www.jped.com.br
ORIGINAL
ARTICLE
High-frequency
profile
in
adolescents
and
its
relationship
with
the
use
of
personal
stereo
devices
夽
,
夽夽
Renata
Almeida
Araújo
Silvestre
a,∗,
Ângela
Ribas
a,
Rogério
Hammerschmidt
b,
Adriana
Bender
Moreira
de
Lacerda
aaUniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil bUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
Received14May2015;accepted13July2015 Availableonline20January2016
KEYWORDS Audiometry; Adolescent; MP3player; Hearingloss; Primaryprevention
Abstract
Objective: Toanalyzeandcorrelatetheaudiometricfindingsofhighfrequencies(9---16kHz)in
adolescentswiththeirhearinghabitsandattitudes,inordertopreventnoise-inducedhearing
loss.
Method: This was a descriptive cross-sectional study, which included 125 adolescents ina
sampleofnormal-hearingstudents,atastateschool.Thesubjectsperformedhigh-frequency
audiometrytestingandansweredaself-administeredquestionnaireaddressinginformationon
soundhabitsconcerningtheuseofpersonalstereodevices.Thesamplewasdividedaccording
totheexposurecharacteristics(time,duration,intensity,etc.)andtheresultswerecompared
withtheobservedthresholds,throughthedifferenceinproportionstest,chi-squared,Student’s
t-test,andANOVA,allatasignificancelevelof0.05.
Results: Averagehigh-frequencythresholdswereregisteredbelow15dBHLandnosignificant
correlationwasfoundbetweenhighfrequencyaudiometricfindingsandthedegreeofexposure.
Conclusion: Theprevalenceofharmfulsoundhabitsduetotheuseofpersonalstereodevicesis
highintheadolescentpopulation,buttherewasnocorrelationbetweenexposuretohighsound
pressurelevelsthroughpersonalstereosandthehigh-frequencythresholdsinthispopulation.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticle as:SilvestreRA, RibasÂ, Hammerschmidt R, deLacerda AB. High-frequencyprofilein adolescentsand its
relationshipwiththeuseofpersonalstereodevices.JPediatr(RioJ).2016;92:206---11.
夽夽
ThisarticlewaswrittenaspartofthethesisofthemainauthorforaMaster’sdegree.
∗Correspondingauthor.
E-mail:[email protected](R.A.A.Silvestre).
http://dx.doi.org/10.1016/j.jped.2015.07.008
PALAVRAS-CHAVE Audiometria; Adolescente; MP3player; Perdaauditiva; Prevenc¸ãoprimária
Perfildealtafrequênciaemadolescentesesuarelac¸ãocomousodeMP3players
Resumo
Objetivo: Analisarecorrelacionarosachadosaudiométricosdealtasfrequências(9---16kHz)
emadolescentescomseushábitoseatitudesdeaudic¸ãoparaprevenirperdaauditivainduzida
porruído.
Método: Esteéumestudotransversaldescritivoqueincluiu125adolescentesemumaamostra
de alunos ouvintes em uma escola estadual. Os indivíduos foram submetidos a testes de
audiometria dealtas frequências e responderama um questionárioautoadministrado
abor-dandoinformac¸õessobrehábitos sonoroscomrelac¸ãoao usodeMP3players. Aamostrafoi
divididadeacordocomascaracterísticasdeexposic¸ão(tempo,durac¸ão,intensidade,etc.)e
os resultadosforamcomparadosaoslimitesobservados,pormeiodoTestedeDiferenc¸ade
Proporc¸ões,Qui-quadrado,testeTdeStudenteanálisedevariância(ANOVA),todosem um
níveldesignificânciade0,05.
Resultados: Foiregistradamédiadelimiaresdealtasfrequênciasabaixode15dBHLenãofoi
encontradanenhumacorrec¸ãosignificativaentreosachadosaudiométricosdealtasfrequências
eograudeexposic¸ão.
Conclusão: AprevalênciadehábitossonorosprejudiciaisdevidoaousodeMP3playerséaltana
populac¸ãoadolescente,porémnãohouvecorrelac¸ãoentreaexposic¸ãoaaltosníveisdepressão
sonorapormeiodeMP3playerseoslimiaresdealtasfrequênciasnessapopulac¸ão.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Studiesrelatedtotherecreationalhabitswithexposureto highsoundpressurelevels(SPL),especiallythroughstereos for personaluse, haveproved toberecurringin different adolescentpopulations,withprevalentdataatover90%.1,2
Consideringthattechnologicaldevelopmenthasprovided increasing quality and power of earphones and headsets, withamplifiersthatreach130dBSPLwithoutsound inten-sitydistortion,3,4andcoupledwithpersonalstereoproducts
thatareinexpensive,highlyportable,storelarge volumes of music, and have long-life batteries, there has arisen a situationin which the personal stereo (PS) hasbecome particularlyprevalentandharmfulamongtheyoungurban population.4,5
Some possible explanations for such exposure involve: theneedforself-worthandsocialacceptance,leadingtothe adoptionoffadsinordertobecomeamemberofagroup6;
customizationpotentialofasoundenvironmentleadingto personalisolation4;andevenexperimentationwithpleasure
andeuphoriathatmayarisefromthereleaseofendorphins duetothephysiologicaldefensereactionthataccompanies exposuretosoundlevelsabove80dBSPL.7
Althoughmusichasbeenconsideredlessharmfultothe humanhearingsystemthananequivalentindustrialnoise, giventheformer’sintermittentnature,allowingfora hear-ingrecoveryperiod,alowerdominantfrequency,andmore discreet alert reactions due to personal interpretation of whether it is a pleasant sound6; one must highlight the
irreversiblecharacteristicofhighSPLinduced hearingloss (HSPLIHL),greatersusceptibilityofcochleardamageinthe youngestpopulations,8 andtheincreasein the
predisposi-tiontodevelophearinglossinadulthoodwhenthereisearly exposuretohighnoiselevels.9
Traditionally, the diagnosis of HSPLIHL, as well as its monitoring and verification, are performed by subjective audiometricthreshold testingobserved throughpure tone audiometry (PTA) and objective audiological evaluations, suchas auditory brainstem response (ABR) and otoacous-tic emissions (OAE) testing, especially distortion product (DPOAE).10
However, in view of the recognizedearly elevation of hearingthresholdsfor highfrequencies, comparedto nor-mal thresholds, in light of potentially harmful conditions for thecochlear system such asexposure tooccupational noiseand/orototoxicdrugs,certainsystemicand ontologi-caldiseases,aswellasduringtheprocessofauditoryaging. High-frequencyaudiometry(HFA)hasbeenindicated asan instrumentintheearlydiagnosisofhearinglosswhen com-paredtoPTAandOAE.11---15
ThisstudyaimedtoanalyzeHFAfindingsinadolescents andcorrelatethemwiththeiruseofPSs.
Method
This was a cross-sectional descriptive study approved by the Research Ethics Committee recorded under No. 2576.183/2011-08.Allparticipantssignedaninformed con-sentauthorizingtheuseofdatacollectedafterclarification regardingtheresearchobjectivesandprocedures.
Table1 Descriptionofsamplebyageandgender.
Age Female
(n=63)
Male
(n=62)
p
n % n %
12 2 3.17 2 3.23 0.9848
13 13 20.63 7 11.29 0.1569
14 17 26.98 12 19.35 0.3142
15 14 22.22 24 38.71 0.0473a
16 11 17.46 11 17.74 0.9673
17 6 9.52 6 9.68 0.9758
Total 63 50.04 62 49.60
---Note:Differenceofproportionstest,significancelevelof0.05.
ap<0.05.
research were students who had no habit of listening to musiconPSs(n=9).
Theevaluation,performedbyotorhinolaryngologist,paid specialattentiontonasalandsinusstructuresandstructures oftheouterandmiddleear,cleaningtheexternalauditory canalwhenneeded.
In the audiological evaluation, normalthresholds were considered to be up to 25dB HL per classification by LloydandKaplan(1978),16 andobtainedthroughpuretone
audiometry(500---8000Hz), performed withan Otometrics branddevice (Madsen Itera II®, Taastrup, Denmark), with
TDH39®headphones(MedRx,Inc.,RD,USA),calibratedina
soundenclosureinaccordancewiththestandardsrequired bytheBrazilianFederalSpeechCouncil.16Tomeasure
acous-ticimpedance,anInteracousticsbrandmiddleearanalyzer wasused,AT22®model(Otometrics®,Middelfart,Denmark),
andnormalresultswereconsideredtobethosecompatible withatypeAtympanogram,accordingtoJerger.16
Studentsincludedintheselectioncriteriawereinvitedto answeraself-administeredquestionnairecomposedofopen andclosedquestions,addressingsoundhabitsregardingthe use of PSs, including information on exposure character-istics(exposure time in years, days per week, and hours perday,insertionorearmuffphones,habitofsleepingwith theunitturnedon,habitoftalkingwhileusingthedevice,
andcommonlyusedintensity)andsymptomsassociatedwith exposure.Avisualanalogscalewasemployedfor estimat-ingthevolumerangecommonlyusedbythestudysubjects. Anyquestionsraised bythesubjectswereclarified bythe researchteam.
Next,anaudiometricevaluationofhighfrequencieswas carriedoutundertheacousticconditionsdescribedabove, withthe aforementioned audiometer, usingKOSS HV/PRO (KOSS®, USA) headphones, at thresholds expressed in dB
HL,atthefrequenciesof9000,11,200,12,500,14,000,and 16,000Hz.
TheresultswerestatisticallyanalyzedbytheChi-squared test, differencein proportions test, Student’s t-test, and ANOVA;the0.05significancelevelwasutilized.
Results
Uponestablishinginclusioncriteriausingperspectivesboth fromclinicalandaudiologicalnormality(n=134)aswellas PSuse(n=125),aprevalenceofPSusewasfoundamong nor-malhearingteenagers(93.28%).Acomparisonofthesample byageandgenderisshowninTable1.
AnalyzingthesamplebytimeofexposuretoPS,itwas found that 58.4% (n=73)of individuals made daily use of
Table2 DescriptionofsamplebyhabitsofPSuse.
PSexposuretime Female
(n=63)
Male
(n=62)
p
n % n %
Lessthan3years 32 50.79 43 69.35 0.0342a
3yearsormore 31 49.21 19 30.65
Upto4days/week 11 17.46 20 32.26 0.0054a
5ormoredays/week 52 82.54 42 67.74
Lessthan2hours/day 30 47.62 41 66.13 0.0367a
2ormorehours/day 33 52.38 21 33.87
Note:Chi-squaredtest,significancelevelof0.05. PS,personalstereo.
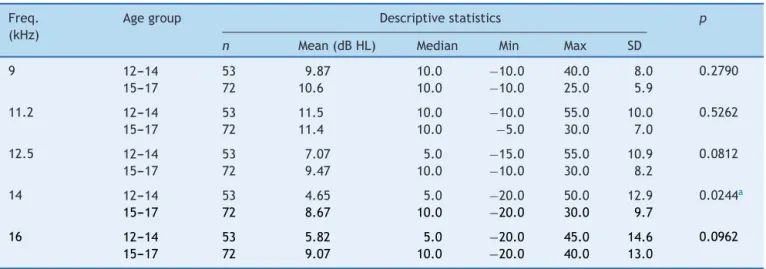
Table3 Descriptionofhearingthresholdsindecibelsatfrequenciesof9000---16,000Hz,byagegroup.
Freq. (kHz)
Agegroup Descriptivestatistics p
n Mean(dBHL) Median Min Max SD
9 12---14 53 9.87 10.0 −10.0 40.0 8.0 0.2790
15---17 72 10.6 10.0 −10.0 25.0 5.9
11.2 12---14 53 11.5 10.0 −10.0 55.0 10.0 0.5262
15---17 72 11.4 10.0 −5.0 30.0 7.0
12.5 12---14 53 7.07 5.0 −15.0 55.0 10.9 0.0812
15---17 72 9.47 10.0 −10.0 30.0 8.2
14 12---14 53 4.65 5.0 −20.0 50.0 12.9 0.0244a
15---17 72 8.67 10.0 −20.0 30.0 9.7
16 12---14 53 5.82 5.0 −20.0 45.0 14.6 0.0962
15---17 72 9.07 10.0 −20.0 40.0 13.0
Note:Student’st-test,significancelevelof0.05.
a p<0.05.
theirdevices,withequivalentanswersfromboth genders. However,usingtheChi-squaredtestat asignificancelevel of0.05,itwasobservedthattherewassignificantlylonger PSusebyfemales,perTable2.
Also, using the Chi-squared test, more harmful habits wereidentifiedamongfemalesforthefollowingvariables: habit of sleeping with the PS turned on (p=0.0037), and perceivedvolumebyothers(p=0.0458).Moreover,through thedifferenceinproportionstest,apreferencewasshown forinsertion-typeearphones(p=0.0150),withbothtestsat the0.05significancelevel.
It wasobserved thatalmost40% ofadolescents(n=49) had experienced at least one otological symptom due to theuseofPSS,withtinnitusprevalenceof21.6%,followed by ear pain, ear fullness, itching, dizziness, and hearing loss. Attempting to correlate the prevalence of otologic complaintswiththehabitualuseofPSSbyapplyingthe chi-squared test and thedifference of proportions Test, at a significancelevelof0.05,nosignificantdifferencewasfound betweenthosesubjectsmoreandlessexposed.
Evaluatingtheresultsofhearingthresholdsforthehigh frequenciestested,meanvalueswereobtainedbelow15dB HL,withslightlybetterresultsforfemalesfrom11,200Hz. With regard to inequalities between the ears, there was nostatisticallysignificantdifference,althoughslightly bet-ter answers for the right ear, only among females, were observed.
Considering both age groups, there was an average of higher thresholds in the older group for all frequencies testedexceptat11,200Hz.However,therewasonlya sig-nificantdifferenceat14,000Hz,withStudent’st-testatthe 0.05significancelevel.Thecharacterizationofthehigh fre-quencythresholdsageisshowninTable3.
Todescribeandanalyzetheresultsbygender,therewas astatisticallysignificantdifferenceinfrequenciesstarting at12.5KHzforthe15---17year-oldagegroup,withtheworst averagebeingamongmales.
The analysis of audiometric thresholds in terms of PS exposureshowednosignificantdifferenceinanyfrequently tested,whetherforPS-usedurationvariablesinyears,days
perweek,orhoursperday,usingStudent’st-test;norfor intensity variables or type of earphone using the ANOVA test,withboth tests at the0.05 significancelevel. There wassomehigheraverageinalltestedfrequencies,forboth ears,amongthosewhoused PSfor fiveor more daysper week.
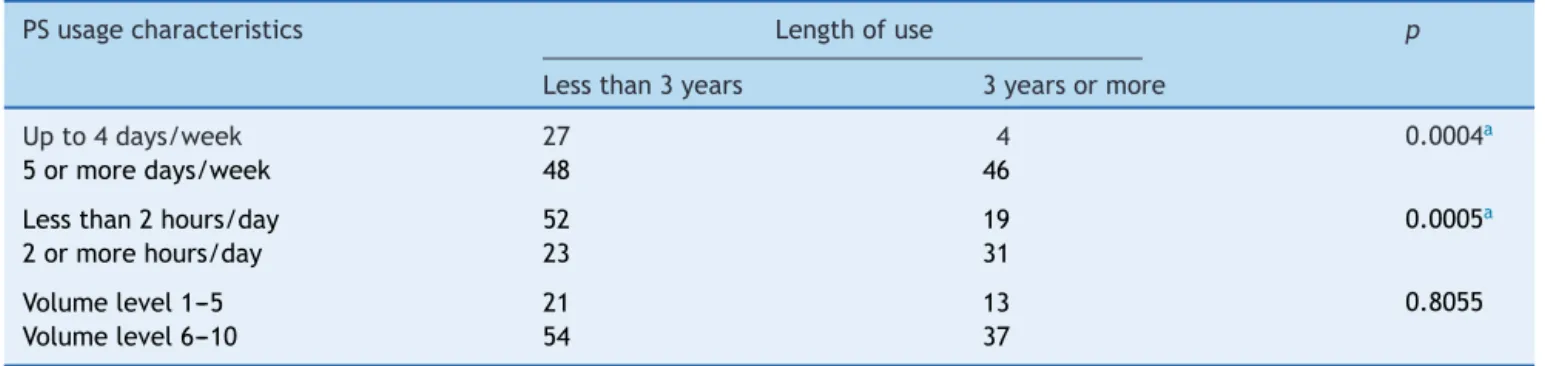
Correlations on exposure are described in Table 4, in whichlessPSusewasdemonstratedindaysperweekand hoursperdayforthesubjectswhostartedusingPSsmore recently.Apreferenceforhighersoundlevelintensity (vol-ume)wasalsoobservedamongthosewhomadeuseofthe devicesatleastfivedaysperweek.
Discussion
ThepopularizationoftheuseofPSs,particularlyinyounger populations, and the lack of regulation on the maximum sound output intensity of devices, have contributed to increasing recreational exposure to sound at high inten-sityinthisagegroup.4Thehigh prevalenceofhabitualPS
useobserved(93.28%)hasbeenrepeatedinstudies involv-ingadolescentpopulationsondifferentcontinents,reaching 95.6%ofsubjectsinsomesamples.1,2,7
The PS usage profile (Table 2), use for at least five daysaweek, atleasttwohoursperday,although forless thanthreeyears,reflectsthepresenceofpositiveattitudes toward noise in the adolescent population. This is a pat-tern of device misusethat has been identified in several studies.4,6,17---19
However,differentlyfromwhatiscommonlyreferredto instudies,20,21theobservationofmoredeleterioushabitsin
thefemalegroupmightbeexplainedbythegreaterneedfor isolationandaprevalenceofsymptomsrelatedtoanxiety anddepressionamonggirls.22,23
Table4 RelationshipsamonglengthofPSuseandusagecharacteristics(innumberofdaysperweek,numberofhoursperday,
andvolumelevel).
PSusagecharacteristics Lengthofuse p
Lessthan3years 3yearsormore
Upto4days/week 27 4 0.0004a
5ormoredays/week 48 46
Lessthan2hours/day 52 19 0.0005a
2ormorehours/day 23 31
Volumelevel1---5 21 13 0.8055
Volumelevel6---10 54 37
Note:Chi-squaredtest,significancelevelof0.05. PS,personalstereo.
ap<0.05.
otologicalsymptomscansignaltemporaryorpermanent sub-clinicalhearingdamage,thehighprevalence ofotological complaints(39.2%)amongthepresentsubjectsstandsout, althoughsomestudieshaveshownresultsupto67.2%.5
Comparingthepresenceoftinnitusamongmoreandless exposedgroups,nodifferenceintheprevalenceof otologi-calsymptomswasobserved,coincidingwithotherstudies,21
although some authors have identifieda positive correla-tionwithPSabusewhenthesubjecthasbeenexposedfor alongertime,5,22athigherintensities,andusing
insertion-styleearphones.2
Average thresholds below 15dB HL were identified for bothgendersinallfrequenciestested,supportingthe sug-gestionofadoptingsuchvaluesasparametersofnormality fortheadolescentpopulation.24Theidentificationofslightly
better results in the female group starting at 11,200Hz hasalsobeenrecurrentinhighfrequency studies, demon-stratingthedependenceofauditorythresholdswithmales alreadyinadolescence.25,26 The observation ofa notchat
thefrequencyof11,200Hzfortheresults inboysfindsno referenceintheliterature,althoughSulaimanetal.21have
observedpositivecorrelationbetweenPSvolumeusedand thresholdsat11.2and14kHz.
Withregardtothedisparitybetweenears,nodifferences betweenthethresholdswerefound,althoughslightlybetter responseswereseenintherightearinthemalegroup.This findingisquitecontroversialintheliteratureand,although someauthors present resultssimilartothoseidentified,27
there is no consensus on this issue, including findings of worsethresholdsontheright.28 Theabsenceofagreement
onthisvariableintheHFAmayresultfromalackof spec-ificationandstatistical processingofinterauralthresholds foundinsomestudies.
Thecharacterizationofhighfrequencythresholdsbyage group (Table 3) shows worse responses in the older age group,exceptatthefrequencyof11.2kHz,reinforcingthe directrelationofageontheHFAresultsinadolescence25,29;
however,studiesshownoagreementontheexactperiodof thebeginningofthisdecrease.24,26
Theanalysisofaudiometricthresholdsrelatedto expo-surecharacteristics(durationofPSuse,typeofearphone, volumeused,gender,etc.)showednosignificantdifference inanyfrequencytested.Nonetheless,itwasobservedthat inbothears,atallfrequencies,therewereworseresponses
inthegroupwithhabitualusageforfiveormoredaysper week,althoughwithnosignificantdifference.
Some studies have identified thresholds up to 6dB HL greaterinsubjectswithatleastfiveyearsofPSusewhen compared to unexposed subjects.25 In addition, although
thesestudiesdemonstratedapositivecorrelation,although weak, regarding PS use and increased responses at 11.2 and 14kHz,23 other authors failed to identify such a
correlation.30
In addition to methodological and sample group dif-ferencesamongseveralstudies, thepossibilityexists that subjectswithhigh SPLexposurewhowere investigatedin thisresearchhavenotshownhearingdamageduetherecent start of PS use (60% with use for less than three years). Moreover, thecorrelations related toexposure character-istics have shown that users withlonger timeof use also havemoreweeklyhoursofuse,andwithgreaterintensity (volume)amongregularusers.
Finally, during theanalyses, it wasrealized that some factorsmayhavelimitedthisstudy;thehomogeneityofthe sample, despitetherandomselection ofsubjects,didnot allowforgroupswithmajordifferencesinexposure.
Thus, further studies should be conducted with young people, but in broader age ranges and including a larger samplesize.Theauthorsalsorecommendlongitudinaland cross-sectionalstudiesbetweenexposuregroupsinorderto clarifyorreduceconflictingresults.
ItwasfoundthattheHFAfindingsweresuccessfully ana-lyzed,withemphasisontheobservationatthresholdsbelow 15dBHL,likelytofunctionasnormalreferencevaluesfor adolescence with a positive relationship to age in males startingfrom15yearsold.
Inparallel,therewashighprevalenceofharmfulsound habitsregardingtheuse ofPS. However,although no cor-relation was observed between exposure to high SPL and thresholds of high frequencies in the population studied, giventheirreversiblenatureofNIHL,audiological monitor-ing and educational measures tocontain such habits and attitudesareimportant.
Conflicts
of
interest
References
1.Vogel I, Verschuure H, Van der Ploeg CP, Brug J, Raat H. Estimated adolescent risk for hearing loss based on data from a large school-based survey. Am J Public Health. 2010;100:1095---100.
2.OghuDS,AsoegwuCN,SomefunOA.Subjectivetinnitusandits associationwithuseofearphonesamongstudentsofthe Col-legeofMedicine,UniversityofLagos,Nigeria.IntTinnitusJ. 2012;17:169---72.
3.BreinbauerHA,AnabalónJL,GutierrezD,CárcamoR,Olivares C,CarolJ.Outputcapabilitiesofpersonalmusicplayersand assessmentofpreferredlisteninglevelsoftestsubjectives: out-liningrecommendationsfor preventingnoise-induced hearing loss.Laryngoscope.2012;122:2549---56.
4.LeveyS, Fligor BJ, Cutler C,Harushimana I.Portable music playerusers:culturaldifferencesandpotentialdanger.Noise Health.2013;15:296---300.
5.LuzTS,BorjaAL.Sintomasauditivosemusuáriosdeestéreos pessoais.IntArchOtorhinolaringol.2012;16:163---9.
6.PellegrinoE,LoriniC,AllodiG,BuonamiciC,GarofaloG, Bonac-corsiG. Music-listeninghabits withMP3 playerinagroup of adolescents:adescriptivesurvey.AnnIg.2013;25:367---76.
7.KimMG,HongSM,ShimHJ,Kim YD,Che CII, YeoSG. Hear-ingthresholdofKoreanadolescentsassociatedwiththeuseof personalmusicplayers.YonseiMedJ.2009;50:771---6.
8.KhatterK.Personalmusicplayersandhearingloss:Arewedeaf totherisks?OpenMed.2011;5:137---8.
9.VanKampI,DaviesH.Noiseandhealthinvulnerablegroups:a review.NoiseHealth.2013;15:153---9.
10.European Commission. Potential health risks of exposure to noisefrompersonalmusicplayersandmobilephonesincluding amusicplayingfunction.Availablefrom:http://ec.europa.eu/ health/phrisk/committees/04scenihr/docs/scenihro018.pdf
[cited16.11.14].
11.MalucelliDA,MalucelliFJ,FonsecaVR,ZeigelboimB,RibasA, de Trotta F, et al. Hearing lossprevalence in patients with diabetes mellitus type 1. Braz J Otorhinolaryngol. 2012;78: 105---15.
12.KucurC,KucurSK,GozukaraI,SevenA, YukselKB,KeskinN, etal.Extendedhighfrequencyaudiometrynpolycysticovary syndrome.SciWorldJ.2013:482689.
13.Al-MalkyG,SuriR,DawsonSJ,SirimannaT,KempD. Aminogly-cosideantibioticscochleotoxicity inpaediatriccysticfibrosis (CF)patients:astudyusingextendedhigh-frequency audiome-tryanddistortionproductotoacousticemissions.IntJAudiol. 2013;50:112---22.
14.Büchler M, Kompis M, Hotz MA. Extended frequency range hearingthresholdsandotoacousticemissionsinacuteacoustic trauma.OtolNeurotol.2012;33:1315---22.
15.OttoniAO, Barbosa-Branco A, Boger ME, Garavelli SL. Study ofthenoisespectrumonhigh frequencythresholdsin work-ers exposed to noise. Braz J Otorhinolaryngol. 2012;78: 108---14.
16.SistemasdeConselhosFederaleRegionaisdeFonoaudiologia. Manualdeprocedimentosemaudiometriatonal, logoaudiome-triaemedidasdeimitânciaacústica.Availablefrom:http:// www.fonoaudiologia.org.br/publicacoes/Manual%20de%20 Audiologia.pdf[cited16.11.14].
17.GilliverM,CarterL,MacounD,RosenJ,WilliamsW.Musicto whoseears?Theeffecttosocialnormsonyoungpeople’srisks perceptionofhearingdamageresultingfromtheirmusic listen-ingbehavior.NoiseHealth.2012;14:47---51.
18.HooverA,KrishnamurtiS.Surveyofcollegestudents’MP3 lis-tening:habits,safetyissues, attitudes,and education.AmJ Audiol.2010;19:73---83.
19.MartinAH,GriestSE,SobelJL,HowarthLC.Randomizedtrial offournoise-inducedhearinglossandtinnitusprevention inter-ventionsforchildren.IntJAudiol.2013;52:41---9.
20.GillesA,vanHalG,deRidderD,WoutersK,vandeHeyning P.Epidemiologyofnoise-inducedtinnitusandtheattitudesand beliefstowards noise and hearingprotection inadolescents. PLoSONE.2013;8:1---8.
21.SulaimanAH,SeluakumaranK,HusainR.Hearingriskassociated withausage ofpersonal listeningdevicesamong urbanhigh schoolstudentsinMalaysia.PublicHealth.2013;127:710---5.
22.CoelhoCB.Epidemiologyoftinnitusinchildren.In:MøllerAR, LangguthB,DeridderD,KleinjungT,editors.Textbookof tinn-itus.NewYork:Springer;2011.p.39---45.
23.JuulJA.Hearingsymptomsinchildrenandadolescents: tinn-itus and temporary thresholds shifts [thesis]. 85f. Sweden: UniversityofGothenburg;2013.
24.Anastasio AR, Radael RD, Cavalcante JM, Hatzopoulos S. A reportof extended high frequencyaudiometry thresholds in school-age children withno hearing complaints.Audiol Res. 2012;2:39---42.
25.LePrellCG,SpankovichC,Lobari˜nasE,GriffithsSK.Extended high-frequencythresholdsincollegestudents:effectsofmusic player useand otherrecreational noise. JAm Acad Audiol. 2013;24:725---39.
26.KlagenbergKF,OlivaFC,Gonc¸alvesCG,LacerdaAB,Garofani VG,ZeigelboimBS.Audiometriadealtasfrequênciasno diag-nósticocomplementaremaudiologia:umarevisãodaliteratura nacional.RevSocBrasFonoaudiol.2011;16:109---14.
27.MehrparvarAH,MirmohammadiSJ,DavariMH,MostaghaciM, Mollasadeghi A, Bahaloo M, et al. Conventional audiometry, extendedhigh-frequencyaudiometry,andDPOAEforearly diag-nosisofNIHL.IranianRedCrescentMedJ.2014;16:1---6.
28.Lopes AC, Melo ADP, Santos CC. Estudo dos limiares de audibilidade nasaltasfrequências em trabalhadoresdaárea odontológica.IntArchOtorhinolaryngol.2012;16:226---31.
29.Lee J, Dhar S, Abel R, Banakis R, Grolley E, Lee J, et al. Behavioral hearing thresholds between 0.125 and 20kHz usingdepth-compensatederasimulatorcalibration.EarHear. 2012;33:315---29.