REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Publicação Oficial da Sociedade Brasileira de Anestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Construction
of
a
tool
to
measure
perceptions
about
the
use
of
the
World
Health
Organization
Safe
Surgery
Checklist
Program
Luis
Antonio
dos
Santos
Diego
a,b,
Fabiane
Cardia
Salman
a,c,
João
Henrique
Silva
a,d,
Julio
Cezar
Brandão
a,e,f,g,∗,
Getúlio
de
Oliveira
Filho
a,f,h,
Antonio
Fernando
Carneiro
a,
Airton
Bagatini
a,
José
Mariano
de
Moraes
aaSociedadeBrasileiradeAnestesiologia(SBA),RiodeJaneiro,RJ,Brazil
bFaculdadedeMedicina,UniversidadeFederalFluminense(UFF),Niterói,RJ,Brazil cFundac¸ãoOswaldoCruz,RiodeJaneiro,RJ,Brazil
dHospitalMoinhosdeVento,PortoAlegre,RS,Brazil
eUniversidadeFederaldeSergipe(UFS),SãoCristóvão,SE,Brazil
fTranslationalMedicine,UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil gMassachusettsGeneralHospital,Harvard,USA
hUniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
Received2September2014;accepted11November2014 Availableonline1May2016
KEYWORDS Tool; Checklist; Safesurgery; Adverseevents; WorldHealth Organization
Abstract
Background: The World Health Organization (WHO) hasrecommended greater attention to
patientsafety,particularlyregardingpreventableadverseevents.TheSafeSurgerySavesLives (CSSV)programwasreleasedrecommendingtheapplicationofasurgicalchecklistforitemson thesafetyofprocedures.Thechecklistimplementationreducedthehospitalmortalityratein thefirst30days.InBrazil,wefoundnostudiesofanesthesiologists’adherencetothepractice ofthechecklist.
Objective: Themainobjectivewastodevelopatooltomeasuretheattitudeof
anesthesiolo-gistsandresidentsregardingtheuseofchecklistintheperioperativeperiod.
Method: This was across-sectional study performedduring the59th CBA inBH/MG, whose
participants wereenrolledphysicianswho respondedtothequestionnairewith quantitative epidemiologicalapproach.
Results:Fromthesampleof459participantswhoansweredthequestionnaire,55%weremale,
44.2%under10yearsofpractice,and15.5%withover30yearsofmedicalschoolcompletion.
∗Correspondingauthor.
E-mail:juliobrand@hotmail.com(J.C.Brandão).
http://dx.doi.org/10.1016/j.bjane.2014.11.011
Sevenitemswith78%reliabilitycoefficientwereselected.Therewasastatisticallysignificant differencebetweenthegroupsofanesthesiologistswhoreportedusingtheinstrumentinless ormorethan70%ofpatients,indicatingthattheattitudequestionnairediscriminatesbetween thesetwogroupsofprofessionals.
Conclusions:Thesevenitemsquestionnaireshowedadequateinternalconsistencyanda
well-definedfactorstructure,andcanbeusedasatooltomeasuretheanesthesiologists’perceptions aboutthechecklistusefulnessandapplicability.
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Ferramenta; Checklist; Cirurgiasegura; Eventosadversos; Organizac¸ãoMundial daSaúde
Construc¸ãodeumaferramentaparamedidadepercepc¸õessobreousodochecklist
doProgramadeCirurgiaSeguradaOrganizac¸ãoMundialdaSaúde
Resumo
Introduc¸ão:AOrganizac¸ãoMundialdaSaúde(OMS)temrecomendadoumamaioratenc¸ãocom
aseguranc¸adopaciente,maisespecificamenteemrelac¸ãoaoseventosadversosevitáveis.Foi lanc¸adooprograma‘‘CirurgiaSeguraSalvaVidas(CSSV)’’,querecomendaaaplicac¸ãodalista deverificac¸ãocirúrgica(checklist)para aconferênciadeitensrelacionadosàseguranc¸ado procedimento.A implantac¸ãodochecklistreduziuamortalidadehospitalarnosprimeiros30 dias.NoBrasil,nãoforamidentificadosestudossobreadesãodosanestesiologistasàpráticado
checklist.
Objetivo:Desenvolvimentodeumaferramentaparamensurac¸ãodaatitudedos
anestesiologis-taseresidentesemrelac¸ãoaousodochecklistnoperíodoperioperatório.
Método: Estudotransversalfeitoduranteo59◦ CongressoBrasileirodeAnestesiologia(CBA),
em BeloHorizonte (MG),cujosparticipantes forammédicos inscritosequeresponderam ao questionáriocomabordagemepidemiológicaquantitativa.
Resultados: A amostraconstou de459 participantesque responderamao questionário, 55%
dosexomasculino, 44,2%commenosde10 anose15,5%acimade30anosdeconclusãodo cursomédico.Foramselecionadosseteitenscomcoeficientedeconfiabilidadede78%.Houve diferenc¸aestatisticamentesignificativaentreosgruposdeanestesiologistasquereferiramusar oinstrumentoemmenosoumaisde70%dospacientesassistidos.Issoindicaqueoquestionário deatitudesdiscriminaentreessesdoisgruposdeprofissionais.
Conclusões:Oquestionáriodeseteitensmostrouadequadaconsistênciainternaeuma
estru-turafatorialbemdelimitada.Podeserusadocomoferramentaparamedidadaspercepc¸õesde anestesiologistasquantoàutilidadeeaaplicabilidadedochecklist.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The 55th World Health Assembly, World Health Organiza-tion(WHO),throughtheResolution55.18hasrecommended toitsmemberstatesincreasedattentiontopatientsafety, particularly regarding preventable adverse events. So, in October 2005 it was introduced the first Global Patient SafetyChallengewiththetheme:CleanCareisSaferCare, whilethesecondGlobalChallengeaddressedthe fundamen-talsandpracticesofsurgicalsafetyfocusingonprevention ofsurgicalsiteinfections,safeanesthesia,surgicalteams, anduseofindicatorsforsurgicalcare.
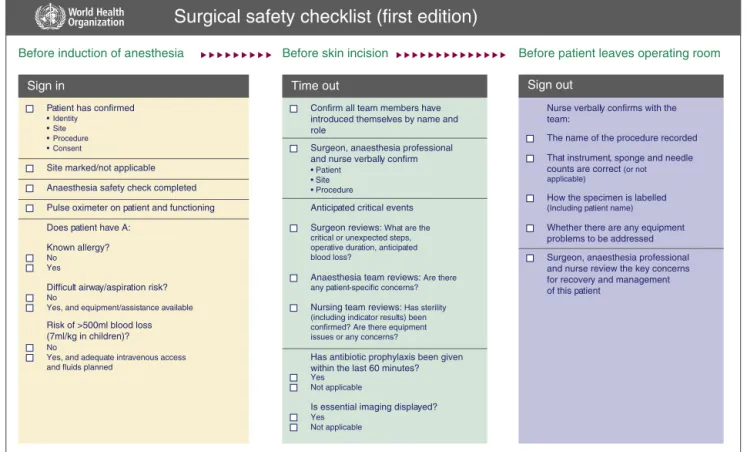
In2009,theWHOlaunchedtheSafeSurgerySavesLives (SSSL)program,1whichrecommendstheapplicationofthe
surgicalsafetychecklist,whichdeterminesthreebreaksin theperioperative periodfor checkingthe itemsregarding procedure security. The checklist and its implementation manualwere translatedintoPortuguese and publishedby theMinistryofHealth/ANVISA/PAHO(Fig.1).
Themethodchosen2fortheproject‘‘SafeSurgery’’was
based on the tool created at the Johns Hopkins Medical Institutionforimprovedcommunicationamongprofessionals participatingintheoperatingroomteam.Themain objec-tive wasfor all the operation planning tobeshared and, thus,facilitatetheintegrationintheprocedure implemen-tation.
Thisstructuredcommunicationtool,inspiredbyaviation, fragmentscomplextasksinmorewatertightsteps,inorder toreducethechancesofforgettingakeyitemforthe qual-ityandsafetyofthewholecare.Checkingtheitemslistedin apreviouslymadechecklistspeedstheprocessand,atthe same time,creates barriers toany process failures.3 One
Patient has confirmed
• Identity • Site • Procedure • Consent
Site marked/not applicable
Anaesthesia safety check completed
Pulse oximeter on patient and functioning
Does patient have A:
Known allergy?
No Yes
Difficult airway/aspiration risk?
No
Yes, and equipment/assistance available
Risk of >500ml blood loss
(7ml/kg in children)?
No
Yes, and adequate intravenous access and fluids planned
Nurse verbally confirms with the team:
The name of the procedure recorded
That instrument, sponge and needle
counts are correct (or not
applicable)
How the specimen is labelled
(Including patient name)
Whether there are any equipment
problems to be addressed
Surgeon, anaesthesia professional and nurse review the key concerns for recovery and management of this patient
Sign in
Confirm all team members have introduced themselves by name and role
Surgeon, anaesthesia professional and nurse verbally confirm
• Patient • Site • Procedure
Anticipated critical events
Surgeon reviews: What are the
critical or unexpected steps, operative duration, anticipated blood loss?
Anaesthesia team reviews: Are there
any patient-specific concerns?
Nursing team reviews: Has sterility
(including indicator results) been confirmed? Are there equipment issues or any concerns?
Has antibiotic prophylaxis been given within the last 60 minutes?
Yes Not applicable
Is essential imaging displayed?
Yes Not applicable
Time out Sign out
Before induction of anesthesia Before skin incision Before patient leaves operating room
Surgical safety checklist (first edition)
This checklist is not intended to be comprehensive. Additions and modifications to fit local practice are encouraged.
Figure1 Surgicalsafetychecklist.
Haynesetal.4The useofchecklisthasbeen stimulatedby
accreditingorganizationsoperatingin Brazil thatconsider itan instrumentof perioperativebestpractices,5 but one
cannotsay thatit hasbecome awidespread andcommon practice.Newprocedureslikethisamonghealth profession-als arenotalwaysreceivedpositivelyat first,particularly whentheeffectivenessofitsresults,thoughperemptory,is noteasilydemonstratedintheshortterm.
Thus,adherencetochecklistdependsonhavingpositive attitudesandperceptionsregardingitsusefulnessand appli-cability,inserted,preferably,ininstitutionsthatemphasize safety culture, because it is believed to be an essential requirement to reduce the occurrence of adverse events affecting rates security and entail reduction of patients’ morbidityandmortality.6---12TheimplementationoftheSafe
SurgeryChecklistProgramreducedhospitalmortalityinthe first30days.Althoughtheimpactontheoutcomewaslower than previously reported,the effectdepends crucially on theadherencetotheroutineuseofthechecklist.12
InBrazil,wefoundnostudiesofanesthesiologists’ adher-enceto theWHO ‘‘Surgical Safety Checklist’’norreports onadherence totypeof subgroupsof healthcare institu-tion,departmentofanesthesiologypracticeandprocedure complexity. Thus, assessing the attitude of profession-als regarding adherence to checklist is very important, particularly in the development of educational activities thatencouragethesafetyculture,asanesthesiologistsare present in all threestages of its implementation,aswell asnursingstaff.Thechecklistintroductioninseveral Euro-peancentersalsofacedbarriersandbiasesandledtosome
difficultiesinitsimplementation,butwiththesafetyculture inanesthesiatherewasabetterstandardofacceptanceand modificationof thestandard practiceof suchcentersand adequacyforthechecklistregularuse.12---14Themain
objec-tiveofthisstudywasthedevelopmentofatooltomeasure theattitudeofanesthesiologistsandresidentsregardingthe useofthechecklistintheperioperativeperiod.
Method
Cross-sectional study performed during de 59th Brazilian AnesthesiologyCongressinBeloHorizonte(MG),whose par-ticipantswereenrolledanesthesiologistsandresidentswho went to the stand of the Brazilian Society of Anesthesi-ology (SBA) and voluntarily responded to the web-based self-administered electronic questionnaire with quantita-tiveepidemiologicalapproach.Thestudywasapprovedby theResearchEthicsCommitteeoftheNationalInstituteof Cardiology,andwritteninformedconsentwasobtainedfrom allparticipants----anonymitywasguaranteed.
The instrument design prioritized the inclusion of questions that could contribute to the understanding of perceptions and attitudes of the profession being stud-ied. Responses were obtained on a 5-point Likert scale7
Table1 Meandifference between total andfactorial scores of questionnairebetween anesthesiologists groups using the checklistinlessormorethan70%ofpatients.
Meandifference 95%MeandifferenceCI p
Inferior Superior
F1 −0.31 −0.42 −0.20 0.00
F2 −0.15 −0.29 −0.02 0.03
Total −0.25 −0.35 −0.14 0.00
been formulated in a positive way, or 1 and 2 (strongly disagree/partially disagree) to the questions formulated negatively.Inthisprocess,thescoresassignedtoitemswith negativeconnotations(1and2tothequestionsformulated positivelyand4and5tothoseformulatednegatively)were reversed,soastoproduceaninstrumentwithmean maxi-mumrangeequalto5points,representingthebestattitudes andperceptionsregardingthechecklist.
The questionnaire reliability was evaluated through internalconsistency,estimatedbytheCronbach’salpha reli-abilitycoefficient,relevantbecausethequestionnairewas appliedonceinthesample.Cronbach’salphavaluesrange from0 to1and thelowerlimitusuallyacceptedis 0.60.8
Afterselecting theitems usingthe correlation coefficient withtotalscore≥0.3,theCronbach’salphacoefficientwas
calculated.Theselecteditemsweresubjectedtoprincipal componentsfactor analysiswithorthogonalrotation (Vari-max)toidentifythefactorialstructureoftheinstrument.
Discriminantvalidityoftheinstrumentscoreswastested bycalculatingthedifferencebetweenthefactorandtotal scoresofthequestionnaireamonganesthesiologistsgroups whoreportedusingthechecklistinlessormorethan70%of patients(Table1).
Predictivevaliditywasassessed(a)usingthecalculation ofSpearman’scorrelation coefficientsbetween thescores andthebinaryvariableofchecklistuseinlessormorethan 70%ofcases(theoutcomevariable)and(b)theanalysisof theROCcurveparametersbetweenthetotalscoreandthe outcomevariable.
Results
The total sample of 459 participants who completed the questionnaireinfourdaysoftheaforementionedCongress, 55% male and 44.2% with less than 10 years and 15.5% over30yearsofmedicalschoolcompletion.Only2.2%said theyhavedoneorbedoingaspecializationcourseor resi-dencyinanesthesiology.Theaverageageofparticipantswas 40.7years.
Seven items with 78% reliability coefficient were selected.Factoranalysisidentifiedtwofactors:F1,related totheperceptionoftheutility,andF2relatedtothe per-ceptionoftheapplicabilityofthechecklist(Table2).These twofactorsexplained58%ofthevarianceinscores.
Therewasastatisticallysignificant differencebetween the groups of anesthesiologists who reported using the instrumentinlessor morethan70%of patients.This indi-catesthattheattitudequestionnairediscriminatesbetween thesetwogroupsofprofessionals.
Table2 Perceivedutilityfactorsandapplicability.
Questionsregardingtheperceptionfactoronutility(F1)
•Areyoufamiliarwiththe‘‘SafeSurgerySavesLives’’
project(Checklist)?
•Itisusefulandpreventserrorsduringsurgery •Itisusefulandpreventserrorsduringanesthesia •Checklistshouldbemandatory
Questionsregardingtheperceptionfactoronapplicability
(F2)
•ShouldbeusedonlyininstitutionswithHospital
Accreditation
•Shouldbeappliedsolelybynurses
•Checklistisnotapplicabletoinvasiveproceduresinthe
DiagnosticCenter,suchasspinalinfiltration
Thecorrelationcoefficientsbetweenthefactorandtotal scoresandtheoutcomevariablewererho=0.32,p<0.01for F1scores;rho=0.14,p<0.02forF2scores;andrho=0.28, p<0.01fortotalscore.Thesevaluesaresignificant,butthe predictivevalidityof thequestionnaireis low.These find-ingsaresubstantiatedbythepercentageofareaunderthe curve=0.66(0.61---0.71).Thisindicates lowsensitivityand specificity of the instrument asa predictor of the use or non-useofthechecklistinmorethan70%ofpatientsseen byanesthesiologists.
Discussion
TheWHOSafeSurgerySavesLivesprogramaimstoincrease thequalityandsafetystandardsinhealthcare;contemplate theprevention ofsentinelevents, surgicalsite infections, safeanesthesia,safesurgicalteams,andindicatorsof sur-gicalcare.Itwasdecidedthattheinstrumentwouldserve acore set ofsafetystandardsthatcouldbe applied glob-allyand in differentscenarios. Inthis set, itwas obvious themultidisciplinarycharacter,includingallwhoworkand contributetotheexcellenceofpatientcare.
The use of checklist is being monitored by the WHO,9
andcurrentlyabout1800healthcarefacilitiesreporttheir systematicuse,particularlyinthecountriesofNorth Amer-icaandEurope,inadditiontoanincreasingimplementation inAsia andMiddleEast.Brazil, sofar,does notappearas oneofthecountriesthatexpresstheuseofchecklisttoits fullest.
TheSBApresentedtheWHO‘‘SafeSurgerySavesLives’’ project to Brazilian anesthesiologists for the first timein 200910 and,sincethen,theQualityandSafetyCommission
in Anesthesia (CQSA) hasbeen promoting theproject dis-seminationactionsinallofficialeventsoftheSociety and many ofits regionalfacilities nationwide.However,there wasnoway tohave an estimate of anesthesiologistswho workinthecountryandusethechecklist.Thus,theBoard ofSBAin2012acceptedtheproposalofCQSAtoperforma surveyduringthe59thCBAinBH/MGandprovidedresources forthesurveyapplicationpresentedhere.
The choice of the event was due primarily to allow that the largest number of participants could respond to the questionnaire, as the number of subscribers, around 2500professionals, allowit toreacha highpercentageof response, which is essential for successful studies using questionnaires as a tool, as well as being a more homo-geneous sample due tothe participation of professionals fromaroundthecountry,eventhoughthesampledoesnot includeanesthetistswhodonotusuallyattendtheCongress ofAnesthesiology.
Conclusions
The7-itemquestionnaireshowedadequateinternal consis-tency(Cronbach’salphacoefficient>0.7)andawell-defined factorial structure, it can be used as a tool to measure anesthesiologists’ perceptions about the usefulness and applicability of the WHO Safe Surgery Saves Lives check-list. However, although the perceptions captured by the questionnaireareabletodiscriminateamong anesthesiolo-gistswithhighestandlowestpercentageofusechecklistin practice,thescoresresultingfromthequestionnaires can-notpredicttheuseoftheinstrument.Thatis,despitethe moreorlesspositiveperceptionsaboutthechecklist,there isnoassociationbetweentheprobabilityofusingornotthe instrumentinpractice.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Organizac¸ão Mundial da Saúde. Segundo desafio global para a seguranc¸a do paciente: Cirurgias seguras salvam vidas (orientac¸ões para cirurgia segura da OMS). Rio de Janeiro: Organizac¸ão Pan-Americana da Saúde, Ministério da Saúde, AgênciaNacionaldeVigilânciaSanitária;2009.
2.MakaryMA,HolzmuellerCG,ThompsonD,etal.Operatingroom briefings:workingonthesamepage.JtCommJQualPatient Saf.2006;32:351---5.
3.ManserT,FosterS,FlinR,etal.Teamcommunicationduring patienthandoverfromtheoperatingroom:morethanfactsand figures.HumFactors.2013;55:138---56.
4.HaynesAB,WeiserTG,BerryWR,etal.Asurgicalsafety check-listtoreducemorbidityandmortalityinaglobalpopulation.N EnglJMed.2009;360:491---9.
5.Joint Commission International. https://manual. jointcommission.org/Manual/WebHome[accessed02.08.14]. 6.Handler SM, Castle NG, Studentski AS, et al. Patient safety
cultureassessmentinthenursinghome.QualSafHealthCare. 2006;15:400---4.
7.WolfleD,LikertR,MarquisDG,etal.Standardsforappraising psychologicalresearch.AmPsychol.1949;4:320---8.
8.HairJF,BlackWC,BabinBJ,etal.AnáliseMultivariadadeDados. 6aed.PortoAlegre:Bookman;2009.
9.Surgical Safety Web Map. http://maps.cga.harvard.edu: 8080/Hospital/[accessed22.09.13].
10.Correa RT. Guia da Organizac¸ão Mundial da Saúde para a seguranc¸a doato anestésico-cirúrgico.Anestesiaem Revista. 2009;2:16---7.
11.Mastracci TM. Whatare the effects ofintroducing theWHO ‘‘surgicalsafetychecklist’’onin-hospitalmortality?JAmColl Surg.2013;217:1151---3.
12.RussSJ.Aqualitativeevaluationofthebarriersandfacilitators towardimplementation oftheWHO surgical safetychecklist acrosshospitalsinEngland:lessonsfromthe‘‘SurgicalChecklist ImplementationProject’’.AnnSurg.2015;261:81---91. 13.World Health Organization. Safe surgery saves lives:
sec-ond global patient safety challenge; 2008. Available at: http://www.who.int/patientsafety/safesurgery/knowledge
base/SSSLBrochurefinalJun08.pdf[accessed13.04.14]. 14.Soria-AledoV.Dificultadesenlaimplantaciondelchecklisten