rev bras hematol hemoter. 2016;38(1):79–81
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
RHD*weak
D
type
38
:
a
family
study
Sidneia
Sanches
Costa
a,b,
Akemi
Chiba
a,
Bruno
Cruz
a,
Dante
Langhi
Júnior
b,
José
O.
Bordin
a,∗aUniversidadeFederalSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2September2015 Accepted18October2015
Availableonline21November2015
Introduction
TheRHDgeneisresponsiblefortheexpressionoftheDantigen whileRHCEencodesproteinscarryingantigensCorc,andE ore.RHDispresentorabsentdependingontheRHhaplotype, andRHCEdisplaysfourcommonalleles(ce,Ce,cE,CE) respon-siblefortheexpressionofthetwoantithetical(allelic)series ofantigens.RHDgenedeletionistheleadingcauseofthe D-phenotypeworldwide.1Functional(antigen)variationsinthe
Rhblood groupsystemisdeterminedbyinsertion/deletion, singlenucleotidepolymorphisms(SNPs),andgeneconversion eventsintheRHDandRHCEgenes.AweakDtypeisavariant oftheRhDproteinthatcomprisesanaminoacidsubstitution locatedinthetransmembraneousorintracellularsegments andexpressesareducedamountoftheDantigen[generally lessthan5000Dantigensperredbloodcell(RBC)].2,3
TheRHD*weakDtype38isproducedbythesinglenucleotide
change(833G>A)intheexon6,causingaGly278Asp substitu-tioninthetransmembraneousRhDprotein.ThisRHDallele showsreducedexpressionoftheDantigenontheRBC sur-faceandmaybeerroneouslytypedasDnegativebystandard serologicmethods.4–6ThefrequenciesofweakDtype38vary
indifferentpopulations.TheweakDtype38was foundin
∗ Correspondingauthorat:RuaDiogodeFaria,824,04023-061SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](J.O.Bordin).
1.5%ofCaucasianswiththeCceephenotype,4whilea
rela-tivelyhigherfrequencyof2.6%wasrecentlydetectedamong BrazilianswiththeCceephenotype.6AlthoughtheRHD*weak
Dtype38isconsideredaveryrareallele,itisrelatively com-moninthePortuguesepopulation.7Inthisstudyweanalyzed
threegenerationsofafamilywithRHD*weakDtype38using serologicandmolecularmethods.
Case
report
Familystudyandbloodsamples
Asamplefroma45-year-oldfemaleblooddonorwastestedD negativebyroutineserologictests(Cceephenotype)but posi-tivebytheadsorption-elutiontechnique.Inordertoelucidate theseresultsweexaminedbloodsamplesfrom12members ofherfamilywereexamined.
Immunohematologic serological tests were performed using commercial monoclonal antibodies (MoAbs) MS-26+TH-28 and ESD1 by classical serology techniques, hemagglutinationingelcards(DiaMed,LatinoAméricaS.A.) andbythetubemethodswithanti-DMoAbsIgM(HM10,P3X61, P3X21211F1,P3X21223B10;Diagast,Loos,France)andanti-D
http://dx.doi.org/10.1016/j.bjhh.2015.10.001
80
revbrashematolhemoter.2016;38(1):79–81II-1
III-1
dce/dce Weak D type38 Ccee III-2 dce/dce
II-2 II-3
III-3
DCcee DCcee
III-4
II-4 II-5
DCcee Weak D type 38
Ccee
Weak D type 38 Ccee Weak D type 38
Ccee Weak D type 38
Ccee Weak D type 38
Ccee Weak D type 38
Ccee
I-2
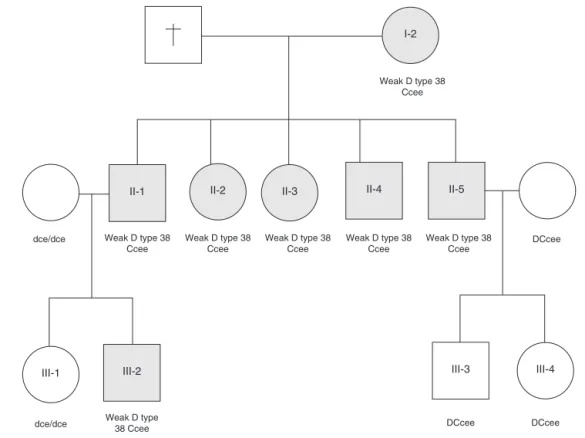
Figure1– PedigreeoffamilywithRHD*weakDtype38.
MoAbsIgG usingtheindirect antiglobulintest(IAT) (HM16, P3X35, P3X241, P3X249, P3X290; Diagast, Loos, France). Rh phenotypeswereperformedbyhemagglutinationingelcards, accordingtothemanufacturer’sinstructions(DiaMed,Latino AméricaS.A.)usingpolyclonalantibodiesagainstD,C,c,Eand e.
TheDantigendensityofsampleswasdeterminedbyflow cytometry(FACSCalibur, Becton Dickinson,Heidelberg, Ger-many) according to a previously described protocol8 with
sevenanti-DIgGMoAbs,HM16,P3X35,P3X241,P3X249,P3X290 (Diagast,Loos, France)and MS26and ESD1(DiaMedLatino AméricaS.A.).
Bloodsamplesfromfamilymemberswereinvestigatedby polymerasechainreaction(PCR)withspecificprimersfortwo genomicregionsoftheRHDgene,intron4andexon10andall tenRHDexonsweresequencedfulllength.9,10
WefoundsevenmembersofthisfamilytestedDnegative byroutineserologictests(Ccee phenotype)and positiveby theadsorption–elutiontechnique.TheirRBCsreacted nega-tivelytofourIgManti-D,butshowedweaklypositiveresults withfourIgGanti-Dreagents(P3X249,P3X35,P3X241,HM16) (Table1).Theflowcytometricanalysisofsamplesfromthese sevensubjectsshowedDantigendensitiesrangingfrom60 to80sitespercell.Molecularanalysisidentifiedthepresence
ofRHD*weakDtype38inthreegenerationsofthisBrazilian
family(Figure1).
Discussion
Thisstudyrevealedmaternalinheritance(firstgeneration)of
theRHD*weakDtype38withtheCceephenotypebyherfive
Table1–Patternofreactivityseenwithdifferentclones ofanti-DantibodiesandDantigendensitiestested againstredbloodcellsfromindividualswithRHD*weak Dtype38.
Anti-DMoAb Depitope Isotype Reactivity
P3X249 2.1 G (±)
P3X290 3.1 G (−)
ESD1 4.1 G (−)
P3X35 5.4 G W
P3X241 5.4 G (±)
HM16 6.4 G W
P3X61 6.4 M (−)
HM10 6.6 M (−)
P3X21211F1 8.2 M (−)
P3X21223B10 9.1 M (−)
MS26 9.1 G (−)
DAntigendensitiesa 60–80sites/cell
MoAb:monoclonalantibody;(−):negativeresult;W:weakresult; (±):veryweakresult.
a Dantigendensitiesdeterminedbyflowcytometrywithanti-DIgG
monoclonalantibodies.
childrenandthesecondgenerationshowedpaternal inheri-tancebyason.ThisfamilyevaluationshowedthatRHD*weak Dtype38wasinheritedasanancestralallele.
Inconclusion,thisstudyfoundarelativelyhighprevalence
ofRHD*weakDtype38inBrazilians,rememberingthatBrazil
was colonized by the Portuguese.6,7 This isthe first report
revbrashematolhemoter.2016;38(1):79–81
81
DnegativebystandardserologicmethodsincludingIAT.Thus, thiscouldrepresentapotentialriskinbloodtransfusionsince unitsofbloodcollectedfromtheseindividualscouldbe trans-fusedtoD-negativerecipientscausingRhDalloimmunization.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FlegelWA.ThegeneticsoftheRhesusbloodgroupsystem. BloodTransfus.2007;5(2):50–7.
2. WagnerFF,GassnerC,MüllerTH,SchönitzerD,SchunterF, FlegelWA.MolecularbasisofweakDphenotypes.Blood. 1999;93(1):385–93.
3. FlegelWA.Moleculargeneticsandclinicalapplicationsfor RH.TransfusApherSci.2011;44(3):81–91.
4. Ansart-PirenneH,Asso-BonnetM,LePennecPY,RousselM, PatereauC,Noizat-PirenneF.RhDvariantsinCaucasians: consequencesforcheckingclinicallyrelevantalleles. Transfusion.2004;44(9):1282–6.
5.MotaM,DezanM,ValgueiroMC,SakashitaAM,KutnerJM, CastilhoL.RHDallelicidentificationamongD-Brazilianblood donorsasaroutinetestusingpoolsofDNA.JClinLabAnal. 2012;26(2):104–8.
6.CostaS,MartinF,ChibaA,LanghiDJr,ChiattoneC,BordinJ. RHDallelesandDantigendensityamongserologicallyD−C+ Brazilianblooddonors.TransfusMed.2014;24(1):60–1.
7.RodriguesMJ,RodriguesF,TilleyL,PooleJ,ChabertT,SouzaG. SeveralnewexamplesofweakDtype38inthePortuguese population.Transfusion.2006;46Suppl.:141A–2A
(abstract).
8.FlegelWA, ˇCurin- ˇSerbecV,DelamaireM,DonvitoB,IkedaH, JørgensenJ,etal.Section1B:RhFlowcytometry.
Coordinator’sreport.RhesusIndexandantigendensity:an analysisofthereproducibilityofflowcytometric
determination.TrendsCellBiol.2002;9(1):33–42.
9.LeglerTJ,MaasJH,KöhlerM,WagnerT,DanielsGL,PercoP, etal.RHDsequencing:anewtoolfordecisionmakingon transfusiontherapyandprovisionofRhprophylaxis. TransfusMed.2001;11(5):383–8.
10.QunX,Grootkerk-TaxMG,Maaskant-vanWIijkPA,vander SchootCE.Systemicanalysisandzygositydeterminationof theRHDgeneinaD-negativeChineseHanpopulationreveals anovelD-negativeRHDgene.VoxSang.2005;88(1):