www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Knowledge
about
cardiovascular
disease
in
Portugal
Nelson
Andrade
a,1,
Elisabete
Alves
a,b,∗,1,
Ana
Rute
Costa
a,
Pedro
Moura-Ferreira
c,
Ana
Azevedo
a,b,
Nuno
Lunet
a,b aEPIUnit-InstitutodeSaúdePública,UniversidadedoPorto,Porto,PortugalbUniversidadedoPorto,FaculdadedeMedicina,DepartamentodeCiênciasdaSaúdePúblicaeForenseseEducac¸ãoMédica,
Porto,Portugal
cInstituteofSocialSciences,UniversityofLisbon,Lisbon,Portugal
Received12September2017;accepted8October2017 Availableonline25July2018
KEYWORDS Cardiovascular disease; Healthinformation management; Healthknowledge; Primaryprevention Abstract
Objectives: Tocharacterizespecificknowledgeoncardiovasculardisease,particularlystroke andmyocardialinfarction(MI),anditsrelationshipwithsociodemographicfactors,health lit-eracyandclinicalhistory,amongthePortuguesepopulation.
Methods:In across-sectional studyconducted in2012, atotalof1624Portuguese-speaking residentsofmainlandPortugal,agedbetween16and79years,wereassessedthrough face-to-faceinterviewsusingastructuredquestionnaire.
Results:Around30%ofparticipantswereunabletoestimatetheriskofMIorstroke.Onaverage, those whoresponded estimatedthat 34.2%and 35.6%of Portuguesewillsuffer astroke or MI,respectively,duringtheirlifetime.‘‘Notsmoking’’(36.8%)anda‘‘healthydiet’’(32.8%) wereidentifiedasthemostimportantbehaviorsforpreventionofcardiovasculardisease,and lessthanhalfoftheparticipantsrespondedthatthemostappropriateoptioninthepresence ofacutecardiovascularsignsorsymptomswastocall theemergencynumber.‘‘Dependence on daily activities’’ (90.7%)and‘‘impaired speech’’(89.8%)were frequently recognized as consequencesofstroke,while‘‘heartfailure’’(86.4%)and‘‘dependenceondailyactivities’’ (85.3%) werethe mostfrequently identifiedconsequences of MI.Overall, participantswith adequatehealthliteracyrevealedmoreappropriatecardiovascularhealth-relatedknowledge. Conclusions: Thereareimportantgapsincardiovascularhealth-relatedknowledgeinthe Por-tuguese population. Health education strategies and practices should be sensitive to the differences in health literacy described herein, in order to improve cardiovascular health knowledgeamongthePortuguesepopulation.
© 2018SociedadePortuguesade Cardiologia.Publishedby ElsevierEspa˜na,S.L.U.Allrights reserved.
∗Correspondingauthor.
E-mailaddress:[email protected](E.Alves). 1 Equallycontributingauthors.
https://doi.org/10.1016/j.repc.2017.10.017
670 N.Andradeetal.
PALAVRAS-CHAVE
Doenc¸as
cardiovasculares; Gestãodainformac¸ão emsaúde;
Conhecimento emsaúde;
Prevenc¸ãoprimária
Conhecimentosobreadoenc¸acardiovascularemPortugal
Resumo
Objetivos: Caracterizar o conhecimento específico sobre a doenc¸a cardiovascular (DCV), nomeadamenteoacidentevascularcerebral(AVC)eoenfarteagudodomiocárdio(EAM),da populac¸ãoportuguesa,deacordocomfatoressociodemográficos,literaciaemsaúdeehistória clínica.
Métodos: Numestudotransversalrealizadoem2012,foramavaliados1624residentesem Por-tugal continental,entre16 e79 anos, através de entrevistaspresenciais comquestionário estruturado.
Resultados: Cercade30%dosparticipantesnãoconseguiramestimaroriscodeAVCeEAM.Em média,osqueresponderamestimaramque34,2%e35,6%dosportuguesessofrerãoumAVCou um EAM durantea suavida, respetivamente.«Não fumar»(36,8%) euma «dietasaudável» (32,8%) foramidentificados como os comportamentos mais importantespara prevenc¸ão da DCV e menos de metade dos participantes respondeu«telefonar para o 112» como opc¸ão correta perante a presenc¸a de sinais ou sintomas de eventos cardiovasculares agudos. A «dependêncianasatividadesdiárias»(90,7%)eas«perturbac¸õesdafala»(89,8%)foram fre-quentementereconhecidascomo consequênciasdeAVC,enquantoa«insuficiênciacardíaca» (86,4%)e«dependêncianasatividadesdiárias»(85,3%)foramasconsequênciasdeEAM iden-tificadas com maiorfrequência. Em geral, participantes comliteracia em saúde adequada revelaramumconhecimentoemsaúdecardiovascularmaisapropriado.
Conclusões:Verificaram-se importantes lacunas noconhecimento específico sobreadoenc¸a cardiovasculardapopulac¸ãoportuguesa.Asestratégiasepráticasdeeducac¸ãoemsaúdedevem sersensíveisàsdiferenc¸asdescritasdeacordocomoníveldeliteraciaemsaúde,deformaa melhoraroconhecimentoemsaúdecardiovasculardapopulac¸ãoportuguesa.
©2018SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Todosos direitosreservados.
Introduction
Cardiovascular disease (CVD) is the main cause of death worldwide and is projected to remain among the most important contributors to mortality up to 2030.1
World-wide,approximately17.3millionpeoplediedfromCVDin
2013,representingnearlyone-thirdoftheoverallnumberof
deathsand45%ofthoseduetonon-communicablediseases.2
Amongthese,8.1milliondeathswereduetocoronaryheart
disease(CHD) and 6.4 million tostroke, which constitute
the leading and third leading causes of disability
world-wide,respectively.2 In Europe,CVD isresponsible for 45%
ofalldeathseachyear, with2.8milliondeathsattributed
to CHD and stroke.3 In Portugal, CVD is the main cause
ofmortality,withstroke andCHDaccountingfor6.1%and
6.0%,respectively, oftotaldisability-adjustedlifeyearsin
2015.4
Despitethehigh burdenofCVD, therehasbeen a
con-siderable decline in mortality in recent decades.5 These
reflect downward trends in exposure to behavioral risk
factors such as smoking, as well as increasing use of
evidence-basedpharmacologicaltreatmentsfor controlof
hypertension and cholesterol levels, and interventional
therapiesandtechniquesforbettermanagementofpatients
in the acute phase.6---9 However, patterns of variation in
mortalityareheterogeneous,5withmanycountries,
includ-ing Portugal, still presenting considerable potential for
further decreases in morbidity and mortality from stroke
and CHD,5,10 through both ‘high-risk’ and ‘population’
strategies.11
Behaviors that increase the risk of CVD are
mod-ulated by individuals’ health-related knowledge and
risk perception,12 and therefore understanding
limita-tions in specific knowledge is essential to develop
strategies aimed at the empowerment of the
popula-tion for self-care and better use of available health
resources.13,14
Wethereforeaimedtocharacterizespecific knowledge
onthefrequency,prevention,controlandconsequencesof
cardiovascular disease,particularlystroke andmyocardial
infarction(MI),anditsrelationshipwithsociodemographic
factors,historyofCVDandhealthliteracy,amongthe
Por-tuguesepopulation.
Methods
Thisanalysisisbasedonacross-sectionalstudyconducted
between January and May 2012, withthe primary
objec-tive of assessing knowledge and health behaviors in a
representativesample ofPortuguese-speaking residentsof
mainlandPortugal,agedbetween16and79years,as
previ-ouslydescribedindetail.15Briefly,astratifiedprobabilistic
sampling procedure was used to select 150 geographical
units, among which a total of 585 starting points were
designated for the selection of households through
stan-dardrandomrouteprocedures.Ineachselectedhousehold,
the resident whose previous birthday was closest to the
date of the interview was invited to participate. A total
of 1624 valid interviews were obtained (response rate:
Face-to-faceinterviewswereconductedtocollectdata
onsociodemographiccharacteristics,clinicalhistory,health
literacyandspecific knowledgeonthefrequency,
preven-tion,controlandconsequencesofCVD.
A personal history of hypertension, stroke or MI was
considered present when participants recalled a medical
diagnosisoftheseconditions.
ToassesstheperceivedriskofstrokeandMI,participants
wereasked‘‘Forevery100Portuguese,howmanywill
suf-ferfrom stroke and how many will suffer fromMI during
theirlives?’’ andthe quantitativeestimates wereusedas
continuousvariablesindataanalysis.
Regarding behaviors for CVD prevention, participants
were asked to select the most important from a list of
different behaviors, namely ‘‘not smoking’’, ‘‘not
drink-ing’’,‘‘healthydiet’’,‘‘regularexercise’’,‘‘regularblood
pressure measurement’’, and ‘‘other behaviors’’, which
includedtheintakeofmultivitamins,regularweighing,
reg-ularblood testsandgeneralcheck-ups. Theproportionof
participantsidentifyingeachbehaviorasthemostimportant
waspresented.
Awarenessofthemostappropriateactioninthepresence
ofan alarmsign or symptomof apotentialcardiovascular
event was obtained through the question ‘‘In the
pres-ence of each of the following symptoms or signs (chest
painorfacialdrooping)statehowtoproceed’’.Theoptions
were‘‘callemergencynumber’’,‘‘gotoemergency
depart-ment’’, ‘‘call Saúde 24 (the national health helpline)’’,
‘‘schedulean appointment withphysician’’, ‘‘goto
phar-macy’’ and ‘‘take a ‘wait and see’ approach’’. Only the
option‘‘callemergencynumber’’wasconsideredcorrect.
To assess knowledge on the potentialconsequences of
CVD,participants wereaskedtoindicatewhethereachof
five options --- ‘‘paralysis’’, ‘‘dependence in daily
activi-ties’’,‘‘impairedspeech’’,‘‘dementia’’and‘‘epilepsy’’
---couldresult fromstroke. Similarly, participantswere also
askedtostatewhethereachoffiveoptions---‘‘angina
pec-toris’’, ‘‘heart failure’’, ‘‘impaired driving’’, ‘‘impaired
sexual activity’’ and ‘‘dependence in daily activities’’
---couldresultfromMI.Inbothquestions,thepossibleanswers
were‘‘yes’’,‘‘no’’,‘‘donotknow’’and‘‘didnotanswer’’
foreachresponsecategoryandfordataanalysisthelatter
twooptionswererecodedas‘‘no’’.
HealthliteracywasassessedusingtheNewestVitalSign
(NVS)instrument.16Thistoolwasdesignedtoassesshealth
literacyskills,specificallyreadingandnumeracyskills.The
number of correct answers was usedto compute a score
rangingfrom0to6(0-1:highlikelihoodoflimitedliteracy
[HLLL], 2-3: possibility of limited literacy and 4-6:
ade-quate literacy [AL]). Participants who reported that they
were unable to read or write were classified as having
HLLL.
Statistical analyses were performed using STATA 11.1
(College Station, TX, 2009). Adjusted mean differences
in the estimated number of people affected by stroke
and MI, according to sociodemographic characteristics,
health literacy and history of CVD (hypertension, stroke
andMI),withrespective95%confidenceintervals(95%CIs),
were computed by multiple linear regression. To
esti-mate the associations between explanatory factors and
health-related knowledge variables, adjusted prevalence
ratios (PRs) and 95% CIs were computed using Poisson
regression.Allmodelswereadjustedforage,gender,
edu-cational level and health literacy. The product of design
and population weights was used for weighting in all
analyses.
ThesurveywasapprovedbytheEthicsCommitteeofthe
UniversityofPorto.
Results
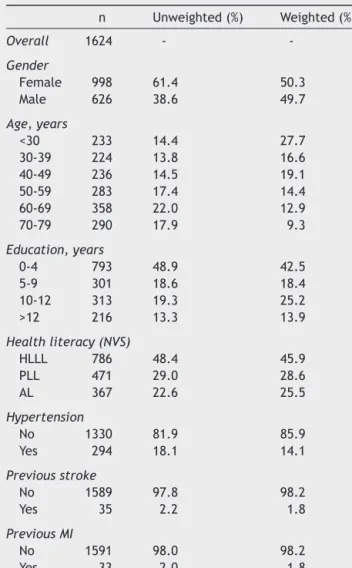
Participantsinoursamplewereevenlydistributedinterms
ofgender.More than 60%were lessthan 50yearsof age,
42.5%hadlessthanfiveyearsofschoolingand45.9%
pre-sentedHLLL(Table1).Apreviousdiagnosisofhypertension
wasreportedby14.1% of participants,and 2.8% reported
priorstrokeorMI(1.8%forstrokeand1.8%forMI).
Nearly 30% of the participants did not answer or did
notknowhowtoanswerthequestionsregardingperceived
riskofstrokeandMI.Theproportionofnon-responseswas
approximatelytwo times higheramong older participants
andnearly40%loweramongthosewithAL.Subjectswitha
previousdiagnosisofstrokewerelesslikelytoestimatethe
lifetimeriskof strokein thepopulation(PR=0.41, 95%CI:
0.21-0.79).Therespondentsstatedthat,onaverage,34.2%
and35.6%ofthePortuguesepopulationwouldsufferastroke
orMI,respectively,duringtheirlifetime(Table2).Therisk
estimates provided by men were approximately8% lower
thanthoseprovided bywomen, andfor stroke those
pro-videdbyparticipants olderthan69were9.6%higherthan
theestimatesbyyoungerparticipants.
Table1 Characteristicsofstudyparticipants.
n Unweighted(%) Weighted(%) Overall 1624 - -Gender Female 998 61.4 50.3 Male 626 38.6 49.7 Age,years <30 233 14.4 27.7 30-39 224 13.8 16.6 40-49 236 14.5 19.1 50-59 283 17.4 14.4 60-69 358 22.0 12.9 70-79 290 17.9 9.3 Education,years 0-4 793 48.9 42.5 5-9 301 18.6 18.4 10-12 313 19.3 25.2 >12 216 13.3 13.9 Healthliteracy(NVS) HLLL 786 48.4 45.9 PLL 471 29.0 28.6 AL 367 22.6 25.5 Hypertension No 1330 81.9 85.9 Yes 294 18.1 14.1 Previousstroke No 1589 97.8 98.2 Yes 35 2.2 1.8 PreviousMI No 1591 98.0 98.2 Yes 33 2.0 1.8
AL:adequateliteracy;HLLL:highlikelihoodoflimitedliteracy; MI:myocardialinfarction;NVS:NewestVitalSign;PLL: possibil-ityoflimitedliteracy.
672 N.Andradeetal.
Figure1 Knowledgeonbehaviors for preventionof cardio-vasculardiseases.
aPercentage ofparticipantsidentifying eachbehaviorasthe
mostimportantforpreventionofcardiovasculardisease. Otherbehaviorsincludedtheintakeofmultivitamins, regular weighing,regularbloodtests,andregulargeneralcheck-ups.
‘‘Not smoking’’ and a ‘‘healthy diet’’ were identified asthe mostimportantbehaviorsfor preventionof cardio-vascular disease by 36.8% and 32.8% of the participants, respectively,while only3.4% reported‘‘checkblood pres-sure’’(Figure1).Nosignificantdifferenceswereobserved
inresponsesconcerningpreventive behaviorsaccording to
sociodemographic characteristics, health literacy or
pre-vious diagnosis of hypertension, stroke or MI, except for
physical exercise,which was less frequently identifiedby
respondentsover69yearsold(PR=0.39,95%CI:0.17-0.89).
Lessthanhalfoftheparticipantsanswered‘‘call
emer-gencynumber’’asthemost appropriateprocedure inthe
presence of facial drooping and chest pain (48.0% and
45.1%,respectively);thiswasindependentlyassociatedwith
greaterlevelsofhealthliteracy(AL:PR=1.44;95%CI:
1.17-1.76 and AL: PR=1.45; 95% CI: 1.17-1.80, respectively, in
comparisonwithHLLL).Amongtheotherparticipants,42.2%
and 39.6% answered ‘‘go to an emergency department’’
whenfacedwithanalarmsignorsymptomofstrokeandMI,
respectively,while1.1%and0.8%wereunabletoanswer.
Data about knowledge on the consequences of stroke
and MI are presented in Figure 2. The most
fre-quently reported consequences were ‘‘dependence in
dailyactivities’’ (90.7%), ‘‘impaired speech’’ (89.8%)and
‘‘paralysis’’(84.3%)forstroke,and‘‘heartfailure’’(86.4%),
‘‘dependenceindailyactivities’’(85.3%),‘‘impaired
driv-ing’’(81.6%)and‘‘anginapectoris’’(81.5%)forMI.
Table 3 presents the distribution of the two most
frequentlyreportedconsequencesofstrokeandMI,
accord-ing to sociodemographic characteristics, health literacy,
and clinical history of the participants. Identification of
‘‘dependenceindailyactivities’’asaconsequenceofstroke
wasmorefrequentamongthosewithadequatehealth
liter-acy (AL vs.HLLL: PR=1.08; 95%CI: 1.01-1.14) andwith a
previous diagnosisofhypertension(PR=1.05; 95%CI:
1.00-1.09), while ‘‘impaired speech’’ was more likely to be
reportedby moreeducated participants(>12 vs. <5years
education:PR=1.10;95%CI:1.00-1.21),thosewithadequate
health literacy (AL vs. HLLL: PR=1.07; 95% CI: 1.02-1.13)
andwithapreviousdiagnosisofMI(PR=1.12;95%CI:
1.06-1.18).RegardingthemainconsequencesofMI,participants
withadequate health literacy (ALvs. HLLL: PR=1.11; 95%
CI:1.04-1.19)andwithapreviousdiagnosisofMI(PR=1.18;
95%CI:1.06-1.31)morefrequentlystated‘‘heartfailure’’,
whilethosewhohadexperiencedstrokeweremorelikelyto
identify‘‘dependenceindailyactivities’’(PR=1.14;95%CI:
1.06-1.22).
Discussion
Thepresentstudyisinnovative,providingacharacterization
of key aspects of health-related knowledge on the
fre-quency,prevention,controlandconsequencesofCVDamong
the Portuguese population. Interpretation of the results
needstotake intoaccountthatgapsinspecificaspectsof
suchknowledgemaybeexpectedtohavedifferentimpacts
oneffortsforpreventionandcontrolofstrokeandMI.
Nearlyonethirdoftheparticipantswereunableto
esti-matethelifetimeriskofMIandstrokeinthepopulation.The
proportionofnon-respondentswashigh,especiallyamong
older participants,takingintoaccountthe highburden of
strokeandMIinthePortuguesepopulation,4theattention
given in the lastdecade tothis subjectin health
promo-tioncampaignsaimedatthegeneralpopulation,17,18andthe
increasingincidenceoftheseconditionswithage.19
Overall, the perceived risk of stroke and MI was
overestimated, with available studies on the Portuguese
population reportingincidenceratesof 207.3/100000and
82.9/100000 population, respectively,20 and prevalence
estimates between 1.6 and 3.2%.21---23 However, it would
probably bedifficult for thegeneral population to
distin-guishbetween thesemeasures, andinformationregarding
theriskofstrokeandMIcomesfrommethodologically
het-erogeneousstudiescarriedoutinpopulationswithdifferent
Paralysis
Dependence in daily activities
Impaired speech Dementia Epilepsy 20 40 60 80 100 Angina pectoris Heart failure Impaired driving Impaired sexual activity
Dependence in daily activities 20 40 60 80 100
Which of the following conditions may affect patients who survive a stroke (%)?a
Which of the following conditions may affect patients who survive myocardial infarction (%)?a
Figure2 Knowledgeofconsequencesofstrokeandmyocardialinfarction.
aPercentageofparticipantsidentifyingeachconditionasapossibleconsequenceaffectingpatientswhosurvivestrokeand myocar-dialinfarction.
nowledge about cardiovascular disease in P ortugal 673
Table2 Perceivedriskofstrokeandmyocardialinfarction,accordingtosociodemographiccharacteristics,healthliteracyandhistoryofcardiovasculardisease. Forevery100Portuguese,howmanywillhavethisdiseaseduringtheirlives?
Stroke Myocardialinfarction
Don’tknow/didnotanswer No.ofpeopleaffected Don’tknow/didnotanswer No.ofpeopleaffected
% PR(95%CI)a Mean (95%CI)a % PR(95%CI)a Mean (95%CI)a
Overall 29.9 — 34.2 — 29.7 — 35.6 —
Gender
Female 29.2 [reference] 38.4 [reference] 30.4 [reference] 40.0 [reference]
Male 30.6 1.09(0.90to1.32) 29.8 −8.26(−11.37to−5.15) 29.0 0.98(0.80to1.21) 31.3 −8.13(−11.44to−4.83)
Age(years)
<30 20.3 [reference] 31.6 [reference] 19.3 [reference] 33.4 [reference]
30-39 19.5 0.95(0.60to1.51) 33.9 2.73(−2.78to8.24) 20.1 1.01(0.63to1.63) 36.5 3.68(−2.13to9.50) 40-49 37.4 1.67(1.11to2.52) 35.2 3.07(−2.40to8.54) 37.8 1.73(1.14to2.63) 36.2 2.29(−3.64to8.22) 50-59 30.6 1.33(0.89to1.99) 35.4 2.92(−2.59to8.44) 33.7 1.48(0.99to2.21) 36.9 2.52(−3.94to8.98) 60-69 34.0 1.47(0.97to2.22) 34.7 1.69(−5.31to8.68) 32.1 1.40(0.92to2.12) 34.5 −1.19(−8.85to6.47) 70-79 55.5 2.27(1.49to3.46) 41.4 9.59(0.91to18.26) 51.7 2.09(1.36to3.22) 42.2 8.43(−0.60to17.46) Education(years)
<5 36.9 [reference] 35.3 [reference] 36.9 [reference] 37.0 [reference]
5-9 33.5 1.21(0.91to1.62) 34.8 1.67(−3.80to7.14) 34.1 1.19(0.90to1.58) 34.9 −2.24(−8.14to3.66)
10-12 21.5 0.91(0.63to1.32) 31.8 −1.10(−7.27to5.07) 20.9 0.86(0.59to1.25) 33.9 −3.24(−10.22to3.75)
>12 19.6 0.90(0.59to1.40) 34.3 1.61(−5.04to8.25) 17.9 0.77(0.49to1.22) 35.6 −1.93(−9.33to5.48)
Healthliteracy(NVS)
HLLL 37.7 [reference] 34.6 [reference] 37.5 [reference] 34.2 [reference]
PLL 28.3 0.87(0.68to1.11) 36.3 1.83(−2.42to6.08) 26.9 0.82(0.64to1.06) 39.6 6.19(1.70to10.68)
AL 17.8 0.61(0.42to0.87) 31.5 −1.92(−6.60to2.75) 18.8 0.66(0.48to0.91) 33.6 1.34(−3.62to6.31)
Hypertension
No 27.9 [reference] 33.6 [reference] 27.6 [reference] 35.2 [reference]
Yes 42.1 1.11(0.87to1.42) 38.8 1.69(−2.68to6.06) 42.6 1.14(0.88to1.48) 39.2 1.02(−3.54to5.57)
Previousstroke
No 30.2 [reference] 34.1 [reference] 29.7 [reference] 35.6 [reference]
Yes 17.4 0.41(0.22to0.79) 36.3 0.95(−6.16to8.06) 29.5 0.71(0.30to1.67) 36.0 0.82(−8.13to9.76)
PreviousMI
No 29.8 [reference] 34.1 [reference] 29.6 [reference] 35.5 [reference]
Yes 38.2 0.83(0.39to1.77) 40.4 5.77(−5.41to16.95) 34.9 0.79(0.35to1.75) 39.9 3.80(−6.11to13.71)
AL:adequateliteracy;CI:confidenceinterval;HLLL:highlikelihoodoflimitedliteracy;MI:myocardialinfarction;NVS:NewestVitalSign;PLL:possibilityoflimitedliteracy;PR:prevalence ratio.
674
N.
Andrade
et
al.
Table3 Thetwomostfrequentlyreportedconsequencesofstrokeandmyocardialinfarction,accordingtosociodemographiccharacteristics,healthliteracyandhistoryof cardiovasculardisease.
Consequencesofstroke ConsequencesofMI
Dependenceindailyactivities Impairedspeech Heartfailure Dependenceindailyactivities
% PR(95%CI)a % PR(95%CI)a % PR(95%CI)a % PR(95%CI)a
Gender
Women 92.1 [reference] 88.4 [reference] 86.2 [reference] 85.7 [reference]
Men 89.2 0.97(0.93to1.01) 91.2 1.03(0.98to1.08) 86.6 1.00(0.93to1.07) 85.0 0.99(0.94to1.04)
Age(years)
<30 92.3 [reference] 88.4 [reference] 87.7 [reference] 85.6 [reference]
30-39 87.1 0.94(0.87to1.02) 90.7 1.02(0.95to1.10) 87.2 0.99(0.90to1.09) 83.5 0.98(0.89to1.08) 40-49 88.5 0.98(0.89to1.08) 93.7 1.09(1.00to1.18) 89.2 1.04(0.94to1.15) 86.0 1.02(0.92to1.12) 50-59 95.0 1.07(0.99to1.15) 90.5 1.06(0.97to1.16) 90.6 1.07(0.99to1.15) 90.7 1.07(0.98to1.17) 60-69 90.9 1.05(0.95to1.16) 90.0 1.08(0.97to1.20) 86.1 1.04(0.94to1.15) 84.9 1.01(0.90to1.14) 70-79 89.3 1.04(0.93to1.16) 83.1 1.01(0.89to1.13) 69.6 0.85(0.72to1.01) 78.9 0.94(0.80to1.10) Education(years)
<5 88.4 [reference] 87.2 [reference] 82.6 [reference] 85.0 [reference]
5-9 91.7 1.05(0.96to1.16) 92.1 1.05(0.97to1.14) 89.8 1.05(0.97to1.13) 84.1 0.98(0.89to1.07)
10-12 91.8 1.05(0.94to1.17) 89.0 1.03(0.93to1.14) 88.8 1.03(0.94to1.14) 87.3 1.02(0.93to1.12)
>12 94.6 1.07(0.96to1.19) 96.8 1.10(1.00to1.21) 90.1 1.03(0.94to1.13) 85.4 0.99(0.89to1.10)
Healthliteracy(NVS)
HLLL 87.6 [reference] 87.3 [reference] 81.8 [reference] 83.9 [reference]
PLL 91.7 1.04(0.98to1.10) 88.6 1.00(0.94to1.07) 87.4 1.03(0.97to1.10) 85.4 1.00(0.93to1.08)
AL 94.8 1.08(1.01to1.14) 95.7 1.07(1.02to1.13) 93.5 1.11(1.04to1.19) 87.9 1.04(0.97to1.12)
Hypertension
No 90.2 [reference] 89.8 [reference] 86.9 [reference] 85.4 [reference]
Yes 93.4 1.05(1.00to1.09) 89.7 1.03(0.98to1.08) 83.7 1.01(0.93to1.10) 85.3 1.01(0.92to1.11)
Previousstroke
No 90.6 [reference] 89.7 [reference] 86.3 [reference] 85.1 [reference]
Yes 94.4 1.04(0.95to1.15) 95.4 1.08(0.98to1.19) 91.0 1.09(0.96to1.24) 97.0 1.14(1.06to1.22)
PreviousMI
No 90.6 [reference] 89.7 [reference] 86.3 [reference] 85.6 [reference]
Yes 93.7 1.06(0.97to1.16) 97.6 1.12(1.06to1.18) 93.7 1.18(1.06to1.31) 74.3 0.89(0.60to1.31)
AL:adequateliteracy;CI:confidenceinterval;HLLL:highlikelihoodoflimitedliteracy;MI:myocardialinfarction;NVS:NewestVitalSign;PLL:possibilityoflimitedliteracy;PR:prevalence ratio.
characteristics. It is estimated that stroke will affect at
leastoneinsixmiddle-agedpeopleduringtherestoftheir
lives.24,25Althoughsimilarestimatesarepresentedformen
regarding MI, the risk is lower for women, with
approxi-matelyoneinninemiddle-agedwomensufferingMIintheir
remaininglifetime.26DespitethehigherprevalenceofCVD
amongmen,3inourstudywomenreportedahigher
percep-tionofrisk,asobservedinpreviousstudies.27,28Also,older
participants tendedto havehigher risk perception,which
maybe duetomore frequent provision ofinformationby
thehealthcaresystemaboutstrokeandMI,sincetheyare
atgreaterriskofdisease.19
Prevention andcontrolofthemain modifiableCVDrisk
factors, suchassmoking, alcohol consumption, unhealthy
diet,obesity,hypertension,dyslipidemia,diabetes,
psycho-logical stress and a sedentary lifestyle, are fundamental
tools to reduce the burden of stroke and CHD.29,30
Parti-cipants identified not smoking and a healthy diet as the
mainpreventivebehaviorsforCVD,althoughtheyattributed
lower importance to blood pressure control, despite the
highprevalenceofhypertensioninthecountry.22However,
since participants were asked to select the most
impor-tant froma list of different behaviors, it is possible that
theyassumedhighbloodpressurewouldbeaconsequence
of unhealthylifestyles. Recent guidelinesonCVD
preven-tion in clinical practice suggest that cognitive-behavioral
methods are effective in helping individuals to adopt a
healthylifestyle,emphasizingtheimplementationof
nutri-tion,exercise,relaxationtraining,weightmanagementand
smokingcessationprograms.31Thiscallsforappropriateand
effectivecommunicationbetweenpatientsandhealth
pro-fessionals,whichwillfacilitatetreatmentandpreventionof
CVD.
In Portugal, in the presence of signsand/or symptoms
suspiciousofstroke orMI,thecorrectprocedureistocall
theemergencynumber.32Althoughlessthanhalfofthe
par-ticipants surveyed selectedthis option inthe presenceof
facialdroopingorchestpain,approximately40%indicated
thattheywouldgodirectlytotheemergencydepartment,
whichisalsoavalidprocedure.Theresultspresentedarein
agreementwithpreviousPortuguesestudies,whichrevealed
thatonlybetween22.4%and68.0%ofrespondentswouldcall
theemergencynumberwhen facedwitha possiblestroke
orMI.33---35 Theselowpercentagesmaybeduetotwomain
factors:lackofawarenessoftheimportanceofcallingthe
emergencynumber,thusactivatingfast-trackprotocols,or
theinabilitytolinkthesesignsandsymptomstoeventssuch
asstrokeorMI.OnestudyconductedinPortugalshowedthat
24%of respondentsdid notrecognizethe signsand
symp-tomsofMI.33Nevertheless,inourpopulation,thelikelihood
of taking appropriate action, i.e., calling the emergency
number in the presence of facial droopingor chest pain,
increasedwithhealthliteracy,whichhighlightstheneedto
improvehealth literacyand cardiovasculardisease
knowl-edgeinthePortuguesepopulation.
As aconsequenceofdownwardtrendsin mortality,the
number of survivors from CHD and stroke is increasing,
which in turn has led to a greater number of
individ-uals suffering from sequelae.36 There is a wide range
of outcomes after a CVD event, from no sequelae to a
comatose state, with considerable personal, emotional,
professional and financial costs to both individuals and
health services.37 Although dependence in daily
activi-ties was frequently recognized as a major outcome of
stroke and MI, this sequela is in fact more prevalent in
stroke.38 This finding may be a consequence of the
diffi-culty among the general population of differentiating MI
and stroke. Other potential consequences of stroke, such
asepilepsyand dementia,were less frequently reported,
possiblybecausetheymaybeperceived aslesssevere, or
ashaving other causes. However, previous studies reveal
that stroke almost doubles the risk of dementia after
the age of 65,39 and is the leading cause of seizures
and epilepsy in the elderly.40 Thus, the dissemination
of more comprehensive information regarding the global
burden of CVD is essential among the general
popula-tion.
Overall,respondentswithALweremorelikelytoanswer
thequestionsandtoprovidecorrectresponsesthanthose
with HLLL. However, a recent study reported that 49%
of Portuguese respondents have limited health literacy,41
highlighting the need to assess citizens’ health-related
knowledgewhenplanningcardiovascularpolicystrategies.
Thisstudy addresseda topicrarely investigatedin
Por-tugal --- knowledge of CVD --- based on a representative
sample of Portuguese-speakingresidents of mainland
Por-tugal.However,somelimitationsshouldbeacknowledged.
Healthliteracywasmeasuredusinganinstrumentdesigned
to assess overall health literacy skills42 that is not
spe-cifictocardiovascularhealth-relatedknowledge.Thus,the
instrumentmaynotbesufficientlysensitivetoassesshealth
literacy concerning CVD specifically, given its particular
characteristics.DataontheconsequencesofstrokeandMI
wereobtained from recognition of possible consequences
in a list, which could lead to overestimation of
knowl-edgeinthisdomain.It hasbeenshown thatclosed-ended
questionsingeneralyield higherpercentages ofresponses
thanopen-endedquestions,43 andthelowerproportionof
non-respondentsinthesequestionsappearstosupportthis
assumption. However, taking into account that the main
consequencesofstrokeandMIwereconsidered,significant
overestimationisunlikely.
Conclusion
EffectivepreventionandcontrolofCVDriskfactorsaswell
astherecognitionofsigns,symptoms,andwhattodowhen
facedwith alarm signs of an acute event44 are essential
to reduce the burden of CVD. In the present study, the
largeproportionof non-respondentstoquestions
address-inghealth-relatedknowledge onstrokeandMI, which are
common conditions in Portugal, as well as participants’
lack of knowledge about vital aspects of these diseases,
highlighttheexistenceofimportantgapsincardiovascular
health-related knowledge. However, it was also observed
that individuals with adequate health literacy responded
more often and more appropriately than those with
lim-itedliteracy,indicatingthathealtheducationstrategiesand
practicesshouldbesensitive tothesedifferencesin order
toimprovecardiovascularhealthknowledgeamongthe
Por-tuguesepopulation.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Acknowledgments
This study was funded by through the Operational
Pro-gramCompetitivenessandInternationalizationandnational
funding from the, under the project ‘Health information
ofPortuguese population: Knowledge andperceived
qual-ity and accessibility of health information sources’ (ref.
676 N.Andradeetal.
Investigac¸ãoemEpidemiologia---InstitutodeSaúdePública daUniversidade do Porto (EPIUnit)
(POCI-01-0145-FEDER-006862;ref. UID/DTP/04750/2013);the PostdocGrant (to
EA)andthePhDgrant(toARC)wereco-fundedbytheand
ProgramaOperacionalCapitalHumano(POCH/FSE).
TheEnglishversionoftheNVSwasdevelopedbyPfizer
Inc.PfizerInc.grantedauthorizationforthetranslationand
assessmentof the psychometric propertiesof NVSfor the
Portugueselanguageintheadultpopulation(aged18to64
years).
References
1.Mendis S,PuskaP,NorrvingB.Globalatlasoncardiovascular diseasepreventionandcontrol.Geneva:WorldHealth Organi-zation(WHO);2011.
2.GBD2013MortalityandCausesofDeathCollaborators.Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematicanalysisfortheGlobalBurdenofDiseaseStudy2013. Lancet.2015;385:117---71.
3.TownsendN,WilsonL,BhatnagarP,etal.Cardiovascular dis-ease in Europe: epidemiological update 2016. Eur Heart J. 2016;37:3232---45.
4.WilkinsE,WilsonL, Wickramasinghe K,et al.European Car-diovascular DiseaseStatistics2017. Brussels:EuropeanHeart Network;2017.
5.Araujo F, Gouvinhas C,Fontes F,et al. Trends in cardiovas-culardiseasesandcancermortalityin45countriesfromfive continents(1980-2010).EurJPrevCardiol.2014;21:1004---17. 6.UnalB,CritchleyJ,CapewellS.Explainingthedeclinein
coro-naryheartdiseasemortalityinEnglandandWalesbetween1981 and2000.Circulation.2004:1101---7.
7.PereiraM,AzevedoA,LunetN,etal.Explainingthedeclinein coronaryheartdiseasemortalityinPortugalbetween1995and 2008.CircCardiovascQualOutcomes.2013;6:634---42. 8.FordES,AjaniUA,CroftJB,etal.Explainingthedecreasein
U.S.deathsfromcoronarydisease,1980-2000.NEngl JMed. 2007;356:2388---98.
9.LacklandDT,RoccellaEJ,DeutschAF,etal.Factorsinfluencing thedeclineinstroke mortality:astatementfrom the Amer-ican Heart Association/American Stroke Association. Stroke. 2014;45:315---53.
10.PereiraM, CarreiraH, ValesC,etal. Trendsinhypertension prevalence(1990-2005)andmeanbloodpressure(1975-2005) inPortugal:asystematicreview.BloodPress.2012;21:220---6. 11.RoseG.Thestrategyofpreventivemedicine.OxfordUniversity
Press;1994.
12.Safeer RS, CookeCE, KeenanJ. The impact ofhealth liter-acyoncardiovasculardisease.VascHealthRiskManag.2006;2: 457---64.
13.VaidyaA,AryalUR,KrettekA.Cardiovascularhealthknowledge, attitudeandpractice/behaviourinanurbanisingcommunityof Nepal:apopulation-basedcross-sectionalstudyfrom Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ Open. 2013;3:e002976.
14.Nielsen-BohlmanL,PanzerA,HamlinB,etal.Healthliteracy:a prescriptiontoendconfusion.Washington:NationalAcademies Press;2004.
15.CostaAR,SilvaS,Moura-FerreiraP,etal.Cancerscreeningin Portugal:sexdifferencesinprevalence,awarenessoforganized programmesand perception ofbenefitsand adverseeffects. HealthExpect.2017;20:211---20.
16.Weiss BD, MaysMZ, MartzW, et al.Quick assessmentof lit-eracy inprimary care: thenewest vitalsign. AnnFam Med. 2005;3:514---22.
17.Direcc¸ão Geral de Saúde (DGS). Programa Nacional de Prevenc¸ão eControlo das Doenc¸as Cardiovasculares. Lisboa: Direc¸ãoGeraldaSaúde;2006.
18.Direcc¸ão Geral de Saúde (DGS). Programa Nacional de Prevenc¸ãoeControlodasDoenc¸as Cérebro-Cardiovasculares. Lisboa:Direc¸ãoGeraldaSaúde;2011.
19.WorldHealthOrganization.Global healthrisks:mortalityand burdenofdiseaseattributabletoselectedmajorrisks.Geneva: WHO;2009.
20.RodriguesA,SilvaS,BatistaI,etal.Médicos-Sentinela:oquese fezem2012.Lisboa:InstitutoNacionaldeSaúdeRicardoJorge; 2014.
21.FiuzaM,Cortez-DiasN,MartinsS,etal.Metabolicsyndrome in Portugal: prevalence and implications for cardiovascu-lar risk --- results from the VALSIM Study. Rev Port Cardiol. 2008;27:1495---529.
22.Polonia J, Martins L, Pinto F,et al. Prevalence, awareness, treatmentandcontrolofhypertensionandsaltintakein Por-tugal:changesoveradecade.ThePHYSAstudy.JHypertens. 2014;32:1211---21.
23.Sousa-UvaM,DiasCM.PrevalênciadeAcidenteVascular Cere-bralnapopulac¸ãoportuguesa:dadosda amostraECOS2013. InstitutoNacionaldeSaúdeDoutorRicardoJorge;2014. 24.SeshadriS, BeiserA, Kelly-Hayes M,et al. The lifetime risk
of stroke: estimates from the Framingham Study. Stroke. 2006;37:345---50.
25.TurinTC,OkamuraT,AfzalAR,etal.Hypertensionandlifetime riskofstroke.JHypertens.2016;34:116---22.
26.TurinTC,KokuboY,MurakamiY,et al.Lifetimeriskofacute myocardialinfarctioninJapan.CircCardiovascQualOutcomes. 2010;3:701---3.
27.Homko CJ, Santamore WP, Zamora L, et al. Cardiovascular diseaseknowledgeandriskperceptionamongunderserved indi-vidualsatincreasedriskofcardiovasculardisease.JCardiovasc Nurs.2008;23:332---7.
28.HomkoCJ,ZamoraL,SantamoreWP,etal.Genderdifferences incardiovascularriskfactorsandriskperceptionamong indi-vidualswithdiabetes.DiabetesEduc.2010;36:483---8. 29.O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for
ischaemicandintracerebral haemorrhagicstrokein22 coun-tries(the INTERSTROKEstudy): acase-control study.Lancet. 2010;376:112---23.
30.YusufS,HawkenS,OunpuuS,etal.Effectofpotentially mod-ifiableriskfactorsassociatedwithmyocardialinfarctionin52 countries(theINTERHEARTstudy):case-controlstudy.Lancet. 2004;364:937---52.
31.PiepoliMF,HoesAW,AgewallS,et al.2016European Guide-linesoncardiovasculardiseasepreventioninclinicalpractice: theSixthJointTaskForceoftheEuropeanSocietyof Cardiol-ogyandOtherSocietiesonCardiovascularDiseasePrevention inClinicalPractice(constitutedbyrepresentativesof10 soci-eties and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37: 2315---81.
32.Alto Comissariado da Saúde --- Coordenac¸ão Nacional para asDoenc¸asCardiovasculares. Recomendac¸õesClínicasparao EnfarteAgudodo Miocárdioe o Acidente VascularCerebral; 2007.Lisboa.
33.PereiraH,PintoFJ,CaleR,etal.StentforLifeinPortugal:this initiativeisheretostay.RevPortCardiol.2014;33:363---70. 34.Branco MJ, Nunes B. Sinais de Alarme de Enfarte Agudo
do Miocárdioe Acidente Vascular Cerebral: uma observac¸ão sobreconhecimentos eatitudes. InstitutoNacional deSaúde Dr.RicardoJorge;2008.
35.MansurKF.OquesabeocidadãosobreoAcidenteVascular Cere-bral:Inquéritonumapopulac¸ãourbana.Instituto deCiências BiomédicasdeAbelSalazar,UniversidadedoPorto;2009.
36.LeviF, Chatenoud L, Bertuccio P, et al. Mortality from car-diovascularandcerebrovasculardiseasesinEuropeandother areasoftheworld:anupdate.EurJCardiovascPrevRehabil. 2009;16:333---50.
37.SchofieldD, ShresthaR, Percival R, et al. Thepersonal and nationalcostsofCVD:impactsonincome,taxes,government supportpaymentsandGDPduetolostlabourforce participa-tion.IntJCardiol.2013;166:68---71.
38.GrimbyG,AndrenE,DavingY,etal.Dependenceandperceived difficultyindailyactivitiesincommunity-livingstrokesurvivors 2yearsafterstroke:astudyofinstrumentalstructures.Stroke. 1998;29:1843---9.
39.PendleburyST, RothwellPM.Prevalence,incidence,and fac-tors associated with pre-stroke and post-stroke dementia: asystematicreviewandmeta-analysis.LancetNeurol.2009;8: 1006---18.
40.JungehulsingGJ,HeuschmannPU,HoltkampM,etal.Incidence and predictors of post-stroke epilepsy. Acta Neurol Scand. 2013;127:427---30.
41.EspanhaR,Ávila P,MendesR. Literaciaem Saúdeem Portu-gal:RelatórioSíntese.Lisboa:Fundac¸ãoCalousteGulbenkian; 2016.
42.Welch VL, VanGeest JB, CaskeyR. Time,costs, and clinical utilizationofscreeningforhealthliteracy:acasestudyusing theNewestVitalSign(NVS)instrument.JAmBoardFamMed. 2011;24:281---9.
43.RejaU,LozarManfredaK,HlebecV,etal.Open-endedvs. close-ended questions in Web questionnaires. Adv Methodol Stat. 2003;19:159---77.
44.World Health Organization. Milestones in health promotion. Statementsfromglobalconferences.Geneva:WHOPress;2009.