www.jped.com.br
ORIGINAL
ARTICLE
Effect
of
4
′
galactooligosaccharide
on
constipation
symptoms
夽
,
夽夽
,
夽夽夽
Célia
A.V.
Beleli
a,
Maria
A.R.G.M.
Antonio
a,
Rosângela
dos
Santos
b,
Gláucia
M.
Pastore
b,
Elizete
A.
Lomazi
a,∗aSchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil bFacultyofFoodEngineering,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received29September2014;accepted23January2015 Availableonline30July2015
KEYWORDS
Child; Constipation; Functionalfood; Therapy
Abstract
Objective: Fructooligosacharides andgalactooligosacharides softenfecal bolusandincrease frequency ofdepositions whenaddedtoinfantformula.This studyaimedtodeterminethe effectsofgalactooligosaccharideinpediatricpatientswithchronicconstipation.
Methods: From 2010 to 2012, 20 constipated patients (4---16 years of age) attended to at a primary healthcare unit were enrolled in adouble-blinded, placebo-controlledcrossover trial.Elevenchildren ingested galactooligosaccharide(1.7g)for 30 days,followed bya 15-day washoutperiod, anda30-dayperiod ofplacebo(maltodextrin).Ninepatientsingested maltodextrin for 30 days, followed by 15-day washout period, and galactooligosaccharide (1.7g)for30days.Constipationsymptomswereconsideredasprimaryoutcomes:bowel move-ments/week, straining during defecation, and stool consistency. Outcome symptoms were rankedaccordingtoanumericalscaleelaboratedforthisstudy.Datawererecordedat base-line,andondays15and30ofeach30-daycrossoverperiod.Repeated-measuresanalysisof variance(ANOVA)wasusedtoanalyzesymptomsalongtime.
Results: Atbaseline,therewasnosignificantdifferenceinsymptomsseveritybetweengroups (p=0.45).Galactooligosaccharideingestion wasrelated toincreaseofthebowelmovement frequency, p<0.0001; relief ofdefecation straining, p<0.0001;and decrease instool con-sistency, p=0.0014, comparedto placeboingestion. Patientsreportedno sideeffectsfrom galactooligosaccharide.
夽 Pleasecitethisarticleas:BeleliCA,AntonioMA,dosSantosR,PastoreGM,LomaziEA.Effectof4′galactooligosaccharideonconstipation
symptoms.JPediatr(RioJ).2015;91;567---73.
夽夽StudylinkedtoSchoolofMedicalSciencesandFacultyofFoodEngineering,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,
SP,Brasil.
夽夽夽
StudyconductedatBasicHealthUnitintheoutskirtsofCampinas,coordinatedbya teamofpediatriciansoftheDepartmentof Pediatrics,SchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brasil.
∗Correspondingauthor.
E-mail:[email protected](E.A.Lomazi). http://dx.doi.org/10.1016/j.jped.2015.01.010
Conclusion: Galactooligosaccharidewaseffectiveatimprovingclinicalsymptomsinthisgroup ofconstipatedchildren.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Crianc¸a; Constipac¸ão intestinal;
Alimentofuncional; Tratamento
Efeitodogalactooligosacarídeosobreossintomasdeconstipac¸ão
Resumo
Objetivo: Aadic¸ãodefrutooligosacarídeosegalactooligosacarídeosafórmulasinfantispode diminuiraconsistênciafecaleaumentarafrequênciadasevacuac¸ões.Oobjetivodopresente estudofoideterminaroefeitodogalactooligosacarídeoemcrianc¸ascomconstipac¸ãocrônica. Métodos: Entre2010e2012,20 pacientesconstipados(4-16anos),atendidosnumaunidade básica de saúde, completaram ensaioclínico duplo cego,placebo-controlado e de delinea-mentocrossover.Onzepacientesreceberamgalactooligosacarídeo(1,7g)por30dias,seguidos por15diasdewashout,e,após,placebo(maltodextrina)por30dias;outrosnovepacientes receberamplacebo30dias,seguidosde15diasdewashoute30diasdegalactooligosacarídeo (1,7g).Osdesfechosprimáriosforamfrequênciasemanaldeevacuac¸ões,esforc¸oevacuatórioe consistênciafecal,classificadaporescalanuméricaelaboradaparaesseestudoecompiladano primeiro,150e300diasdecadaperíododecrossover.Análiseestatísticafoifeitapormétodo
deanálisedevariância(ANOVA)paramedidasrepetidas.
Resultados: Intensidadedossintomasnosgruposfoisemelhantenoiníciodoestudo(p=0,45). Durante aingestão degalactooligosacarídeo constatou-se maiorfrequência deevacuac¸ões, p<0,0001, menor dificuldade evacuatória, p<0,0001 e diminuic¸ão da consistência fecal, p=0,0014.Efeitoscolateraisnãoforamreferidosduranteaingestãodoprebiótico.
Conclusão: Duranteaingestãodegalactooligosacarídeoossintomasclínicosdaconstipac¸ãoem crianc¸aseadolescentesforamsignificantementealiviados.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Datafromthe lastdecadeshave indicatedchildhood con-stipation as a common problem worldwide. Its reported prevalence has varied from 0.7% to 30%; in addition, in recentyears,thenumberofpatientshasgrownsignificantly inwesternworld.1,2Differenttherapeuticshave been rec-ommended for constipation management, including stool lubricants,dietaryfibersupplementation,laxatives, proki-netics,andfunctionalfoods.Osmoticlaxativesanddietary fibersarethemostwidelyusedtherapeutictools;however, thereareveryfew evidence-basedstudiestosupportany treatment recommendations for constipation in pediatric patients.3,4
Functional foods containing probiotics or prebiotics havebeen identifiedasuseful for regulatingbowel habits in children.5 A multicenter controlled trial showed that consumption of fermented dairy products containing Bifi-dobacterium lactis was associated to increase in stool frequencyinchildrenwithconstipationandstoolfrequency <3times/week.6
Concerningtheeffectsofprebioticsonlaxation,studies conducted in pediatric patients have included predomi-nantlyinfants fedexclusively on milk formulas. Ingestion of prebiotics was proposed to be effective for treating constipation, since consumption of fructooligosaccharides and galactooligosaccharides added to infant formula has
been shown toincrease fecal bolus andthe frequency of depositions.7---10
Therationaleofprebiotics’therapeutic effectson con-stipationisbasedonthefactthat4′galactooligosaccharide
(GOS) affects the host health by stimulating the growth and/or activity of colonic bifidobacteria.11 Bifidobacte-ria, mainly Lactobacillus acidophillus or Bifidobacterium bifidum,actbyfermentingcarbohydrates,producingshort chainfattyacids(SCFAs),themajoraniononthelarge intes-tine; SCFAs are able to increase colonic blood flow and muscularactivity,enhancingfecalwetweightandthus pro-motinglaxation.12,13
Thecurrentstudywasaimedatevaluatingthe effective-nessoftheprebioticGOSinthetreatmentofconstipation inchildrenandadolescents.
Methods
Design:Aninterventional,non-randomized,double-blinded, placebo-controlled, crossover assignment study was con-ductedfromJune8,2010toMarch25,2012.
Setting:Aprimaryhealthcareunitmanagedbymedical schoolstaff.
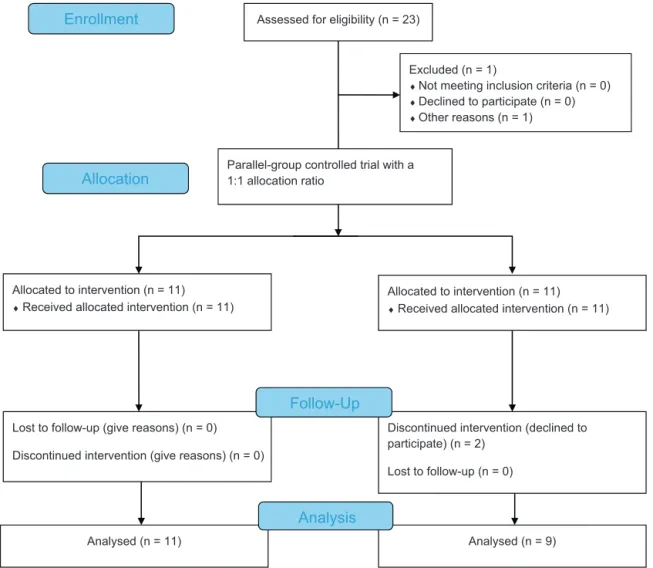
Assessed for eligibility (n = 23)
Excluded (n = 1)
♦Not meeting inclusion criteria (n = 0) ♦Declined to participate (n = 0) ♦Other reasons (n = 1)
Analysed (n = 11) Lost to follow-up (give reasons) (n = 0)
Discontinued intervention (give reasons) (n = 0) Allocated to intervention (n = 11)
♦Received allocated intervention (n = 11)
Discontinued intervention (declined to participate) (n = 2)
Lost to follow-up (n = 0) Allocated to intervention (n = 11)
♦Received allocated intervention (n = 11)
Analysed (n = 9)
Analysis
Follow-Up
Enrollment
Parallel-group controlled trial with a 1:1 allocation ratio
Allocation
Figure1 StudyflowchartaccordingtotheConsolidatedStandardsofReportingTrialsstatement.30
Eligibilitycriteria
Inclusioncriterion: Diagnosisof constipationbased onthe RomeIIIcriteriaforfunctionaldisorders.14Furthermore,in ordertoexcludelactoseintolerance,tobeenrolledpatients wererequiredtoreportadailyingestionofatleast250mLof cow’smilkwithoutreferringsymptoms,andtheywereasked specifically about pain, cramping, diarrhea,or flatulence aftermilkingestion.
Non-inclusion criterion: Patients with other comorbid conditions,thosealreadyundertreatmentforconstipation, andthosewhousedantibioticsor probioticsfor thelast6 months.
Studyproducts
Testproduct:TheprebioticGOSwasproducedfromlactose throughtheactionof-galactosidaseenzymes,producedby themicroorganismScopulariopsissp.15Adaily6mLvolume ofprescribedmaltodextrinsolution(placebo)andGOSwas ingestedinthe morning.IntheGOSmixture,a volumeof 6mLcontaining1.7gGOSwasused.Parents/guardiansand participants wereinformedof possibleGOS ingestion side effects,suchasabdominaldistention,flatulence,abdominal cramping,anddiarrhea.
Control: The placebo consistedof a maltodextrin solu-tion.
Blinding
Thetwotreatments,prebioticGOSandplacebo,were iden-tical in viscidity, color, smell, taste, and packaging. All researchstaffandpatients involved were unawareof the treatmentadministeredtothepatient.
Orderofpatientsinclusioninstudyandflow diagram
The trial consisted of a two-sequence, two-period, two-treatment crossover design. Each crossover period lasted 30days,separatedby15daysasthewashoutperiod.The sequenceof GOSor placeboingestion definedby thefirst patientenrolledinthestudywaschosenbylot.Theorderof ingestioninthefollowedpatientswassystematically alter-nate.Fig.1showsastudyflowchart.16
Compliancewithsubstanceswasmeasuredbythereturnof previouslyusedflasks.
Samplesizecalculation
Datafrom10subjectswhofirstcompletedthestudywere analyzed by ANOVA to calculate sample size.17 SAS soft-ware for sample size calculation was used, v. 9.2 of the SASSystemforWindows(SASInstituteInc.Cary,NC,USA). Statistical analysis using analysis of variance (ANOVA) for repeatedmeasureswasapplied.ANOVAwasusedtoanalyze comparativetreatments,consideringthedifferencein out-comes.PoweranalysiswasappliedinthecontextofANOVA by assuming a two-sequence, two-period, two-treatment crossoverdesign,effectsizeinthepopulation,samplesize, and significance level. A statistically significant effect in ANOVAwasmonitoredwithfollow-uptests,inordertoassess which variable was different between groups. Follow-up tests were performed post hoc. SAS software ‘‘fpower’’ wasthenusedtocalculatesamplesizeafterspecifyingthe powerofstudyat90%andalpha=0.05.Suchanalysisshowed thatusingapoweranalysisof90%,ninesubjectswouldbe requiredineachgroup.
Further dietaryfiber supplementationwas notallowed untilcompletionofthetrial.Forthosepatientswhorefused toparticipateinthestudyorthosewhocompletedthetrial, dietaryfiberwasprescribed.
Outcomes
Three symptoms were considered as primary outcomes: bowelmovementsperweek, fecalconsistency and strain-ing/painduringfecalpassage.Thesesymptomswereranked accordingtonumericalvalues.Bowelmovementsfrequency wasranked from1to3,asfollows:1=greaterthan three timesperweek;2=onetotwotimesperweek;and3=less thanonceperweek.Intensityofstraining/painduringstool passage ranged from 1 to 3 (1=no discomfort or pain, 2=episodic pain and/or discomfort, and 3=pain and/or discomfortduring every stool passage). Fecal consistency wasdefined according to a photographic scale18 and var-iedfrom3to0(3=hard,separate lumps,2=banana with deepcracks,1=bananawithsuperficialcracks,and0=soft banana/separatesoftpieces/fluffypieces).Thesumof val-uesrangedfrom2to9andwasconsideredaclinicalscore characterizingsymptom intensity. The physical evaluation andpatientscoreswerecompiledduringthebaseline inter-view,andonday15and30ineachperiod.
Statisticalanalysis
Descriptive analyses were performed, including measures ofcentraltendencyanddispersionfornumericalvariables. Atbaseline,clinicalanddemographicdatawerecompared (Mann---Whitneytest).
GOSeffectwasdeterminedaccording toatwo-period, two-treatmentcrossoverassignment:GOSandplacebo.The Kolmogorov---Smirnovtest wasperformed totestnormality ofdata,rejectingthenullhypothesisofnormality.For statis-ticalanalysis,ANOVAwasusedforrepeatedmeasurements
withrank-transformation(ANOVAonranks).Rankingisa pro-cedureusedtotransformdatathatviolatetheassumptions ofnormality.ANOVAonrankssignifiesthatastandard anal-ysis of variance has been calculated on rank-transformed data.Thesignificanceleveladoptedforstatisticaltestswas 5%.
The study was approved by the Ethics Committee of theinstitution,No.366/2009,CAAE:0280.0.146.000-09.All participants and/or parents/guardianssigned an informed consent.Thestudywasreviewedandpublishedonthesite ClinicalTrials.gov,identifiernumber:NCT02183766.
Results
Twenty-three patients were initially included, but three patientswerelosttofollow-upduetoachange ofaddress without anypreviouscommunication.Twentychildrenand adolescents aged 4---16 years (mean 8.8±4.1 SD) were included. Twelve children were female. After unblinding, itwasobservedthat11patientsreceivedthesequence of GOS to placebo and nine patients received the sequence ofplacebotoGOS.Noneofthepatientsrefusedtreatment or had a low acceptance of medication. At the baseline interview, all patients reported fewer than three bowel movementsperweekorhardstoolconsistency.
Sincepatients were systematically allocated togroups according toconsecutive firsthealthcare visit,theeffect of allocation (order of product ingestion) was calculated byANOVAforrepeatedmeasures;therewasnodifference betweenthegroups’scoresdeterminedbygroupallocation,
p=0.9427.
Clinicalscoresovertime
Table 1shows demographicclinical data from20 patients
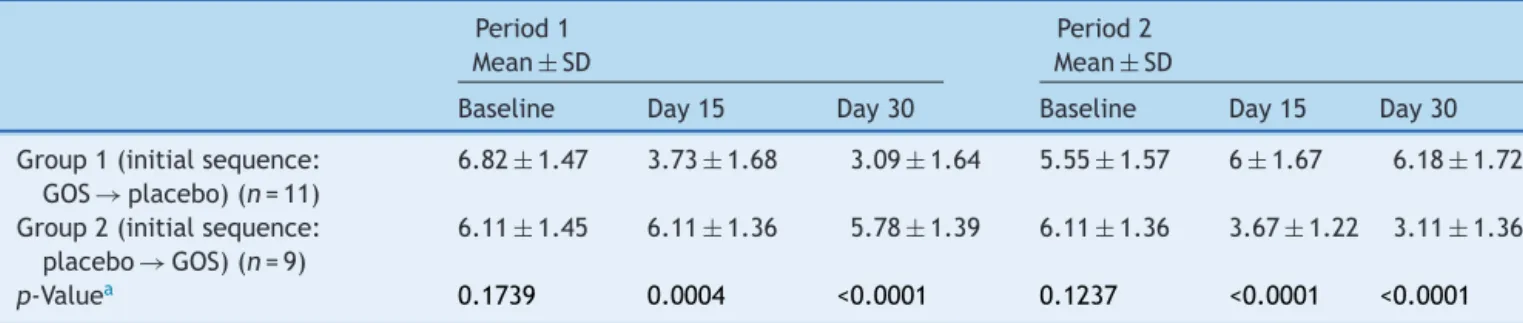
whocompletedthetrial.Tables2and3showthedistribution ofclinical scores,consideringGOSeffectandtimeeffect, respectively, i.e., clinical scores over time.Mean clinical scoresdecreasedsignificantlyduringGOSingestioninboth groups(Table2).Meanclinicalscoresovertimeshowedthat theeffectofGOSlastedthroughoutitsingestion,sincethe washout periodstopped theeffect of GOS.There wasno group/timeinteraction(Table3).
Discussion
The prebiotic GOS ingested by constipated children was effectiveatincreasingbowelmovementfrequency, reliev-ingpainor discomfortduringstoolpassage,andsoftening stoolconsistency.Noadverseeffectswerereported.
Table1 Baselinedemographicsandclinicalcharacteristics.
GOS→PlaceboGroup1(n=11) Placebo→GOSGroup2(n=9) p-Valuea
Variable
Sex,M:F 4:7 4:5 NS
Age,(years)(mean±SD) 8.7±4.8 8.8±3.5 NS Ageatearlysymptoms,(years,mean±SD) 5±4.7 3.8±2.4 NS Constipationstartedon1styearoflife 3/11 1/9 NS Durationofconstipation(years) 3.8±0.7 5.4±3.45 NS Bowelmovements/week(Baseline) 1.5±0.5 1.7±0.7 NS
Stoolconsistencyb
Mean±SD 2.8±0.2 2.6±0.2 0.07
Median(min-max) 3(1---2) 2.5(2.5---3)
Baselinescorec 6.5±1 6.1±1.4 0.45
ScoreduringGOS 4.6±1.2 4.3±1 0.70
Scoreduringplacebo 5.8±1.1 6±1.3 0.65
Clinicalscoreispresentedasmean±SD. GOS,galactooligosaccharide.
a Mann---Whitneytest.
b Stoolconsistencyclassification:3=hard;2=bananawithdeepcracks;1=bananawithsuperficialcracks,zero=softbanana/separate
softpieces/fluffypieces.
c Clinicalscoreincludedbowelfrequency,fecalconsistency,anddefecationdiscomfort,andrangedfrom9(greatestseverity)to2(no
symptoms).
Table2 Clinicalscoresbasedonbowelfrequency,fecalconsistency,anddefecationdiscomfort.
Period1 Mean±SD
Period2 Mean±SD
Baseline Day15 Day30 Baseline Day15 Day30
Group1(initialsequence: GOS→placebo)(n=11)
6.82±1.47 3.73±1.68 3.09±1.64 5.55±1.57 6±1.67 6.18±1.72
Group2(initialsequence: placebo→GOS)(n=9)
6.11±1.45 6.11±1.36 5.78±1.39 6.11±1.36 3.67±1.22 3.11±1.36
p-Valuea 0.1739 0.0004 <0.0001 0.1237 <0.0001 <0.0001
GOS,galactooligosaccharide.
a ANOVA.
Table3 Clinicaldataandtimeeffect(clinicaldataovertime)usinganalysisofvariance(ANOVA).
Score/group Period1 Mean±SD
p-Value Time effect
Period2 Mean±SD
p-Value Time effect
Baseline Day15 Day30 Baseline Day15 Day30
Group1
GOS→Placebo (n=11)
6.82±1.47 3.73±1.68 3.09±1.64 <0.0001a 5.55±1.57 6±1.67 6±1.72 <0.0001b
Group2
Placebo→GOS (n=9)
6.11±1.45 6.11±1.36 5.78±1.39 0.4493 6.11±1.36 3.67±1.22 3.11±1.36 0.0105b
Clinicalscorerangedfrom9(greatestseverity)to2(nosymptoms). GOS,galactooligosaccharide.
a p-Valuereferstoclinicalscorevaluesatbaselinetimevs.day15oftrial.
b p-Valuereferstoclinicalscorevaluesatbaselinetimevs.day15andatbaselinetimevs.day30oftrial.
The main symptoms of constipated children seek-ing Brazilian primary health care settings refer to hard stools and large intervals between bowel movements. Less than 15% of patients reported fecal retentive
complaintsduring itsingestion, regardless other adjuvant recommendation.
Inpresentstudy,meandurationwasfrom3to5years.It islikelythatmostpatientshadalreadybeentreatedbutdid notcontinuewiththerapy.Nopatientreferredsymptomsof retentivefecalincontinenceorhadfecalretentionpalpable inabdomenoridentifiedbyrectalexamination.Itappears thatthepatientshavemildconstipation,responsivetooral laxativesandwithnocomplications.Suchaclinicalpicture isfound commonly in constipatedchildren treated in pri-maryhealthcarecenters.Thesedatashowthatasagroup, childrenandadolescentsimprovewhileusingGOS,andno changesinsymptomwererecordedwithplacebo.Noother sortoftherapywasrecommendedbesidesstrictadherence totheproducts.
Inspiteofapaucityofdataprovidingconclusiveevidence tosupportthecurrentrecommendationsoffiberintakefor constipatedpediatricpatients,pediatricclinicaltrialshave shownthatdietaryfiberincreasesthefrequencyof defeca-tionandstoolsoftness.23Dietmodificationtoincreasefiber consumptionisconsidered animportantcomponentinthe managementofconstipation.Dietaryfibersupplementation wasnotprescribedduringthistrial,inordertobetter evalu-atetheisolatedGOSeffectonfecalcharacteristics.Dietary fiberwasprescribedtosubjectswhodeclinedtoparticipate inthestudyortothosewhohadcompletedthetrial.
Broad age range and sample size should be discussed as limitations of the present study. The pathogenesis of non-organicconstipation is closely relatedtostool toilet-ingrefusal caused bypainduring stool passage,generally occurring during the toilet-training period. Such patients usuallyhaveaprevioushistoryofhardfeces,andinfrequent and painful evacuation often accompanied by screaming and stool-holding maneuvers. When symptoms are not addressed, the condition progresses until a diagnosis is made.Inaround50%ofchildren,along-termoutcomecan be observed, and 25% of children with functional consti-pationcontinuetoexperiencesymptomsintoadulthood.24 Long-termconstipationis associatedwithfecalimpaction, retentive incontinence, and megarectum. Irrespective of complicationsandage,goodclinicaloutcomesweredefined asatleastthreebowelmovementsperweekforatleast4 weeks,withnomorethantwoepisodesoffecalincontinence permonth,irrespectiveoflaxativeuse.24Considering patho-genesis context, it must be pointed out that despite age variability,theincludedsubjectswereverysimilarintheir constipation characteristics, with no subjects presenting signsofcomplicationssuchasfecalimpactionand require-mentofaggressivelaxatives.Inrespecttothesmallsample issue,thecrossoverdesignwaschosenbecausethisdesign enabled researchers to make comparisons between small samples;thesamplesizewasprimarilydefinedassufficient bystatisticalanalysis.Acceptingtheseconsiderations,itis possibleto concludethat the present results aretrue for patientswithmildsymptoms.
In studies conducted to evaluate prebiotic effects on infantconstipation,treatmentdurationrangedfrom21days to8weeks for symptom evaluation.A 4-week periodwas proposedbasedonsuchstudies.25---27
The fixed GOS dosage was chosen to provide an ade-quatebalance between efficacy and tolerance, according toresultsfromadulttrials.Itwasnotpossibletoexamine
bifidogenic effectonmicrobiota or the increased produc-tionoffecalSCFAs.Accordingtotheliterature,theaddition of 12g/day of GOS was shown to be effective and well-tolerated, resulting in increased fecal bifidobacteria in healthy individuals.28,29 It was shown that the estimated safeadultdoserangingfrom0.3to0.4g/kg/dayand2.5g GOSissufficienttoinduceabifidogeniceffect.30An exces-siveamountofGOScouldpromoteadverseosmoticeffects leadingtoosmoticdiarrhea,symptomsnotreferredbythe presentpatientsduringGOSingestion.
ThispilotstudyshowedthatGOSimprovesclinical consti-pationsymptomsandmayrepresentasupportivemeasure inthetreatmentofconstipation.Toconfirmthesefindings, alarger,randomized,placebo-controlledtrialisrequired.
Funding
Tocarryouttheproject,fundingwasobtainedfromFAEPEX (Support Education Fund, the Research and Extension), SchoolofMedicalSciences,UniversidadeEstadualde Cam-pinas(UNICAMP),SaoPaulo,Brazilreleasedon12/11/2009 undertheAgreementN◦:519,294.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.VandenBergMM,BenningaMA,DiLorenzoC.Epidemiologyof childhoodconstipation: asystematic review.AmJ Gastroen-terol.2006;101:2401---9.
2.EverhartJE,RuhlCE.BurdenofdigestivediseasesintheUnited States: PartII. Lowergastrointestinal diseases. Gastroenter-ology.2009;136:741---54.
3.Gordon M, Naidoo K, Akobeng AK, Thomas AG. Cochrane review:osmoticandstimulant laxativesfor themanagement ofchildhoodconstipation(Review).Evid BasedChild Health. 2013;8:57---109.
4.PijpersMA, Tabbers MM, BenningaMA, Berger MY. Currently recommended treatments of childhood constipation are not evidencebased:asystematicliteraturereviewontheeffect oflaxative treatmentand dietary measures. Arch DisChild. 2009;94:117---31.
5.VandenplasY,Veereman-WautersG,DeGreefE,PeetersS, Cas-teelsA,MahlerT,etal.Probioticsandprebioticsinprevention andtreatmentofdiseasesininfantsandchildren.JPediatr(Rio J).2011;87:292---300.
6.TabbersMM,ChmielewskaA,RoseboomMG,BoudetC,PerrinC, SzajewskaH,etal.Effectoftheconsumptionofafermented dairyproductcontainingBifidobacteriumlactisDN-173010on constipationinchildhood:amulticentrerandomisedcontrolled trial(NTRTC:1571).BMCPediatr.2009;9:22.
7.NóbregaFJ,TrabulsiLR,KellerR,FranzolinMR,AlvesRC,Santos MF,etal.Effectsoftheprebiotic(oligosaccharide)inmodified milkpowderontheintestinalflora:comparisonwithmodified milkpowderwithoutprebioticinadouble-blindstudy.RevPaul Pediatr.2004;22:205---11.
9.CostalosC,KapikiA,ApostolouM,PapathomaE.Theeffectof aprebioticsupplementedformulaongrowthandstool microbi-ologyofterminfants.EarlyHumDev.2008;84:45---9.
10.RibeiroTC, Costa-RibeiroHJr,Almeida PS,PontesMV,Leite ME, Filadelfo LR, et al. Stool pattern changes in toddlers consuming a follow-on formula supplemented with polydex-troseandgalactooligosaccharides.JPediatrGastroenterolNutr. 2012;54:288---90.
11.Sabater-MolinaM,LarquéE,TorrellaF,ZamoraS.Dietary fruc-tooligosaccharidesandpotentialbenefitsonhealth.JPhysiol Biochem.2009;65:315---28.
12.TimmDA,ThomasW,BoileauTW,Williamson-HughesPS,Slavin JL.Polydextroseandsolublecornfiberincreasefive-dayfecal wetweightinhealthymenandwomen.JNutr.2013;143:473---8. 13.Topping DL, Clifton PM. Short-chain fatty acids and human colonic function: roles of resistant starch and nonstarch polysaccharides.PhysiolRev.2001;81:1031---64.
14.RasquinA,DiLorenzoC,ForbesD,GuiraldesE,HyamsJS, Sta-ianoA,etal.Childhoodfunctionalgastrointestinal disorders: child/adolescent.Gastroenterology.2006;130:1527---37. 15.Mwenya B, Santoso B, Sar C, Gamo Y, Kobayashi T, Arai I,
etal.Effectsofincludingbeta1,4-galactooligosaccharides, lac-ticacidbacteriaoryeastscultureonmethanogenesisaswell asenergy and nitrogenmetabolism in sheep. AnimFeed Sci Technol.2004;115:313---26.
16.Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updatedguidelinesforreportingparallelgrouprandomised tri-als.JPharmacolPharmacother.2010;1:100---7.
17.KhattreeR,NaikDN.Analysisofrepeatedmeasuresdata.In: KhattreeR, Naik DM, editors.Applied multivariate statistics withSASsoftware.2nd ed.Cary,NC:SASInstitute;2003. p. 151---246.
18.Rubin G, Dale A. Chronic constipation in children. BMJ. 2006;333:1051---5.
19.TeuriU,KorpelaR.Galacto-oligosaccharidesrelieve constipa-tioninelderlypeople.AnnNutrMetab.1998;42:319---27. 20.Moro G, Minoli I, Mosca M, Fanaro S, Jelinek J, Stahl B,
et al. Dosage-related bifidogenic effects of galacto- and fructooligosaccharidesinformula-fed terminfants.JPediatr GastroenterolNutr.2002;34:291---5.
21.Del Ciampo IR, Galvão LC, Del Ciampo LA, Fernandes MI. Prevalência de constipac¸ão intestinal crônica em crianc¸as atendidas em unidade básica de saúde. J Pediatr (Rio J). 2002;78:497---502.
22.BurgersR,Bonanno E,MadarenaE,GrazianoF,Pensabene L, Gardner W, et al. The care of constipated children in pri-mary care in different countries. Acta Paediatr. 2012;101: 677---80.
23.Weber TK, Toporovski MS, Tahan S, Neufeld CB, de Morais MB. Dietary fiber mixture in pediatric patients with con-trolled chronic constipation. J Pediatr Gastroenterol Nutr. 2014;58:297---302.
24.BongersME,vanWijkMP,ReitsmaJB,BenningaMA.Long-term prognosisforchildhoodconstipation:clinicaloutcomesin adult-hood.Pediatrics.2010;126:e156---62.
25.Moro GE, Stahl B, Fanaro S, Jelinek J, Boehm G, Coppa GV. Dietaryprebiotic oligosaccharidesare detectable inthe faeces offormula-fed infants.Acta PaediatrSuppl.2005;94: 27---30.
26.Boehm G, Lidestri M, CasettaP, Jelinek J, Negretti F,Stahl B, et al. Supplementationofa bovine milk formulawithan oligosaccharidemixtureincreases countsoffaecal bifidobac-teria in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2002;86:F178---81.
27.Scholtens PA, Alliet P, Raes M, Alles MS, Kroes H, Boehm G, et al. Fecal secretory immunoglobulin A is increased in healthyinfantswhoreceiveaformulawithshort-chain galacto-oligosaccharidesandlong-chainfructo-oligosaccharides.JNutr. 2008;138:1141---7.
28.SairanenU,PiirainenL,NevalaR,KorpelaR.Yoghurt contain-ing galacto-oligosaccharides,prunesand linseedreducesthe severityofmildconstipationinelderlysubjects.EurJClinNutr. 2007;61:1423---8.
29.BouhnikY,AchourL,PaineauD,Riottot M,AttarA,BornetF. Four-weekshortchainfructo-oligosaccharidesingestionleads toincreasingfecalbifidobacteriaandcholesterolexcretionin healthyelderlyvolunteers.NutrJ.2007;6:42.