis patients in a dose dependent manner. Annals of the Rheumatic Diseases. 2012; 71:1914-1915.
Kuek A, Hazleman B, Ӧstӧr A. Immune-mediated inflammatory diseases (IMIDs) and biologic therapy: a medical revolution. Postgraduate Medical Journal. 2007; 83(978):251-260.
Mulleman D, Lauféron F, Wendling D, et al. Infliximab in ankylosing spondylitis: alone or in combination with methotrexate? A pharmacokinetic comparative study. Arthritis Research and Therapy. 2011; 13:R82.
Nestorov I. Clinical pharmacokinetics of tumor necrosis factor antagonists. The Journal of Rheumatology. 2005; 74:13-18.
Odrás I, Mould DR, Feagan BG, Sandborn WJ. Anti-TNF monoclonal antibodies in inflammatory bowel disease: pharmacokinetics-based dosing paradigms. Clinical Pharmacology and Therapeutics. 2012. 91(4):635-646.
Pascual-Salcedo D, Plasencia C, Ramiro S, et al. Influence of immunogenicity on the efficacy of long-term treatment with infliximab in rheumatoid arthritis. Rheumatology. 2011; 50(8):1445-1452. Bartelds GM, Krieckaert CL, Nurmohamed MT, et al.
Piston D, Kremers G. Fluorescent protein FRET: the good, the bad and the ugly. Trends in Biochemical Sciences. 2007; 32(9): 407-414.
31 Plasencia C, Pascual-Salcedo D, Nuño L, et al. Influence of immunogenicity on the efficacy of long-term treatment of spondyloarthritis with infliximab. Annals of the Rheumatic Diseases. 2012; 71:1955-1960.
Rutgeers P, Vermeire S, VanAssche G. Predicting the response to infliximab from trough serum levels. Gut. 2010; 59(1):7-8.
Saad A, Ashcroft DM, Watson KD, et al. Improvements in quality of life and functional status in patients with psoriatic arthritis receiving ant-tumor necrosis factor therapies. Arthritis Care and Research. 2010; 62(3):345-353.
Sahoo H. Fӧrster resonance energy transfer – A spectroscopic nanoruler: Principle and applications. Journal of Photochemistry and Photobiology C: Photochemistry reviews. 2011; 12: 20-30.
Schuler B, Eaton WA. Protein folding studied by single-molecule FRET. Current Opinion in Structural Biology. 2008. 18:16-26.
Seow CH, Newman A, Irwin SP, Steinhart AH, Silverberg NS, Greenberg GR. Trough serum infliximab: a predictive factor of clinical outcome for infliximab treatment in acute ulcerative colitis. Gut. 2010; 59:49-54.
Takeuchi T, Miyasaka N, Inoue K, Abe T, Koike T. Impact of trough serum level on radiographic and clinical response to infliximab plus methotrexate in patients with rheumatoid arthritis: results from the RISING study. Modern Rheumatology. 2009; 19:478-487.
Taylor PC. Pharmacology of TNF blockade in rheumatoid arthritis and other chronic inflammatory diseases. Current Opinion in Pharmacology. 2010; 10(3):1-8.
van der Laken CJ, Voskuyl AE, Roos JC, et al. Imaging and serum analysis of immune complex formation of radiolabeled infliximab and anti-infliximab in responders and non-responders to therapy for rheumatoid arthritis. Annals of the Rheumatic Diseases. 2007; 66:253-256.
32 van Kuijk AW, de GM, Stapel SO, et al. Relationship between the clinical response to adalimumab treatment and serum levels of adalimumab and anti-adalimumab antibodies in patients with psoriatic arthritis. Annals of the Rheumatic Diseases. 2010; 3:624-625.
van Schouwenburg PA, van de Stadt LA, de Jong RN, et al. Adalimumab elicits a restricted anti-idiotypic antibody response in autoimmune patients resulting in functional neutralization. Annals of the Rheumatic Diseases. 2013; 72:104-109.
Wang SL, Ohrmund L, Hauenstein S, et al. Development and validation of a homogeneous mobility shift assay for the measurement of infliximab and antibodies-to-infliximab levels in patient serum. Journal of Immunological Methods. 2012; 382:177-188.
Wolbink GJ, Vis M, Lems W, et al. Development of antiinfliximab antibodies and relationship to clinical response in patients with rheumatoid arthritis. Arthritis and Rheumatism. 2006; 54:711-715.
Zhu YW, Pendley C, Sisco D, et al. Pharmacokinetics and pharmacodynamics of infliximab, an anti-tumor necrosis factor-alpha monoclonal antibody, following single subcutaneous administrations in rheumatoid arthritis patients. Clinical Pharmacology and Therapeutics. 2005; 77: 43.