EVALUATION OF NURSING PRACTICE
AND NURSING EDUCATION’
Patricia A. Deimanz
Evaluation is a vital part of nursing management. This article describes the major focuses of evaluation in nursing, principle steps in the evaluation process, and requirements for effective evaluation that in turn give rise to important implications for members of the nursing profession.
Introduction
Evaluation is a timely topic, one now receiving considerable attention from nurs- ing groups around the world. Your selec- tion of “Methods of Evaluation” as the theme of the Eighth National Congress of the Nurses’ Association of Chile’ evidences concern about ways of determining the quality of both nursing and educational programs, and about ways of establishing quality control measures.
The nursing profession in Chile, as else- where, has discharged its responsibilities for ensuring quality to a certain degree by: (1) establishing requirements for those who enter the profession; (2) controlling the programs that prepare nursing personnel; and (3) confirming that those who complete these programs are competent -by means of examination and subsequent official recog- nition. However, no members of a profes- sion who hold themselves accountable for the practice of that profession can be satis- fied by the mere establishment and enforce- ment of such entry-oriented controls.
‘Paper prepared for the Eighth National Congress of the Nurses’ Association of Chile held at Temuco, Chile, on 4-9 September, 1977. Also appearing in Spanish in the R&tin de la Oficina Sanitaria Pan- americana 85(6):487-497, 1978.
zPAHO/WHO Nursing Adviser at the time this paper was prepared. At present Nursing Adviser, Division of Nursing, BHM, HRA, U.S. Department of Health, Education, and Welfare.
Evaluation reinforces professional ac- countability. Nursing practitioners are accountable for the quality of their work- accountable to themselves, to their patients, to the patient’s families, to other health team members, to the institutions and agen- cies involved, to the community, to the nursing profession, and by way of the nurs- ing profession to society as a whole (I). By the same token nurse educators are ac- countable to their profession, their teach- ing institutions, their students, and them- selves. In both cases, however, it is only possible to be accountable, which is to say answerable for quality, if the quality of one’s work is actually determined through evaluation.
The Evaluation Concept
In essence, evaluation is the process of determining the degree to which preselected objectives have been attained. Evaluation is an integral part of the management process, which can be viewed as encompassing the four steps of planning, organization, imple- mentation, and evaluation. As this sequence suggests, evaluation not only presupposes but relies on initial planning. A meaning- I ful evaluation simply cannot be performed unless the planning needed to define objec- tives has taken place.
Evaluation also requires the use of value judgments. Such judgments, made through- out the evaluation process, help de-
“Sound observation.
. . is not
for the sake of piling up miscel-
laneous information
or curious
fact, but for the sake of saving
life and increasing
health and
comfort”
-F.
Nightingale
(3).
(Photo: WHO/P.
Almasy.1
e
fine what behaviors,
products,
or outcomes
are desired, how these things should be ob-
tained, critical
elements to measure, the best
instruments
with
which
to measure
them,
and what decisions should
be reached
as a
result of the evaluation
(2).
At
the same time, standards must be estab-
lished in order to determine
how well the
desired objectives have been attained.
Natu-
rally,
such standards
are a prerequisite
for
evaluation.
Overall,
it is important
to recognize
that
evaluation
cannot
be performed
by merely
describing
a situation.
Evaluation
requires
collection
of data,
interpretation
of the
data, and recommendation
of actions indi-
cated
by that interpretation.
In addition,
for evaluation
to be truly
productive,
em-
phasis must be placed
on those indicated
actions
-actions
designed
to support,
strengthen,
or otherwise
modify
the services
involved.
Florence
Nightingale,
writing
about the
related process of observation,
expressed this
point very succinctly.
She said:
In dwelling
upon
the vital
importance
of
sound observation,
it must never be lost sight of
what observation
is for. It is not for the sake of
piling
up miscellaneous
information
or curious
facts, but for the sake of saving life and in-
creasing health and comfort (3).
What
this says of observation
applies
equally
well to evaluation-for
no evalua-
tion can be of any practical
worth
unless
good use is made of its results.
Different
Applloaches
to Nursing
Evaluation
ing the nursing care or teaching processes involved, and by assessing the end results or outcomes obtained. For convenience, the three are commonly referred to as “struc- ture,” “process,” and “outcome” evalua- tions.
To be a little more specific, structure evaluations generally consider the purpose, organization, fiscal resources and manage- ment, personnel qualifications, and physi- cal plant and equipment of the institution, agency, or program being assessed. Process evaluations (I) appraise the steps taken to care for patients or educate students for the purpose of attaining specified therapeutic or educational goals. And outcome evalua- tions assess the patient care or teaching process in terms of its end result-that is, in terms of the measurable impact the process has on patient health status or nurs- ing student behavior.
Generally speaking, these three types of evaluation require different methodologies and help answer different questions. Rele- vant questions to which each type is ad- dressed are as follows:
l
Structure evaluation:
Are the facilities,equipment, and manpower resources con- ducive to effective teaching or delivery of quality care?
l
Process
evaluation: Is the nursing pro-perly practiced? Or is the manner of teach- ing appropriate and adequate?
l
Outcome evaluation:
What effect doesthe nursing care or instruction have on pa- tient health status or student performance?
As these questions suggest, structure eval- uation places the focus on characteristics of practitioners and the setting; process eval- uation focuses on practitioner performance; and outcome evaluation is focused on the effects of the process on the patients, clients, or students.
These distinctions make it relevant to ask how the different types of evaluation relate to one another. Specifically, are the varia- bles appraised by one more significant than
the variables appraised by the others? And, in a similar vein, does it suffice to employ one type of evaluation alone, or should balanced use of the different kinds be made?
Because of the general nature of these queries and lack of extensive scientific data, the available answers are necessarily empirical. However, a few studies reported in nursing journals have pointed ?rp the close relationships existing between struc- ture, process, and outcome evaluations. The relevant findings of three such studies are briefly summarized below:
l Hegyvary and Hausmann (4) found a
number of structural variables to positively influence the quality of various components of the nursing process. In essence, these structural elements were: (1) organizational structure of the nursing unit; (2) the style of nursing leadership; (3 ) unit staff atti- tudes; (4) supervisory staff attitudes; and (5) graduate nurse preparation.
l A randomized trial of nurse praction-
ers providing primary health care focused attention on two outcomes-clinical effec- tiveness and safety. These outcomes were assessed in terms of the physical, emotional, and social conditions of two groups of patients-one receiving primary care from nurse practitioners and the other receiving conventional care. Besides demonstrating comparability of these two groups at the start of the study, the results showed similar levels of physical, emotional, and social functioning by both groups after receiving care for one year. In other words, the study showed the nurse practitioners to be pro- viding care that was both safe and effective (5). This outcome study thus provided an excellent basis for exploring the firocess of primary health care delivery by nurse prac- titioners.
l Yauger (6) has reported on an outcome
findings showed that the family-centered approach to health care had no significant impact on health outcome. These negative findings pointed up an urgent need to eval- uate the process involved. Or, as the author put it, “It is essential that the process of family-centered care be more closely iden- tified and evaluated. An intervention that is not producing results must either be changed or the whole concept eliminated”
(6).
As all these studies suggest, it is impor- tant for appraisals to be made on the basis of all three elements of evaluation-struc- ture, process, and outcome-rather than being restricted to just one or another element. Combining the results of all three types of evaluation will give a more com- plete picture of the quality of the services.
The Evaluation Process
The model of evaluation shown in Fig- ure 1 depicts it as a cyclical process con- sisting of the following general steps: (1) determine
what
is to be evaluated; (2) de- fine evaluationcriteria;
(3) plan the meth-odology
to be applied; (4) gather informa-tion; (5) analyze the
results;
(6) take action;and (7) re-evaluate.
Determining What Is To Be Evaluated
As the foregoing indicates, it has proven useful to have nursing evaluations focus on structures, processes, and outcomes. Logi- cally, then, the first step in planning an evaluation is to determine which of these are to be evaluated in order to achieve the desired aims. This implies, of course, that the aims of the evaluation must be defined initially so as to ensure consistency between the reasons for the evaluation and what is being evaluated. For example, if the evalu- ation seeks to identify strengths and weak- nesses of personnel performance, the main focus of the evaluation must clearly be on processes, although evaluation of structures and outcomes can be included as well. Once determined, this primary focus of the evaluation will play a large part in dictat- ing who should be responsible for carrying out the subsequent steps of the evaluation process.
Defining Evaluation Criteria
Generally speaking, a criterion used for evaluation purposes should constitute a baseline for measuring some event or be- havior (7) that is “established by authority, custom, or general consent” (8). Such a cri- terion should also be a single element in a given situation-an element that is clearly
Figure 1. A model of the evaluation process.
defined, measurable, and relevant to the situation or condition being assessed. These latter qualities are essential to the perform- ance of an objective evaluation that will yield valid results.
Structural criteria. Criteria must neces- sarily be developed in accordance with the focus of the evaluation. Structural criteria, with which we are particularly familiar, are elements relating to: the purpose of an institution, agency, or program; organiza- tional characteristics; fiscal resources and management: personnel qualifications; and physical facilities and equipment. Two examples of structural criteria are that a graduate nurse supervisor is present on each tour of duty at a hospital, or that an educational institution has at least one instructor for every 10 nursing students.
Process
criteria. These criteria, which relate to the performance of nursing per- sonnel or nurse educators, help measure such factors as: the nature of interactions between the nurse and the patient or client, or the nurse educator and student; the extent to which objectives are realized; the degree of skill with which techniques or procedures are executed; and the degree of consumer participation. Examples of process criteria are that the prenatal pa- tient receives at least 10 hours of instruc- tion; that the nurse develops a care plan for each patient; and that the instructor provides for course evaluation on the part of the students. Ideally, logically developed process criteria would permit a qualitative judgment concerning proper completion of each phase of the nursing care process. Using such criteria, the evaluator could determine the accuracy with which the pa- tient’s needs are identified, the appropri- ateness of the goals set, the adequacy of the interventions planned, and the skill with which these interventions are performed (7).Brief mention should also be made of performance appraisals. Unfortunately,
most formats for evaluating personnel call for judgment of personal characteristics such as appearance, initiative, quantity of work, and competence -rather than of actual performance. Nevertheless, the merits of measuring individual perform- ance against criteria established in accord- ance with job expectations can hardly be questioned. And although formulating cri- teria to judge the quality of role perform- ance is a time-consuming task, nurses who have done it report that the positive results obtained more than compensate for the time and energy required.
Outcome criteria. The third major type of criteria, outcome criteria, focus on mea- surable alterations in patient health status or student behavior resulting from health care or the educational process.
Health outcome criteria are unquestion- ably the most difficult to draft, due princi- pally to the multiple causes of health effects. It may be difficult, for example, to deter- mine if a case of wound sepsis was the fault of the surgeon, the nurse who changed the dressings, or personnel in the central sterile supply room. By the same token, if a surgical patient remains free of infection, it is not due to the efforts of nursing alone.
The problem of multiple causation, how- ever, is surmountable. Stevens suggests de- veloping outcome criteria applicable to groups of patients for whom similar out- comes are desired. That is, criteria could be formulated for patients with the same disease (e.g., cardiac patients), for those receiving similar treatment (e.g., preopera- tive patients), for those with like needs (e. g., geriatric patients), or for those at the same stage of an illness (e.g., patients re- quiring intensive care) (7).
a performance criterion is that the patient can identify his or her medications, while a state of being criterion is that the patient has intact skin in the affected area. In this regard, it is noteworthy that both types of outcome criteria could be formulated for any of the groups of patients mentioned in the preceding paragraph.
Develofiing and
checking
criteria. A relevant question at this point is who bears the responsibility for drafting criteria? Does it rest with nurse educators, nursing service personnel, or nursing administra- tors? My own belief is that development of structure, process, and outcome criteria should be done by all three groups working together. Nurse administrators should join forces with nurses with expertise in caring for pediatric patients and with instructors of pediatric nursing to develop pediatric criteria; and the same approach should be followed in other specialties. In fact, this same collaboration should occur regardless of whether the criteria developed are to be applied in the practice or educational set- tings. The underlying reason for this is that criteria should be developed by a rep- resentative group of nurses who have ex- pertise in administration, provision of care, and education in the particular field concerned.In addition, I am aware of one instance where auxiliary personnel were also in- volved in defining criteria. This had the gratifying effect of improving staff rela- tionships and unifying the staff in their efforts to do something about the quality of the care being provided.
Another significant point is that once criteria have been developed, the validity of those criteria needs to be checked. One way of doing this is by peer review, a method that yields added benefits by in- volving more nurses in the evaluation process, arousing their interest and enthu- siasm, and thereby enhancing implementa- tion of quality control efforts.
Planning the Methodology
A format in keeping with the purpose of the evaluation must be prepared for gather - ing the information desired. In addition, decisions must be made about the source of the information, how and when the infor- mation will be collected, and who will col- lect it. These decisions, especially the two former ones, should reflect full considera- tion of the need for accurate and efficient data collection.
Data sources may be direct or indirect. The former include direct observation of nursing performance and the results of nursing activities while reports by third parties, records, and reports by those who are the subject of evaluation fall into the latter category. In general, indirect sources tend to be less reliable, have more biases, and provide less valid information than direct sources (9).
Despite the fact that the patient, client, or student is an indirect data source, the importance and value of consumer partici- pation in evaluating the services received needs to be emphasized. For although the consumer may not have the background to assess care or instruction professionally, he or she is the
only
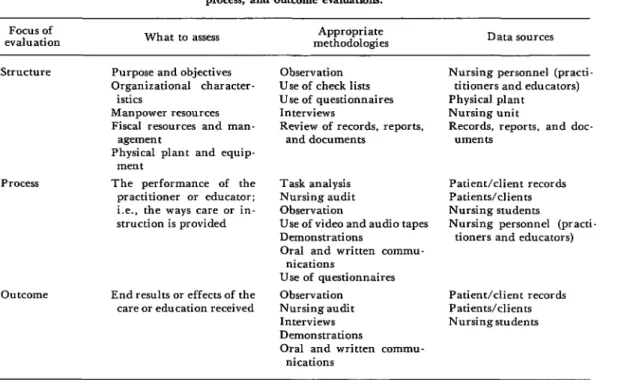
person who can judge whether his or her perceived needs were met.Various methodologies and data sources appropriate for structure, process, and out- come evaluations are shown in Table 1.
Gathering Information
The people responsible for collecting in- formation should receive adequate orienta- tion-irrespective of how simple the meth- odology employed may seem.
Table 1. Selected methodologies and data sources employ4 in structure, process, and outcome evaluations.
Focus of
evaluation What to assess
Appropriate
methodologies Data sources
Structure Purpose and objectives Organizational character-
istics
Manpower resources Fiscal resources and man-
agemen t
Physical plant and equip- ment
Process The performance of the practitioner or educator: i.e., the ways care or in- struction is provided
outcome End results or effects of the care or education received
Observation Use of check lists Use of questionnaires Interviews
Review of records, reports, and documents
Task analysis Nursing audit Observation
Use of video and audio tapes Demonstrations
Oral and written commu- nications
Use of questionnaires Observation Nursing audit Interviews Demonstrations
Oral and written commu- nications
Nursing personnel (practi- titioners and educators) Physical plant
Nursing unit
Records, reports, and doc- uments
Patient/client records Patients/clients Nursing students
Nursing personnel (practi- tioners and educators)
Patient/client records Patients/clients Nursing students
course and at its termination. Evaluation of student performance may be carried out whenever the student is in the clinical area-by means of self-assessments and in- structor assessments employing anecdotal notes. Performance appraisals of staff mem- bers are ordinarily done more frequently during each member’s probation period and less frequently thereafter. Three occasions that might be considered appropriate for assessing outcomes of hospital patient care are: (1) at the end of the critical stage of the patient’s illness; (2) upon the patient’s dis- charge from the inpatient unit; and (3) one or two months following discharge (10).
Analyzing the Results
Both interpretation of the data and feed- back to all individuals concerned should take place within the shortest time feasible
once the information has been gathered. In addition, opportunities should be provided for discussing the evaluation’s results-par- ticularly if those doing the reviewing and those reviewed are different parties.
Taking Action
Evaluation results may indicate a need to reinforce what is already being done, to modify procedures, or to introduce other changes. They may also call for shifting priorities, revising objectives, or developing new programs or services to meet previously unidentified needs.
referred to appropriate authorities; and here it must be recognized that the likeli- hood of receiving administrative approval and support is far greater when the requests for change are well-documented by the re- sults of a sound evaluation. To cite an obvi- ous case, a request that additional funds be spent on supplies might not succeed if the requesting parties give the impression that they wanted a well-stocked supply closet. Success would be more likely if the request were accompanied by a solid evaluation report which includes the incidence of post- operative wound infections.
Re-evaluation
When actions designed to improve the situation have been completed, another evaluation must be made in order to deter- mine whether or not they have had the de- sired effect. To state this point more gener- ally, evaluation is a cyclical process requir- ing continual repetition. And it is only to the extent that the nursing profession recog- nizes this fact and acts accordingly that con- tinuing improvement in the quality of nurs- ing programs can be assured.
Implications for Nursing
What has just been said about evaluation in general has some very specific implica- tions for those of us in nursing today. I would like to briefly mention four that appear most important.
l
The need to define @rogram or service
objectives in terms
ofhealth outcome.
Just as defining the behavioral outcome objec- tives of an educational program make the program more amenable to assessment, so the definition of health outcome objectives would facilitate health program evaluation. Such defined objectives, describing the de- sired health status of the patient or client served, in either intramural or extramural settings, would better enable nursing per-sonnel to gauge the effectiveness of the serv- ices provided. All nurses, but particularly those in the service setting, need to give this point serious consideration.
l
The need
forsystematic
evaluation ofrole changes.
The changing needs and de- mands for health services exert a profound influence on the nurse’s role-a role that over the last decade has tended to expand. This makes it essential that changes in the roles performed by nurses be planned for and systematically evaluated. Not only is this necessary in order to provide well- articulated nursing services and appropri- ate nursing education, but it is also neces- sary in order to determine whether the nurs- ing needs of society are actually being met.l
The
needto define relevant national
criteria.
It is imperative for nurses to define criteria that will be relevant for judging the quality of nursing practice and education - within the all-important context of their respective country’s social, cultural, and economic framework and health care deliv- ery system. This task might not be as Hercu- lean as it sounds if special groups of nurses were formed and each one assigned respon- sibility for defining criteria in a specific area. This process could be assisted by having the national nurses’ association de- velop a coordinating mechanism for sharing criteria developed by nurses from a variety of agencies and educational institutions.l
The need
fornursing leadershi@
ofSUMMARY Evaluation is a basic part of nursing manage- ment. Though there are many types of evalua- tion, it is possible to discern three predominant focuses in nursing, each viewing nursing activi- ties in a different way. These are “structure” evaluations which are concerned with the ad- ministrative and other structural elements underlying nursing activities; “process” evalua- tions which are concerned with nursing activi- ties themselves, and “outcome” evaluations which are concerned with the end results.
While it is difficult to generalize about the relative merits of each kind, it seems clear that wherever possible all three types should be em- ployed. That is because such combined evalua- tion is capable of giving the truest picture of the quality of the services being provided.
Another basic point is that evaluation is a cy- clical process that must be repeated. The basic steps involved are as follows: determine what is to be evaluated, define evaluation criteria, plan the methodology to be applied, collect data, analyze the results, take action, and re-evaluate the effects of that action.
Because ongoing evaluation is necessary for continuing improvement of the quality of nurs-
ing service and educational programs, the nurs- ing profession must be cognizant of and take appropriate action with respect to the following needs:
l The need to define program or service ob-
jectives in terms of health outcome. Such de- fined objectives would better enable nursing personnel to gauge the effectiveness of the pro- gram or services involved.
l The need for systematic evaluation of
changes in the nurse’s role. This is necessary in order to provide well-articulated nursing serv- ices, appropriate nursing education, and assur- ance that the nursing needs of society are actual- ly being met.
l The need to define relevant national crite-
ria. This is imperative for judging the quality of nursing care and education within the context of each country’s social, cultural, and economic framework and health care delivery system.
l The need for nursing leadership. Where
there is no multidisciplinary quality control pro- gram, nursing administrators must frequently assume a leadership role and establish quality control programs that will monitor the care being provided under their direction.
REFERENCES
(1) Phaneuf, M. C. The Nursing Audit: Pro- file for Excellence, Appleton-Century-Crofts,
New York, 1972, pp. 6 and 15.
(2) Arndt, C., and L.M.D. Huckabay. Nurs- ing Administration. C.V. Mosby, St. Louis, 1975, p. 136.
(3) Nightingale, F. Notes on Nursing. J. B. Lippincott, Philadelphia, 1946, p. 70.
(4) Hegyvary, S. T., and R. K. Hausmann. Correlates of the quality of nursing care.J Nurs Admin 6(9):22-27, 1976.
(5) Sackett, D. L., W. 0. Spitzer, M. Gent, et al. The Burlington randomized trial of the nurse practitioner: Health outcomes of patients. Ann Intern Med 80(2):137-142, 1974.
(6) Yauger, R. A. Program evaluation in com-
munity health nursing: Does family-centered care make a difference? Nurs Outlook 20(5):320- 323, 1972.
(7) Stevens, B. The Nurse as Executive. Con- temporary Publishing, Wakefield, Mass., 1975, pp, 128, 149, and 151.
(8) Ramey, I. G. Setting standards and evalu- ating care. J Nurs Admin 3(3):27-35, 1973.
(9) Hagen, E. Conceptual issues in the ap- praisal of the quality of care. In: U.S. Depart- ment of Health, Education, and Welfare, Assess- ment of Nursing Services, Bethesda, Maryland, 1975, p. 61.