www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Assessment
of
Eustachian
tube
function
in
patients
with
tympanic
membrane
retraction
and
in
normal
subjects
夽
,
夽夽
Inesângela
Canali
a,∗,
Letícia
Petersen
Schmidt
Rosito
a,
Bruno
Siliprandi
a,
Cláudia
Giugno
a,
Sady
Selaimen
da
Costa
baUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bUniversidadeFederaldoRioGrandedoSul(UFRGS),DepartamentodeOftalmologiaeOtorrinolaringologia,PortoAlegre,RS,
Brazil
Received10September2015;accepted17January2016 Availableonline25April2016
KEYWORDS
Eustachian
tube/physiopathology; Ear
dis-ease/physiopathology; Middleear
ventilation/methods; Valsalva maneu-ver/physiology; Analysisofvariance; Child
Abstract
Introduction:ThediagnosisofEustachiantubedysfunctionsisessentialforbetter understand-ingofthepathogenesisofchronicotitismedia.A seriesofteststoassesstubefunctionare describedintheliterature;however,theyaremethodologicallyheterogeneous,withdifferences rangingfromapplicationprotocolstostandardizationoftestsandtheirresults.
Objective:Toevaluatethevariationinmiddleearpressureinpatientswithtympanic mem-braneretraction and innormal patients during tubefunction tests,as well asto evaluate intra-individualvariationbetweenthesetests.
Methods:Anobservational,contemporary,cross-sectionalstudywasconducted,inwhichthe factorunderstudywasthevariationinmiddleearpressureduringtubefunctiontests(Valsalva maneuver,sniff test,Toynbee maneuver)inhealthypatients andinpatients with mildand moderate/severetympanicretraction.A totalof38patients (76ears)were includedinthe study.Patientsunderwenttubefunctiontestsattwodifferenttimepointstodeterminepressure measurementsaftereachmaneuver.StatisticalanalysiswasperformedusingSPSS software, version18.0,consideringp-values<0.05asstatisticallysignificant.
Results:Mean(standarddeviation)agewas11(2.72)years;55.3%ofpatientsweremaleand 44.7% female. The prevalenceoftype A tympanogram was higheramong participants with healthyearsandthosewithmildretraction,whereastypeCtympanogramsweremorefrequent
夽 Pleasecitethisarticleas:CanaliI,RositoLP,SiliprandiB,GiugnoC,daCostaSS.AssessmentofEustachiantubefunctioninpatients withtympanicmembraneretractionandinnormalsubjects.BrazJOtorhinolaryngol.2017;83:50---8.
夽夽Institution:CentrodeOtiteMédiadoBrasil(COM.BR);DepartmentofOtorhinolaryngology,HospitaldeClínicasdePortoAlegre(HCPA), UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](I.Canali).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.010
inthemoderate/severeretractiongroup.Anincreaseinmiddleearpressurewasobserved dur-ingtheValsalvamaneuveratthefirsttimepointevaluatedinallthreegroupsofears(p=0.012). ThevariationinpressurewasnotsignificanteitherforthesnifftestorfortheToynbee maneu-veratthetwotimepointsevaluated(p≥0.05).Agreementbetweenmeasurementsobtainedat thetwodifferenttimepointswasweaktomoderateforalltestsinallthreegroupsofears,and thevariationsindiscrepancybetweenmeasurementswerehigherinearswithmoderate/severe tympanicretraction.
Conclusion: Inthisstudypopulation,themeanpressureinthemiddleearshowedsignificant variationonlyduringtheValsalvamaneuveratthefirsttimepointevaluatedinthethreegroups ofears.Normalearsandthosewithmildretractionbehavedsimilarlyinalltests.Thetested maneuversexhibitedweaktomoderateintra-individualvariation,withthegreatestvariation occurringinearswithmoderate/severeretraction.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
TubadeEustáquio/ fisiopatologia; Doenc¸aotológica/ fisiopatologia; Ventilac¸ãodoouvido médio/métodos; Manobrade Valsalva/fisiologia; Análisedevariância; Crianc¸as
Avaliac¸ãodafunc¸ãodatubadeEustáquioempacientescomretrac¸ãodemembrana timpânicaeemindivíduosnormais
Resumo
Introduc¸ão: Odiagnósticodasdisfunc¸õesdatubaauditivaéessencialparaomelhor entendi-mentodapatogênesedaotite médiacrônica.A literaturadescreveumasériedetestesque avaliam afunc¸ãotubária;contudo,tais examessãometodologicamenteheterogêneos, com diferenc¸asquevariamdesdeosprotocolosdeaplicac¸ãoatéapadronizac¸ãodosexameseseus resultados.
Objetivo: Avaliaravariac¸ãonapressãonaorelhamédiaempacientescomretrac¸ãoda mem-branatimpânicaeemindivíduosnormaisdurantearealizac¸ãodostestesdefunc¸ãotubária,e tambémavaliaravariac¸ãointraindividualdessestestes.
Método: Estudoobservacionaldotipotransversalecontemporâneo,noqualofatoremestudo foiavariac¸ãonapressãonaorelhamédiadurantearealizac¸ãodostestesdefunc¸ãotubária (manobradeValsalva,SniffTestemanobradeToynbee)emindivíduosnormaiseempacientes comretrac¸õestimpânicaslevesemoderadas/graves.Foramincluídos38pacientes(76orelhas). Ospacientesforamsubmetidos,emdoismomentosdiferentes,atestesdefunc¸ãotubáriapara determinarasmedidasdepressãoapóscadamanobra.Aanáliseestatísticafoirealizadacom ousodoprogramaSPSS,versão18.0,econsideramoscomoestatisticamentesignificativosos valoresdep<0,05.
Resultados: Amédia±desviopadrãodaidadefoide11±2,72anos;55,3%dospacienteseram do gêneromasculinoe44,7% pertenciamao gênerofeminino.A prevalência decurvas tim-panométricasdotipoA foimaisaltaentreosparticipantescomorelhasnormaisenaqueles comretrac¸õesleves,enquanto ascurvas timpanométricasdotipoCforammais frequentes nogrupocomretrac¸õesmoderadas/graves.Observamospressõesaumentadasnaorelhamédia durantearealizac¸ãodamanobradeValsalvanoprimeiromomentodaavaliac¸ãonostrêsgrupos deorelhas(p=0,012).Avariac¸ãonapressãonãofoisignificativaparaoSniffTest,nempara amanobradeToynbeenosdoismomentosdeavaliac¸ão(p≥0,05).Consideramosquea con-cordânciaentreasdeterminac¸õesobtidasnosdoismomentosdiferentesfoifracaamoderada paratodosostestesnostrêsgruposdeorelhas,easvariac¸õesemtermosdediscrepânciaentre asmedidasforammaioresnasorelhascomretrac¸õestimpânicasmoderadas/graves.
Conclusão:Napopulac¸ãoestudada,amédiadaspressõesnaorelhamédiaapresentouvariac¸ão significanteapenasduranteamanobradeValsalvanoprimeiromomentodeavaliac¸ão,nostrês gruposdeorelhas.Asorelhasnormaiseaquelasapresentandoretrac¸ãolevesecomportaramde maneirasimilarnostestesrealizados.Asmanobrastestadasexibiramumavariac¸ão intraindivid-ualfracaamoderada,eamaiorvariac¸ãoocorreunasorelhascomretrac¸õesmoderadas/graves. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
Introduction
The Eustachian tube (ET), or auditory tube, is the main structureresponsible for equalizing pressure betweenthe middleearandtheoutsideenvironment,ensuring ventila-tionoftheairspacesofthetemporalbone,andprotecting themiddleearfromnasopharyngealsecretions.1Persistent
ETdysfunction mayproduce negativepressure withinthe tympaniccavity,resultinginashiftofintravascularfluidinto theinterstitialspacesandthenintothemiddleearlumen,2
orcausingretractionofthetympanicmembrane(TM),and is thus one of the earliestlandmarksof the pathogenesis ofchronicotitismedia(COM).3,4Therefore,severalstudies
havepinpointedETdysfunctionasoneofthefactorsfor per-petuationofotitismediawitheffusion(OME),progressionof OMEtomoderateandsevereTMretraction,andprogression ofthelattertochroniccholesteatomatousotitismedia.
The diagnosis of ET dysfunction is therefore essential for a better understanding of COM pathogenesis. Several testsofETfunctionhavebeendescribedintheliterature.5---7
However,thesetestsaremethodologicallyheterogeneousin aspectsranging fromapplicationprotocolsto standardiza-tionoftestsandtheirresults.Hence,thetrueapplicability ofthesetestsisamatterofdebate,particularlyinpatients withquestionable ET patency. The Eustachiantube func-tion(ETF)testsmostcommonlyemployedinpatientswith intactTMincludetheValsalvamaneuver,thesnifftest,and theToynbeemaneuver.1,8,9
The present study sought toassess variationin middle earpressureinpatientswithmildandmoderate/severeTM retractionand healthypatients during ETF tests(Valsalva maneuver, sniff test, and Toynbee maneuver), as well as assessintra-individualvariationinthesetestsinthethree aforementionedpatientgroups.
Methods
This was an observational, cross-sectional, contemporary study. The factor under study was variation in pressure withinthe middle earduring ETF testing in patients with mild TM retraction, moderate/severe TM retraction, or healthyTMs.Thesamplecomprised38patientsaged8---18 years,recruitedfromtheoutpatientotolaryngologyclinicof atertiarycarecenterfromDecember1,2012,toMarch31, 2013.Patientswereallocatedintothreegroupsaccordingto theseverityofparstensaretractionintheworseear,using themodifiedSadéandBerco(1976)classificationproposed byCostaetal.,asfollows:group1---patientswithnormal TMsbilaterally(controls);group2---patientswithmildTM retractioninatleastoneear;andgroup3---patientswith moderateorsevereTMretractioninatleastoneear.
Inclusion criteria for the patient group were: age between 8 and 18 years; mild, moderate, or severe TM retraction in at least one ear; and intact TMs in both ears. The inclusion criteria for controls were: good overall health; same age range as participants in the patient group; current outpatient follow-up for ade-noidectomy or adenotonsillectomy performed at least six months before recruitment; and normal TMs bilaterally. Exclusion criteria for patients and controls were: middle ear effusion; cleft lip and palate or other craniofacial
abnormalities; Down syndrome; mucopolysaccharidoses; immunosuppression-related diseases; nasalor nasopharyn-geal obstruction; inability to undergo audiometry, aural toilet,video otoscopy,orETF tests;andrefusalto partic-ipate.
Allpatients underwenta thorough, targeted interview duringthe firststudyvisit.Videootoscopy wasperformed andrecorded.Findingsweresystematicallydescribedbya senior otologist using a dedicated form. All patients also underwentnasalendoscopyforassessmentof nasopharyn-gealobstruction.Puretoneandspeechaudiometrywasalso performed duringfirstassessment ofallpatients and con-trols.
AssessmentofETFconsistedofthefollowingtests,which were performed withthe Interacoustics AZ26 and AT235h impedance audiometers to measure middle ear pressure after each test maneuver. First, tympanometry was per-formedinbothearstorecordthebaselinepressureineach earpriortotestingandascertainitstypeoftympanogram, according totheJerger (1970)classification.Thiswas fol-lowed by the Valsalva maneuver, sniff test, and Toynbee maneuver, whichwereperformed sequentially,firstin the rightearandthenintheleft.Duringeachtest,middleear pressurewasmeasuredfivetimesconsecutivelyasdescribed below:
Valsalvamaneuver:thepatientwasaskedtoperformfive consecutiveValsalvamaneuvers.Middleearpressurewas measuredandrecordedimmediatelyaftereachmaneuver (VP1---VP5), during which time the patient was asked to refrainfromspeakingorswallowing.
Sniff test: the patient was asked to inhale forcefully throughthenose(mouthclosed)fivetimesconsecutively. Again, middle ear pressure was measured and recorded immediatelyaftereachmaneuver(SP1---SP5),duringwhich time the patient was asked to refrain from speaking or swallowing.
Toynbee maneuver: the patient was asked to swallow a sip of water while his or her nose waspinched shut by theinvestigator,fivetimesconsecutively.Middleear pres-surewasmeasuredandrecordedimmediatelyaftereach maneuver (TP1---TP5),during whichtimethepatientwas askedtorefrainfromspeakingorswallowing.
Betweeneachtest,a5-minuteintervalwasenforcedand thepatientwasinstructedtodrinkwater,inanattemptto returnpressuretobaselinevalues.Baselinepressurebefore each test wasrecorded as well (baselinepressure before Valsalvamaneuver[VBP];baselinepressurebeforesnifftest [SBP];andbaselinepressurebeforeToynbeetest[TBP]).
Alloftheaforementionedtestswereperformedata sec-ond time point of assessment, 15---30 daysafter the first studyvisit.Resultsweredescribedascorrespondingtothe firstorsecondtimepointofassessment.
Quantitative data were expressed asmeans and standard deviations, andcategorical data, asabsoluteand relative frequencies.Analysisofmiddleearpressuremeasurements was based on mixed-effects (fixed and random) models, taking intoaccount intra-subject correlatedobservations, both for ears and for repeated measures. Categorical datawere analyzedby means ofa generalizedestimating equations (GEE) model. The Bland---Altman method and intraclasscorrelationcoefficientswereusedforassessment ofagreementbetweenmeasurements.
Thisstudywasapprovedbytheethicscommitteeofthe GroupofResearchandGraduateStudiesunderNo.12-0432. Aninformedconsentwassignedfor theanonymoususeof patientdatabythelegalguardiansofallparticipants. Treat-mentwasnotaffectedinanywaywhetherpatientsprovided orrefusedinformedconsent.Asthisstudyalsoused histor-icaldataforanalysis,allauthorssigned anagreementfor theconfidentialuseofdata.
Results
Atotalof38participantswereassessed:14healthycontrols, 12patientswithmildTMretractioninatleastoneear,and 12patientswithmoderate/severeTMretractioninatleast oneear.Separateanalysisofeachearrevealed36healthy ears,23earswithmildretraction,and17earswith moder-ate/severeretraction.Meanageandstandarddeviation(SD) was11(2.72)years(range,8---17years).Patientdistribution accordingtosexwas55.3%maleand44.7%female.
The prevalence of type A tympanogram was higher in groups 1and2,whereastypeCtympanogramsweremost commoningroup3,atbothtimepointsofassessment.There weresignificantdifferencesamongthethreegroupsatthe first and second time points of assessment (p=0.002 and p<0.001,respectively,chi-squaredtest).
Eustachiantubefunctiontests
Valsalvamaneuver
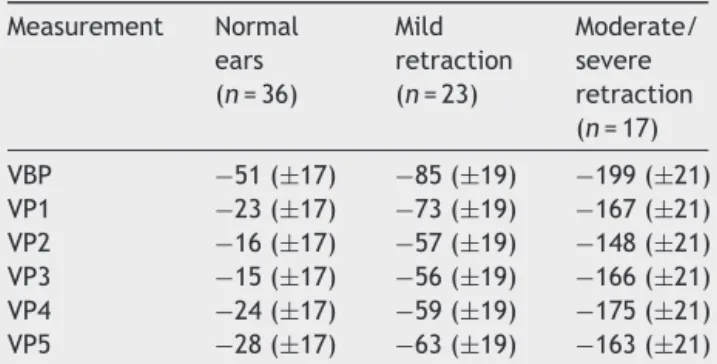
At the first time point of assessment with the Valsalva maneuver,therewasatrendtowardincreasingmiddleear pressuresfrombaseline(VBP)duringeach ofthefive con-secutiveValsalvamaneuvers(VP1---VP5)in allthreegroups ofears,withp=0.012(p [measurement]).Meanpressures (VP1---VP5)weredifferentin each group,withp<0.001(p [group]).Atthesecondtimepointofassessment,thetrend toward pressures increasing from VBP during each of the fiveconsecutivemaneuvers(VP1---VP5)remained;however, due to the behavior of pressure measurements in group 3, p-values did notreach statistical significance (p [mea-surement]=0.707).Again,meanpressures(VP1---VP5)were differentineachgroup,asatthefirsttimepointof assess-ment(p[group]<0.001).Tables1and2showtheestimated meanpressuresatbaselineandafterfiveconsecutive Val-salva maneuvers, after mixed-models adjustment, in the threestudygroups, at thefirstand secondtimepointsof assessment, respectively. At both time points, the peak increase in middle ear pressure occurred during the first threemaneuvers,inallthreestudygroups.Fig.1showsthe variabilityinmeanpressuresinthethreestudygroupsover
Table 1 Estimated means obtained with a linear mixed
modelfortheValsalvamaneuverinthethreegroups,atthe firsttimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
VBP −51(±17) −85(±19) −199(±21) VP1 −23(±17) −73(±19) −167(±21) VP2 −16(±17) −57(±19) −148(±21) VP3 −15(±17) −56(±19) −166(±21) VP4 −24(±17) −59(±19) −175(±21) VP5 −28 (±17) −63 (±19) −163 (±21)
VBP,Valsalvamaneuverbaselinepressure;VP,Valsalva maneu-verpressure.
Data expressed as mean (standard error), (p [measure-ment])=0.012;(p[group])<0.001.
Table 2 Estimated means obtained with a linear mixed
modelfortheValsalvamaneuverinthethreegroups,atthe secondtimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
VBP −53(±18) −84(±20) −154(±22) VP1 −42(±18) −89(±20) −136(±22) VP2 −37(±18) −67(±20) −156(±22) VP3 −36(±18) −68(±20) −148(±22) VP4 −37(±18) −70(±20) −168(±22) VP5 −36(±18) −73(±20) −185(±22)
VBP,Valsalvamaneuverbaselinepressure;VP,Valsalva maneu-verpressure.
Data expressed as mean (standard error); (p [measure-ment])=0.707;(p[group])<0.001.
thecourseofthetestmaneuverprocess(VBPandVP1---VP5), atthefirstandsecondtimepointsofassessment.
Snifftest
Atbothtimepointsofassessmentwiththesnifftest,there was no trend toward decreases in middle ear pressures frombaseline(SBP)duringeachofthefiveconsecutivetest maneuvers(SP1---SP5)inanyofthethreegroupsofears,as representedby thep-valuesobtainedat thefirstand sec-ond time points of assessment (p [measurement]=0.716,
First time point Second time point
0
–50
–100
–150
Mean pressure (daP
a)
–200
–250
PBV PV1 PV2 PV3 PV4 PV5 PBV PV1 PV2 PV3 PV4 PV5 0
–50
–100
–150
–200
–250
Normals ears (group 1) Mild retraction (group 2) Moderate/severe retraction (group 3)
Figure1 VariabilityofmeanmiddleearpressuremeasurementsduringValsalvamaneuveratthefirstandsecondtimepointsof assessment.
First time point Second time point
0
–50
–100
–150
Mean pressure (daP
a)
–200
–250
SBP SP1 SP2 SP3 SP4 SP5 SBP SP1 SP2 SP3 SP4 SP5 0
–50
–100
–150
–200
–250
Normal ears (group 1) Mild retraction (group 2) Moderate/severe retraction (group 3)
Figure2 Variability ofmeanmiddle earpressuremeasurements duringthesniff test atthefirst andsecondtime pointsof assessment.
Toynbeemaneuver
AtbothtimepointsofassessmentwiththeToynbee maneu-ver,therewerenotrendstowardeitherdecreaseorincrease inmiddleearpressuresfrombaseline(TBP)duringeachof the five consecutive test maneuvers (TP1---TP5) in any of the threegroups of ears, as represented by the p-values obtainedatthefirstandsecondtimepointsofassessment (p [measurement]=0.945 and 0.440, respectively). Mean pressures(TP1---TP5)weredifferent ineach groupat both timepoints(p<0.001).Tables 5and6showtheestimated meanpressures atbaselineandafterfiveconsecutivetest maneuvers after mixed-models adjustment, in the three studygroups,atthefirstandsecondtimepointsof assess-ment, respectively. Fig. 3 demonstrates the variability in meanpressuresinthethreestudygroupsoverthecourseof thetestmaneuver process(TBPandTP1---TP5),atthefirst andsecondtimepointsofassessment.
Toassessthedegreeofagreementbetweenthetwotime pointsofmiddleearpressuremeasurementduringthe per-formanceofETFtests,scatterchartswereplottedforeach testandintraclasscorrelationcoefficients(ICCs)were cal-culated.TheICCswere0.65fortheValsalvamaneuver,0.67 forthesnifftest,and0.63fortheToynbeemaneuver,which correspondtomoderateagreementbetweenthetwotime pointsof assessment across all threetests.Bland---Altman plots of agreement between middle ear pressures at the twotimepointsofassessmentshowedpoorreplicabilityof resultswithallthreetestmaneuvers.
First time point Second time point
0
–50
–100
–150
–200
–250
Mean pressure (daP
a)
TBP TP1 TP2 TP3 TP4 TP5 TBP TP1 TP2 TP3 TP4 TP5 0
–50
–100
–150
–200
–250
Normal ears (group 1) Mild retraction (group 2) Moderate/severe retraction (group 3)
Figure3 VariabilityofmeanmiddleearpressuremeasurementsduringtheToynbeemaneuveratthefirstandsecondtimepoints ofassessment.
Table 3 Estimated means obtained with a linear mixed
modelfor the snifftest inthethreestudy groups, atthe firsttimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
SBP −31(±15) −85(±16) −157(±18) SP1 −40(±15) −79(±16) −140(±18) SP2 −45(±15) −78(±16) −176(±18) SP3 −46(±15) −84(±16) −152(±18) SP4 −41(±15) −79(±16) −169(±18) SP5 −41(±15) −77(±16) −163(±18)
SBP,snifftestbaselinepressure;SP,snifftestpressure. Data expressed as mean (standard error); (p [measure-ment])=0.716;(p[group])<0.001.
Table 4 Estimated means obtained with a linear mixed
modelfor the snifftest inthethreestudy groups, atthe secondtimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
SBP −42(±17) −71(±19) −146(±21) SP1 −47(±17) −72(±19) −124(±21) SP2 −46(±17) −74(±19) −130(±21) SP3 −49(±17) −76(±19) −134(±21) SP4 −49(±17) −72(±19) −165(±21) SP5 −54(±17) −73(±19) −167(±21)
SBP,snifftestbaselinepressure;SP,snifftestpressure. Data expressed as mean (standard error); (p [measure-ment])=0.477;(p[group])<0.001.
Table 5 Estimated means obtained with a linear mixed
modelfortheToynbeemaneuverinthethreestudygroups, atthefirsttimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
TBP −50(±16) −44(±18) −152(±20) TP1 −47(±16) −51(±18) −138(±20) TP2 −46(±16) −56(±18) −143(±20) TP3 −44(±16) −58(±18) −143(±20) TP4 −49(±16) −47(±18) −124(±20) TP5 −43(±16) −52(±18) −141(±20)
TBP,Toynbeemaneuverbaselinepressure;TP,Toynbee maneu-verpressure.
Data expressed as mean (standard error); (p [measure-ment])=0.945;(p[group])<0.001.
Table 6 Estimated means obtained with a linear mixed
modelfortheToynbeemaneuverinthethreestudygroups, atthesecondtimepointofassessment.
Measurement Normal ears (n=36)
Mild retraction (n=23)
Moderate/ severe retraction (n=17)
TBP −54(±16) −67(±18) −148(±20) TP1 −50(±16) −78(±18) −137(±20) TP2 −45(±16) −76(±18) −144(±20) TP3 −40(±16) −75(±18) −125(±20) TP4 −40(±16) −74(±18) −110(±20) TP5 −42(±16) −84(±18) −118(±20)
TBP,Toynbeemaneuverbaselinepressure;TP,Toynbee maneu-verpressure.
600
400
200
0
–200
–400
Normal
Diff
erence betw
een measurement 1 and
measurement 2
Mild
Group
Moderate/Severe
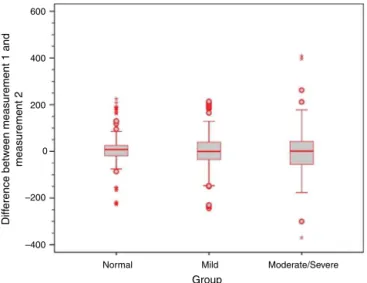
Figure4 Boxplotofdifferencesbetweentimepoints1and 2fortheValsalvamaneuverinthethreestudygroups.
600
400
200
0
–200
–400
Normal Mild
Group
Moderate/Severe
Diff
erence betw
een measurement 1 and
measurement 2
Figure5 Boxplotofdifferencesbetweentimepoints1and 2forthesnifftestinthethreestudygroups.
firstandsecondtimepointsofassessment weregreaterin themoderate/severe TM retractiongroup acrossall three ETFtests,asshownbytheboxplotsbelow(Figs.4---6).
Discussion
Eustachiantubefunctionhasbeenthesubjectofmany clin-icalandexperimental studies,most seekingtodefine the bestmethodsforitsassessment,aswellascharacterizeand improvethetreatmentofETdysfunctions.1,6,9---16
Neverthe-less,manyunansweredquestionsremain,suchas:whatis theclinicalutilityofETFtestsinpatientswithintactTMs, andwhichistheoptimaltestprotocol?Whichlevelofchange inmiddleearpressureafterperformanceofeachtestshould bedefinedasthecutoffforpositiveornegativeresults,and whatisthesignificanceofapositiveornegativefindingin dailyclinicalpractice?What istheutilityofthesetestsin patientswithpretestsuspicionofETdysfunction?
600
400
200
0
–200
–400
Normal Mild
Group
Moderate/Severe
Diff
erence betw
een measurement 1 and
measurement 2
Figure6 Boxplotofdifferencesbetweentimepoints1and 2fortheToynbeemaneuverinthethreestudygroups.
Thesedoubts remainbecause,althoughseveral studies have assessed tubal function in ears with intact TMs by meansofseveraltests,thereisnoconsensuson standardiza-tionoftesttechniques.Comparisonofresultsamongthese studies is therefore challenging, due to heterogeneity in testchoiceandadministration,aswellasmeasurementand reportingofresults.Hence,stricttestingandresult repor-tingprotocolsarerequired.
Thepresentstudydidnotconsiderwhethertestresults were positiveor negative,as elsewhere inthe literature, but rather if a statistically significant variation in mean pressuresoccurred.Thiscriterionwaschosenbecause,after anextensivereviewoftheliterature,itwasdeterminedthat noconsensusexists astowhich change inpressure would constituteapositiveresult.Somestudiesadvocatethatany increase in pressureafter the Valsalva maneuver be con-sideredpositive,11,15,17whereasothersadoptacutoffpoint
of 10daPa.1,9,18 Establishing which level of change should
be adopted to ensure clinical relevance is an extremely challenging proposition, as analysis of the difference in middle ear pressure that would lead to classification of a tympanogram asnormal or abnormal showed enormous variationinpressureranges(ofupto100daPa)and demon-stratedthatthesuggestedcutoffpointof10daPaispurely arbitrary.
questionablewhetherrepeatedmaneuvers,assuggestedby severalauthorsfortreatmentofETdysfunction,arereally capableofimprovingETF.14,16
Analysisofthesecondtimepointofassessmentshowed a persistent trend toward increased middle earpressures afterthe fiveconsecutivemaneuvers,although valuesdid notreachstatistical significance.Itisbelievedthatthisis attributabletothewidevariationinpressuresinthe mod-erate/severeTMretractiongroup.
Responsestothesnifftestweredistinctfromresponses totheValsalvamaneuver.Inboththefirstandthesecond timepointsofassessment,theexpecteddecreaseinmiddle earpressures failedtooccurinanyofthethreegroupsof ears.Althoughresponsevariabilitywasgreaterinearswith moderate/severeTMretractionthaninothergroups, admin-istration of the test maneuvers was not associated with significantchangesinmiddleearpressure.Similarresponses wereobservedtotheToynbeemaneuver,againbothinthe firstandinthesecondtimepointsofassessment:therewere nosignificantchangesinmiddleearpressuresfrombaseline afterthefiveconsecutivetestmaneuvers.
On comparison of mean pressures in each group of ears, it was found that these measurements were differ-entfromoneanotherduringallthreetests,aspatientswith moderate/severeretractionhadsignificantlymorenegative baseline pressures than the other patient groups. In the presentsample,patientswithmildTMretraction---despite near-normalresponsestotestmaneuvers,aswellasnormal tympanogramsinmostcases---alsohadmorenegative base-line pressuresthanpatients withhealthyears (allfindings statisticallysignificant).
Swartsetal.17 reportedthat81% ofpatientswereable
toinduceincreasesinmiddleearpressureafteraValsalva maneuver.Inasampleofhealthypatients,Falkfoundthat only 14% of the tested ears had negative pressure after the sniff test.19 A study of 32 patients found that only 5
(16%) exhibitedchanges in middle earpressure after this test.17 Ryding et al.20 found that patients with a history
of COM had significantly poorer active ETF as compared withhealthycontrols,andthatearwithevidenceoftubal dysfunctionorpatuloustubeshadthemostsevereTM dys-function. The present study corroborates the findings of theseauthors,demonstrating thatthe earswiththemost severeTMchangesexhibitedtheleastresponsetoValsalva maneuvers. Bunneet al.9 also found the Valsalva
maneu-ver to be more effective in healthy ears than after OM. Another study conducted by the same authors showed a 90%successrateformiddleearpressureequalizationwith thismaneuverinhealthysubjects,vs.only48%inpatients withTM retraction.11 In thesame study,26% ofears with
TMretractionand44% ofhealthyearshad apositivesniff test.Interestingly,inthatstudy,retractionswerenot clas-sifiedbyseverity,and,asinthepresentinvestigation,each degreeofretractionwasassociatedwithadistinctpattern ofresponsetotubalpatencytests.Earswithmildretraction respondedinamannermuchclosertohealthyearsthanears withmarkedTMretraction.
ItiswellknownthattheresultsofETFtestsmaydepend on howthe test is performed (e.g., how forcefully air is insufflated,andwhetherthepatientswallowsimmediately after the maneuver). Although these variations mayhave occurredinthepresentstudy,particularlyduetothelack
ofanyincreaseinmeanpressuresinthemoderate/severe retractiongroupaftertheValsalvamaneuverattimepoint 2,thefindingsareconsistentwiththosereportedinthe lit-erature,whichsuggeststhattheValsalvamaneuverismore effective than other tests.11 Anotherpotential reason for
thelackofanysignificantincreaseinpressureafterthe Val-salvamaneuver in earswithmoresevere TM retractionis thatthesepatientsexperienceworseeardiscomfortduring themaneuver,whichmayleadtoless forcefulinsufflation and,therefore,lessenedeffectivenessoftheValsalvatest ascomparedtootherpatients.
Inaddition,onlyweaktomoderateagreementwasfound betweenmeasurementsobtainedatthefirstandatthe sec-ondtimepointsof assessmentwithallthreetests.This is consistent with the existing literature, and demonstrates substantialintra-individualvariability.9Furthermore,using
allthreetests,therangeofdifferencebetween measure-ments obtained at the first and second time points was greaterinearswithmoderate/severeTMretraction,which showsthatthebehavioroftheseearsinresponsetoETFtests isevenmoreunstable.Thisvariabilityisconsistentwiththe clinicalinstabilityoftenseeninpatientswithTMretraction andatelectasis.16,21
In view of the broad variability in ETF tests, a single assessmentoftubalopeningisoflimitedapplicability, par-ticularlyinpatientswithmiddleeardisease.ETopeningand closureare less variablein normalears than in ears with TMretraction.11,14,16,22Ifatestyieldsapositiveresult,ETF
isprobablygood,but anegativeresultcannotbe usedto drawdefinitive conclusionsabout saidfunction.According toBunneetal.,7,11testresultsinasubstantialproportionof
patientsshiftfrompositivetonegativeorviceversaon re-administrationoftheValsalvaandsnifftestsafter30min. FalkandMagnusonreportedsimilarfindingsregardingtest instability,withqualitativeresponsestothesnifftest chang-ingin30%ofpatientswhenretestedonthesameday.14
Therefore,ETFtests,whichwerewidelyemployedinthe past, are nowof questionable clinical applicability, since theirresultsaremostvariableandleastreliableprecisely inthepatientpopulationinwhomtheywouldbemost indi-cated(earswithTMretractionandatelectasis).
Conclusion
In the study population, mean pressures in the tympanic cavity tended to increase from baseline during the Val-salvamaneuver,inallthreestudy groups,onlyatthefirst timepoint of assessment. The expected changes in pres-sure during the sniff test and Toynbee maneuver did not occurinanyofthethreestudygroupsateithertimepoint ofassessment.The normalearandmild retractiongroups behavedsimilarlybetweenoneanotheracrossalltests.The maneuversstudiedhereinexhibitedweaktomoderate intra-individualvariation, demonstratingpoor test replicability. Greatervariationbetweenmeasurementsoccurred among earswithmoderate/severeTMretraction.
Conflicts
of
interest
References
1.HidirY,UlusS,KarahatayS,SatarB.Acomparativestudyon effi-ciencyofmiddleearpressureequalizationtechniquesinhealthy volunteers.AurisNasusLarynx.2011;38:450---5.
2.DoyleWJ,SerokyJT,AlperCM.Gasexchangeacrossthe mid-dleearmucosainmonkeys.Estimationofexchangerate.Arch OtolaryngolHeadNeckSurg.1995;121:887---92.
3.BluestoneCD.Pathogenesisofotitismedia:roleofeustachian tube.PediatrInfectDisJ.1996;15:281---91.
4.Bluestone CD, Hebda PA, Alper CM, Sando I, Buchman CH, Stangerup SE, et al. Recent advances in otitis media. 2. Eustachiantube,middleear,andmastoidanatomy;physiology, pathophysiology, and pathogenesis.Ann OtolRhinol Laryngol Suppl.2005;194:16---30.
5.BentoRF,MartinsGSQ,PinnaMH.Tratadodeotologia.2nded. EditoraAteneu;2013.
6.BluestoneCD,SwartsJD.Humanevolutionaryhistory: conse-quencesforthepathogenesisofotitismedia.OtolaryngolHead NeckSurg.2010;143:739---44.
7.BunneM,MagnusonB,FalkB,HellstromS.Eustachiantube func-tionvariesovertimeinchildrenwithsecretoryotitismedia. ActaOtolaryngol.2000;120:716---23.
8.SadeJ.Thenasopharynx,eustachiantubeandotitismedia.J LaryngolOtol.1994;108:95---100.
9.Bunne M, Falk B, Hellstrom S, Magnuson B. Variability of Eustachiantubefunctioninchildrenwithsecretoryotitismedia. Evaluationsat tube insertionand at follow-up. IntJPediatr Otorhinolaryngol.2000;52:131---41.
10.Recentadvancesinotitismedia.AnnOtolRhinolLaryngolSuppl. 2005;194:6---160.
11.Bunne M, Falk B, Magnuson B, Hellstrom S. Variability of Eustachian tube function: comparison of ears with retrac-tiondiseaseandnormalmiddleears.Laryngoscope.2000;110: 1389---95.
12.Choi SH, Han JH, Chung JW. Pre-operative evaluation of Eustachiantubefunctionusinga modifiedpressure equilibra-tiontestispredictiveofgoodpostoperativehearingandmiddle earaerationintype1tympanoplastypatients.ClinExp Otorhi-nolaryngol.2009;2:61---5.
13.DoyleWJ,WintherB,AlperC.Dailytympanometryasa func-tional measure of middle ear status and Eustachian tube function.AurisNasusLarynx.2009;36:20---5.
14.FalkB,MagnusonB.Test-retestvariabilityofEustachiantube responsesinchildrenwithpersistentmiddleeareffusion.Arch OtolaryngolHeadNeckSurg.1984;240:145---52.
15.MakibaraRR,Fukunaga JY,GilD.Eustachian tubefunctionin adultswithintacttympanicmembrane.BrazJ Otorhinolaryn-gol.2010;76:340---6.
16.SandoI,TakahashiH,MatsuneS,AokiH.Localizationoffunction intheEustachiantube:ahypothesis.AnnOtolRhinolLaryngol. 1994;103:311---4.
17.Swarts JD, Alper CM, Mandel EM, Villardo R, Doyle WJ. Eustachiantubefunctioninadultswithoutmiddleeardisease. AnnOtolRhinolLaryngol.2011;120:220---5.
18.CinamonU.PassiveanddynamicpropertiesoftheEustachian tube: quantitative studies in a model. Otol Neurotol. 2004;25:1031---3.
19.FalkB.Negativemiddleearpressureinducedbysniffing:a tym-panometricstudyinpersonswithhealthyears.JOtolaryngol. 1981;10:299---305.
20.RydingM,WhiteP,KalmO.Eustachiantubefunctionand tym-panicmembranefindingsafterchronicsecretoryotitismedia. IntJPediatrOtorhinolaryngol.2004;68:197---204.
21.SadeJ,BercoE.Atelectasisandsecretoryotitismedia.AnnOtol RhinolLaryngol.1976;85:66---72.
22.Adali MK, Uzun C. Comparison of effects of dry versus