revbrashematolhemoter.2017;39(4):375–378
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Role
of
daratumumab
in
transfusion
medicine:
a
must
know
entity
Rajeswari
Subramaniyan
a,∗,
Ramaprabahari
Satheshkumar
a,
Karishma
Rosann
Pereira
baKovaiMedicalCenterandHospital,Coimbatore,India
bYashodaHospital,Hyderabad,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received25April2017 Accepted11July2017 Availableonline8August2017
Introduction
Druginterferenceinserologicalassaysisawell-known phe-nomenon.Therapeuticmonoclonalantibodies(MoAbs)have beensuccessfulintreatingavarietyofmalignancies.Some of these MoAbs interfere in day-to-day laboratory tests. Recently, a novel targeted immunotherapy, daratumumab (MoAb against CD38 antigen) was approved for treating advancedstagemultiplemyeloma(MM).1Herein,wedescribe theinterferenceofdaratumumabintheredbloodcell(RBC) compatibilitytestingofapatientwithrefractoryrelapsedMM.
Case
description
A 72-year-old gentleman previously diagnosed with immunoglobulin (Ig)A MM presented with complaints ofpaininboththehipjointsforthreeweeks.Hematological parameters at the time of admission were: hemoglobin 6.8g/dL, platelet count: 95×109/L; total leukocyte count:
∗ Correspondingauthorat:DepartmentofTransfusionMedicine,KovaiMedicalCenterandHospital,AvinashiRoad,Coimbatore641014,
India.Tel.:+9104224324817.
E-mailaddress:[email protected](R.Subramaniyan).
2.7×103/L. Magnetic resonance imaging (MRI) showed spinalcordcompressionatL4-L5level.Onthesecondweek of admission, wereceived a request foroneRBC unit. His blood grouping was BRhD positive. Initially, oneRBC unit was incompatible inthe anti-humanglobulin (AHG) phase usingaLISS/Coombsgelcard(Biorad,Cressier,Switzerland). Immediatespin(IS)crossmatchusingthetubetechniquewas compatible.Adirectantiglobulintest(DAT)ofthepatientwas negativeforIgGandC3dusingmonospecificCoombsgelcard (Biorad,Cressier,Switzerland). Subsequently,weperformed an indirect antiglobulin test (IAT) using LISS/Coombs gel cardwithcommercialthreecellpanel,DiaCellI-II-III(Biorad, Cressier,Switzerland)whichwaspanreactive(2+)whilethe auto controlwas negative.RBC antibodyidentification was panreactive (2+) using the ID-Diapanel (Biorad, Cressier, Switzerland). We suspected multiple alloantibodies or an antibodytoahigh-prevalenceantigen.Extendedphenotyping could not be done asthe previous transfusion waswithin threemonths.RBCantibodyidentificationwasrepeatedusing apapaintreated11-cellpanel(singlestageassay).However, novariationinthegradeofagglutinationwasobserved.Acid
http://dx.doi.org/10.1016/j.bjhh.2017.07.002
376
revbrashematolhemoter.2017;39(4):375–378elutionwas performed using the commercial kit (Diacidel, Biorad, Cressier, Switzerland) and the IAT of the eluate wasnegative.WefurtherperformedAHGcrossmatchwith18 groupspecificRBCunitsandallwereincompatible.Previously, thepatienthadbeentransfusedondifferentoccasionsatour centerwithfivegroupspecificpackedRBCs(AHGcompatible) dueto anemia. Wereviewedhiscompatibility profileprior tothefirsttransfusion.HisbloodgroupwasBRhDpositive, whilehisDAT andIATwerenegative.Retrospective exami-nationofhistreatmentrecordsrevealedthatthepatienthad receivedonecycleofdaratumumab(dose:16mg/kg–1200mg) three days before the crossmatching was requested. Since theRBCunitswereAHGcompatiblepriortotheinitiationof daratumumab,wesuspectedthatdaratumumabinterferedin pretransfusiontesting.
Dithiothreitol (DTT) treatment of the reagent RBCs has beenshowntoeliminatetheeffectsofdaratumumab.So,we attempted crossmatching withDTT treated donorRBCs as describedbyChapuyetal.2DTT(0.2M)waspreparedby dis-solving1gofDTTin32mLofphosphatebufferedsaline(PBS) atpH 8.0.Two K-negative RBC units were taken for cross-matching.K+andE+RBCswereusedascontrols.Donorcells
andcontrolcellswerewashedwithPBS(pH7.3)fourtimes. Aquantityof400LDTTatpH8.0wasaddedto100L(5% suspension)ofRBCs.Themixturewasincubatedat37◦Cfor
30min.Followingincubation,thecellswerewashedwithPBS (pH7.3)fourtimes.A0.8%suspensionwaspreparedwithPBS (pH7.3)andthecrossmatchwasrepeatedonaLISS/Coombs gelcard.AfterDTTtreatment,thetwoRBCunitswere AHG-compatible.IATwasnegativewithDTT-treatedreagentRBCs. ThepatientwastransfusedwithonecompatibleRBCunitand notransfusionreactionwasobserved.Post-transfusion,the patient’shemoglobinlevelimprovedto7.6g/dL.
Discussion
Daratumumab is the first-in-class human IgG1 anti-CD38 MoAb approved by the FDA in 2015 for the treatment of patientswithMMwhoaredoublerefractoryto immunomod-ulatorydrugs(IMiDs)and proteasomeinhibitors(PIs).CD38 isa transmembrane glycoprotein which is involvedin cell adhesionandsignaltransductioninavarietyofcells.Itplays akey role inintracellularcalcium mobilization throughits enzymaticactivity.Itisnormallyexpressedatlowlevelson precursor and activatedTand Bcells,myeloid cells, natu-ralkillercells,RBCs,plateletsandplasmacells.Itisstrongly expressedonmyelomacells,afactwhichunderliesthe treat-mentofMMwithtargetedimmunotherapy.1FalsepositiveIAT resultswerefirstobservedinpatientsreceivingdaratumumab duringphaseIandIIclinicaltrials.3However,thedrugdoes notaffect thepatient’sABO bloodgroupingand immediate spincrossmatch.ItbindstoendogenousCD38onRBCs.Such sensitizedRBCsagglutinateintheCoombsphaseresultingin panreactivityinvitro(DAT,antibodyscreening/identification, crossmatching).4
Routine serological methods are ineffective in circum-venting the interference in compatibility testing, thereby resulting in an unexpecteddelay infinding suitable blood forthesepatients.Also,itmaymasktheunderlying
alloan-tibodies,mimickingahightiterantibodyoranantibodytoa high-prevalenceantigenasdescribedinourcase.5Anti-CD38 canbindtothepatient’sownRBCscausingpositiveDAT.In ourcase,theDAT wasnegativewhichprobablywasdueto clearance ofdrug-coatedRBCs inthespleenbyFc-receptor mediateduptake.Daratumumabinfusionhasbeenrelatedto clinicallyinsignificantanemia.6 Sofar,afterthedrug’s infu-sion,notransfusion-relatedhemolysishasbeenobservedin severalclinicaltrialsheldworldwide.5Afterstarting daratu-mumabinourpatient,drugrelatedanemiawasnotobserved. Several strategies have been proposed to eliminate the drug’s interference. Provision ofblood forsuch patients is feasible by1.ThioltreatedRBCs forpretransfusiontesting; 2. serologic phenotyping of patients and antigen-matched transfusions; 3. Genotyping and antigen-matched transfu-sions; 4.antibodyscreeningwithcordblood 5.neutralizing theantibodywithsolubleCD38oranti-daratumumaband6. acombinationofthesetechniques.7
Genotypingismoreaccurateandcomprehensivein pro-viding extended antigen profile of RBCs than serologic phenotyping. It can be carried out in patients even after the initiation of daratumumab. This method is expensive, not readily available and challenging formany centers for want of an antigen-matched inventory. As per previous reports, many centers perhaps prefer the DTT-based tech-nique thanks to its easy availability in blood banks. CD38 hassixdisulfidebondsinitsextracellulardomainwhichare disruptedbyDTTandotherreagents (2-mercaptoethanol/2-aminoethylisothiouronium).Veryfewcentershavereported the use of the other thiol reagents.2 Our center is a ter-tiary care hospital and a transplant center (bone marrow and solid-organ transplant). However, welack facilitiesfor antigengenotyping.WeroutinelyuseDTTforABOantibody titers. Hence, we preferred DTT-based pretransfusion test-ing to negatethe drug’s interference.SinceDTT denatures Kell antigens, K-negativeRBC units shouldbeprovidedfor suchpatientsunlessthepatientisK-positive.However,this is not without disadvantages. Firstly, it is time-consuming (averagetimetakentoresolvetheinterferenceinapatient withnoantibodyandwithonealloantibodywas2hand4h, respectively).Secondly,underlyingantibodiesagainstK,DO, IN,JMH,KN,LWantigenswouldnotbedetected,asthese anti-gensaredestroyedbyDTT.Nevertheless,thissituationisvery rare.2
revbrashematolhemoter.2017;39(4):375–378
377
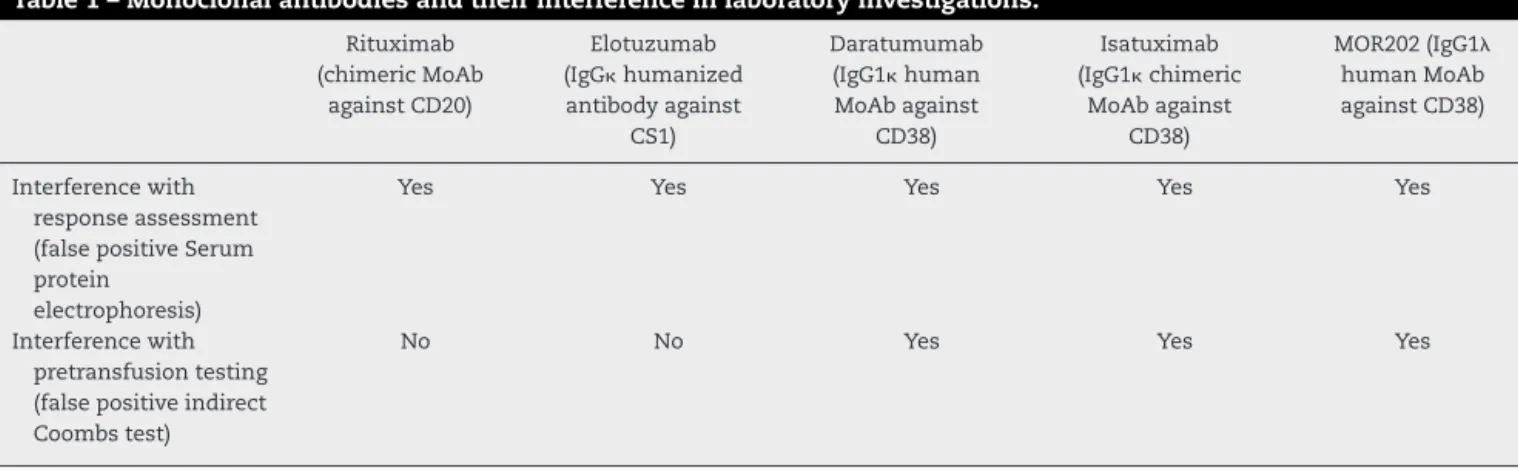
Table1–Monoclonalantibodiesandtheirinterferenceinlaboratoryinvestigations.
Rituximab (chimericMoAb
againstCD20)
Elotuzumab (IgGhumanized antibodyagainst
CS1)
Daratumumab (IgG1human MoAbagainst
CD38)
Isatuximab (IgG1chimeric
MoAbagainst CD38)
MOR202(IgG1
humanMoAb againstCD38)
Interferencewith responseassessment (falsepositiveSerum protein
electrophoresis)
Yes Yes Yes Yes Yes
Interferencewith pretransfusiontesting (falsepositiveindirect Coombstest)
No No Yes Yes Yes
cost ofthiol-based antibody investigations withinfive and 21 transfusion events, respectively. In contrast, for more thansixantigen-matchedtransfusions,thiol-basedantibody investigationwaseconomical.7
Otherapproacheshavelimitedroleinmanycentersowing totheirlimitedavailability,high-costandlackof standardiza-tion.Thedrug’seffectisthoughttopersistforsixmonthsafter initiation.1 Inthispatient, forfuturetransfusions,antibody screeningwould be repeated withDTT-treated cells.If the antibodyscreeningisnegative,thepatientwillbeprovidedK−,
ABO/DcompatibleRBCsbyIATcrossmatchusingDTTtreated donorRBCs.Iftheantibodyscreeningispositive,DTT-antibody identificationwillbeperformed.Antigennegativeunitswould beprovidedbyIATcrossmatchusingDTTtreateddonorRBCs.8 Also,wehaveprovidedthepatientwithaninformationcard indicatinghistreatmentwithdaratumumab.
Otheranti-CD38MoAbscurrentlyunderinvestigationsuch as chimeric IgG MoAb isatuximab (SAR650984) and IgG1
MoAbMOR202are alsoexpectedtocausefalsepositiveIAT resultsduetotheirclasseffect(Table1).1Anti-CD44MoAbs are also thought to interfere with pretransfusion testing.9 Daratumumab, similar to rituximab, is also implicated in falsepositive results inserum proteinelectrophoresis and immunofixationelectrophoresis,therebyaffectingthe mon-itoringofcompleteresponseinpatientswithIgG1myeloma. Flowcytometricassessmentofnormalandneoplasticplasma cells is also hampered following the initiation of daratu-mumab.Theanti-CD38drugsare currentlybeingevaluated fortheirefficacyinother hematologicalmalignancies (non-Hodgkin lymphoma,chronic lymphocytic leukemia).10 This unique clinical laboratory problem is a must know entity forcliniciansandtransfusionmedicinespecialists.Itisalso emphasizedthatcommunicationtothebloodbankaboutthe initiationofdaratumumabforMMpatientsiscrucialtoavoid unnecessarydelayinthereleaseofcompatibleunits.
Conclusion
Daratumumabandother anti-CD38MoAbsareemerging as apromising targetedapproachfor patientswith refractory relapsed MM. However, they are not without limitations. These drugs interfere with compatibility testing thereby leading to misinterpretations of test results and delay in bloodtransfusions.Time-consumingspecialtechniquesare
neededtonullifythedrug’sinterference.Everycentershould recognize its mode of testing basedon the accessibility of reagents, availability ofmanpower and expertise, antigen-matchedblood and itsinventory and turnaround time.Of note, theDTT-basedmethodhasbeenacceptedworldwide. Communication to the Transfusion Medicine Department regardingtreatmentwithsuchdrugsismandatorytoensure safe transfusions in these patients. Knowledge related to theseinadvertentadverseeffectsisessentialforoptimizing transfusionrequirementsinthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
WethankMs.Manimegalai,LabTechnologistforcarryingout thetechnicalaspectsinvolvedinthisstudy.
r
e
f
e
r
e
n
c
e
s
1.MoreauP,vandeDonkNW,SanMiguelJ,LokhorstH,NahiH, Ben-YehudaD,etal.Practicalconsiderationsfortheuseof daratumumab,anovelCD38monoclonalantibody,in myeloma.Drugs.2016;76(8):853–67.
2.ChapuyCI,AguadMD,NicholsonRT,AuBuchonJP,CohnCS, DelaneyM,etal.Internationalvalidationofadithiothreitol (DTT)-basedmethodtoresolvethedaratumumab
interferencewithbloodcompatibilitytesting.Transfusion (Paris).2016;56(12):2964–72.
3.MurphyMF,DumontLJ,GreinacherA.Interferenceofnew drugswithcompatibilitytestingforbloodtransfusion.NEngl JMed.2016;375(3):295–6.
4.ChapuyCI,NicholsonRT,AguadMD,ChapuyB,LaubachJP, RichardsonPG,etal.Resolvingthedaratumumab
interferencewithbloodcompatibilitytesting.Transfusion (Paris).2015;556Pt2:1545–54.
5.AnaniWQ,DufferK,KaufmanRM,DenommeGA.HowdoI workuppretransfusionsamplescontaininganti-CD38? Transfusion(Paris).2017;57(6):1337–42.
378
revbrashematolhemoter.2017;39(4):375–3787. AnaniWQ,MarchanMG,BensingKM,SchanenM,PieferC, GottschallJL,etal.Practicalapproachesandcostsfor provisioningsafetransfusionsduringanti-CD38therapy. Transfusion(Paris).2017;57(6):1470–9.
8. ,AABBAssociationBulletin#16-02Mitigatingtheanti-CD38 interferencewithserologictesting[Internet].Bethesda,MD: AABB;2016.Availablefrom:https://www.aabb.org/programs/ publications/bulletins/Documents/ab16-02.pdf[cited29.5.16].
9.vandeDonkNW,MoreauP,PlesnerT,PalumboA,GayF, LaubachJP,etal.Clinicalefficacyandmanagementof monoclonalantibodiestargetingCD38andSLAMF7in multiplemyeloma.Blood.2016;127(6):681–95.