Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Universal
newborn
hearing
screening:
knowledge
of
pediatricians
and
neonatologists
in
the
city
of
Jundiaí,
São
Paulo,
Brazil
夽
,
夽夽
Ana
Carolina
Moreno
de
Campos
∗,
Henrique
Yassuhiro
Shirane,
Paulo
Vitor
Atsushi
Takemoto,
Edmir
Américo
Lourenc
¸o
FaculdadedeMedicinadeJundiaí,Jundiaí,SP,Brazil
Received29August2013;accepted9March2014 Availableonline13August2014
KEYWORDS
Hearing; Questionnaires; Spontaneous otoacoustic emissions;
Neonatalscreening
Abstract
Introduction:Hearinglosshassevereemotional,psychological,andsocialconsequences.The earlyidentificationofhearingimpairmentiscrucial.
Objective: To evaluate and quantify the knowledge of neonatologists, pediatricians, and residentsinpediatricsregardingdetection,riskfactors,earlydiagnosis,andreferralfor reha-bilitationofpatientswithneonatalhearinglossinJundiaí,stateofSãoPaulo,Brazil.
Methods:Thiswasacross-sectionalcontemporarycohortstudyincluding47physiciansfrom threehospitalsandaquestionnairewith15items.
Results:Mostoftherespondents(83%) hadreceivedinformationabouthearinglossintheir medicalcourses,buthadnoknowledgeoftechniquesforhearingevaluation,anddegreesand typesofloss.Allphysiciansagreedthatinthefirstsixmonthsoflife,itispossibletoevaluate hearingfunctionandthatitisthephysician’sresponsibilitytoassessthenewborn.Regarding theagethatthechildcanreceiveauditory rehabilitation,theendofthefirst yearandthe secondyearoflifepredominates.
Conclusion: Most respondents know the risk factors for the detection of neonatal hearing impairment,knowhowtoperformprocedures,andrecognizetheimportanceofdiagnosisof hearinglossandtheneedtorefersuspectedcases,butmostdonotknowthetechniquesused toassesshearinginnewborns.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Institution:FaculdadedeMedicinadeJundiaí,Jundiaí,SP,Brazil.
夽夽
Pleasecitethisarticleas:deCamposAC,ShiraneHY,TakemotoPV,Lourenc¸oEA.Universalnewbornhearingscreening:knowledgeof
pediatriciansandneonatologistsinthecityofJundiaí,SãoPaulo,Brazil.BrazJOtorhinolaryngol.2014;80:379---85.
∗Correspondingauthor.
E-mail:[email protected](A.C.M.deCampos).
http://dx.doi.org/10.1016/j.bjorl.2014.07.006
PALAVRAS-CHAVE
Audic¸ão; Questionários; Emissõesotoacústicas espontâneas;
Triagemneonatal
Triagemauditivaneonataluniversal:conhecimentodospediatraseneonatologistas emJundiaí,SãoPaulo,Brasil
Resumo
Introduc¸ão:A deficiênciaauditiva acarretagraves consequênciasemocionais,psicológicase sociais,sendoimprescindívelaidentificac¸ãoprecocedealterac¸õesauditivas.
Objetivo:Avaliarequantificaroconhecimentodemédicosneonatologistas,pediatrase resi-dentesemPediatria,sobredetecc¸ão,fatoresderisco,diagnósticoprecoceeencaminhamento parareabilitac¸ãodospacientesacometidospordeficiênciaauditivaneonatalnomunicípiode Jundiaí,SP.
Método: Estudodecoortecontemporâneacomcortetransversal,incluindo47médicosdetrês instituic¸õeshospitalares,comaplicac¸ãodeumquestionáriode15perguntas.
Resultados: Grandepartedosentrevistados(83%)teveinformac¸õessobredeficiênciaauditiva emseuscursosmédicos,emsuamaioriadesconheciamtécnicasdeavaliac¸ãoauditivana infân-cia,grausetiposdeperda.Todosrelataramquenosprimeirosseismesesdevidajáépossível avaliaraaudic¸ão,sendodeverdomédicosepreocuparcomsuacomunicac¸ão.Comrelac¸ãoà idadeemqueacrianc¸apodereceberareabilitac¸ãoauditiva,predominaramofinaldoprimeiro eosegundoanodevida.
Conclusão:A maioriadosentrevistados conheceosfatoresde riscoparaadetecc¸ão neona-taldadeficiênciaauditiva,realizaprocedimentos,reconheceaimportânciadodiagnósticoda deficiênciaauditivaeanecessidadedeefetuarencaminhamentodoscasossuspeitos, porém desconhecetécnicasdeavaliac¸ãodaaudic¸ãoemneonatos.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hearinglosshassevereconsequencesforthedevelopment of language and communication in children. In addition to emotional, psychological, and social problems, it also affectstheirfamilies.1Forthisreason,theearly
identifica-tionofhearingimpairmentisessentialforearlyadaptation ofhearingaidsandauditorystimulation,allowing appropri-atedevelopmentandminimizingthesocioeconomicimpact ofthistypeofdisability.Theimplementationofthe univer-salnewbornhearingscreening(UNHS)programallowsrapid audiologicalscreeningofchildrenforasubsequentfurther assessment,dependingontheneed.
In accordance with Resolution 01/99 of the Brazilian Committee onHearing Loss in Childhood, the UNHS aims to evaluate all newborns,2 and is considered effective if
at least 95% of all newborns are evaluated. If there is a failurein theimplementation of UNHS, the recommenda-tionis toprioritize newborns at greatest risk of deafness and gradually expand the service to all newborns. The term‘‘screening’’referstotheprocessofapplyingcertain fastandsimplemeasurestoalarge numberofindividuals thatwillidentifyhigh probabilityof diseasein thetested function.3 It is not a diagnostic procedure, but rather a
methodtoidentify,amongasymptomaticindividuals,those morelikelyofpresentingthestudieddisease.3
Thus, it is suggested that UNHS beperformed through objectivemeasures (otoacoustic emissions [OAEs]), which can be complemented by the evoked auditory brainstem response(ABR) in the firstmonth of life, afterwhich the diagnosismustbemadebythreemonthsofageand inter-ventionmustbestartedatsixmonths.3
UNHS is mandatoryin accordancewith municipal laws inseveralcitiesinBrazil,4,5 anditiscurrentlyrequiredby
FederalLawN◦12,303ofAugust2,2010.6Thelawrequires
thatallhospitalsandmaternityunitsperformthe examina-tionfree of chargeduring the firstdaysof thenewborn’s life.
Theincidence ofbilateral hearing lossin healthy new-bornsisestimatedatonetothreecasesperthousandlive births,andfrom2%to4%ofchildreninintensivecareunits.7
Itisestimatedthat7---12%ofallnewbornshaveatleastone riskfactorforhearingimpairment.8
Inrecentyears,earlydetectionandtreatmentof hear-ing loss have gained great importance in pediatric and otorhinolaryngologypractice.9 Pediatricians and
neonatol-ogists play a key role in interdisciplinary teams that work to prevent hearing loss, as the first profession-als who come into contact with newborns. Due to this fact, their evaluation and knowledge about the risk fac-tors for neonatal hearing loss are of utmost importance for the child’s audiological follow-up. Teaching (univer-sity) hospitals are constantly engaged in the promotion of the theory, research, and practice of interdisciplinar-ity,but thisrealitydoes notalwaysapplytoallmunicipal hospitals.
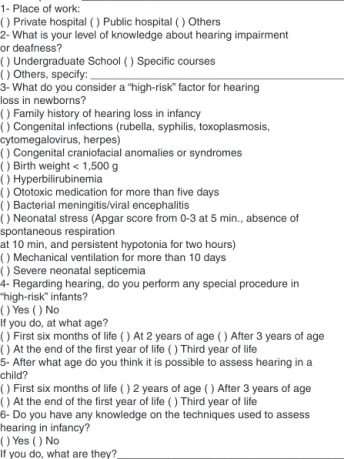
Therefore, this study aimed to evaluate and quantify, throughtheuseofaquestionnaire(Fig.1),theknowledge ofneonatologists,pediatricians,andpediatricresidentson riskfactors,earlydiagnosis,andrehabilitationofnewborns withhearingimpairmentinthecityofJundiaí,stateofSão Paulo,Brazil.
Materials
and
method
Date of birth: ________/ ______/ ______
Year of Graduation from Medical School________________
Current position: ____________________________________________ 1- Place of work:
( ) Private hospital ( ) Public hospital ( ) Others
2- What is your level of knowledge about hearing impairment or deafness?
( ) Undergraduate School ( ) Specific courses
( ) Others, specify: ___________________________________________ 3- What do you consider a “high-risk” factor for hearing
loss in newborns?
( ) Family history of hearing loss in infancy
( ) Congenital infections (rubella, syphilis, toxoplasmosis, cytomegalovirus, herpes)
( ) Congenital craniofacial anomalies or syndromes ( ) Birth weight < 1,500 g
( ) Hyperbilirubinemia
( ) Ototoxic medication for more than five days ( ) Bacterial meningitis/viral encephalitis
( ) Neonatal stress (Apgar score from 0-3 at 5 min., absence of spontaneous respiration
at 10 min, and persistent hypotonia for two hours) ( ) Mechanical ventilation for more than 10 days ( ) Severe neonatal septicemia
4- Regarding hearing, do you perform any special procedure in “high-risk” infants?
( ) Yes ( ) No If you do, at what age?
( ) First six months of life ( ) At 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
5- After what age do you think it is possible to assess hearing in a child?
( ) First six months of life ( ) 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
6- Do you have any knowledge on the techniques used to assess hearing in infancy?
( ) Yes ( ) No
If you do, what are they?______________________________________
7- Do you routinely assess hearing in your patients? ( ) Yes ( ) No
If you answered “Yes”, at what age do you perform this assessment? ( ) First six months of life ( ) 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
8- What hearing tests do you apply?
__________________________________________________________ __________________________________________________________ __________________________________________________________ 9- Do you know the classifications for the different degrees of
hearing loss?
( ) Yes ( ) No If you do, how do you classify them?
__________________________________________________________ __________________________________________________________ 10- Do you have knowledge on the different types of hearing loss? ( ) Yes ( ) No If you do, how do you differentiate them?
__________________________________________________________ __________________________________________________________ 11- When do you refer a child to a hearing assessment specialist? ( ) When the mother has a complaint ( ) When you perceive a problem during the assessment
( ) When the child is at high risk for hearing loss ( ) routine
12- At what age do you refer a child to a hearing assessment specialist? ( ) First six months of life ( ) 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
13- At what age do you think a child can use a hearing aid? ( ) First six months of life ( ) 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
14 – At what age do you think a child can undergo speech therapy for deafness?
( ) First six months of life ( ) 2 years of age ( ) After 3 years of age ( ) At the end of the first year of life ( ) Third year of life
15- Do you think physicians are responsible for assessing the child’s communication skills?
( ) Yes ( ) No
Figure1 Questionnaireusedinthestudy.
This research was designed as a contemporary cross-sectional cohort study. Data collection consisted of completingaquestionnaire,whichincludedeight multiple-choice questions, six yes/no questions, and an essay question.Everytimethechosenanswerwas‘‘yes’’, respon-dentswereinstructedtoexpandtheanswer,describingtheir conduct.
Thisquestionnairewasthesameasthatusedinthestudy performedbyColozzaandAnastasio,10withminorchanges.
Beforecompletingit,respondentswererequiredtosignan informedconsent,withtherespondent’sidentificationand signature,authorizingparticipationintheresearchanduse ofdata.Thequestionnairesweredeliveredpersonallybythe author,whowitnessedthecompletionofthequestionnaire inordertoansweranyquestionsandtoensurethat physi-ciansrespondedimmediately.Therewerenointerviews.In eachhospital,accesstotheemployees’shiftscheduleswas obtainedinordertoapproachtheseprofessionalsinthebest manner.
Theapplicationof60questionnaireswasplanned,each consistingof15questions,including:workplace;conditions toacquireknowledgeoncongenitalhearingloss;knowledge ofhigh-riskfactorsforhearingloss;conductwhentreatinga childathighriskforhearingloss;minimumagepossiblefor hearingassessment;hearingassessmentinchildrenasa rou-tine;specifictestsusedinhearingassessmentinchildhood; degreesandtypesofhearingloss,includingagefor refer-raltotheotorhinolaryngologist;appropriateageforhearing
aiduse;ageatwhichthechildcanundergospeechtherapy; andthephysician’sresponsibility inrelation tothechild’s communicationcapacity.Therewerealsoquestionsaimed toidentifytherespondent,suchasage,yearofgraduation, and medical specialty (pediatrics, neonatology, pediatric residency).
ThisstudywasapprovedbytheResearchEthics Commit-teeoftheInstitutionunderprotocolN◦146/2011.
Statisticalanalysiswasconductedbythestatistician in charge of the Support Center for Research and Teaching (NúcleodeApoioàPesquisaeàDocência---NAPED)ofthe Institution.
Results
Atotalof47questionnaireswerecompletedof60planned; 13physiciansrefusedtoparticipate.
The meanage of respondentswas40.58 yearsandthe meantimeaftergraduationwas15.06years.
Table1 Workplaceofinterviewees(n=47).
Workplace n %ofresponses
Privatehospital 11 23.4
Publichospital 8 17.0
Publicandprivatehospitals 19 40.5 Publicandprivatehospitalsand
otherplaces
5 10.7
Privatehospitalandotherplaces 2 4.2 Publichospitalandotherplaces 1 2.1
Others 1 2.1
Total 47 100
otherplaces(officesandBHUs),one(2.1%)inapublic hospi-talandelsewhere,andone(2.1%)onlyelsewhere(Table1). Thirty-nine(83%)respondentssaidtheyacquired knowl-edgeoncongenital hearingloss duringthe undergraduate course,five(10.6%)saidtheyhadtakenaspecificcourse, seven (14.9%) had taken other courses, and one (2.7%) didnotanswer thequestion,surpassingthetotalof100%, considering thatthreeanswered ‘‘undergraduate course’’ and‘‘specificcourse’’ andtwoanswered ‘‘undergraduate course’’ and ‘‘others’’. Regarding those who answered ‘‘others’’, they had to specify their answers and thus, two answered ‘‘during residency’’, two reported having acquiredknowledgethroughmedicalliterature,andthree didnotanswer.
Regardingthe questiononthe presenceof ‘‘highrisk’’ factors, in descending order and with the possibility of multiple responses, the most often identified were con-genital infections (intrauterine or perinatal), identified by 46 (97.9%); ototoxic medication for more than five days,41(87.2%);bacterialmeningitis,39(83%);congenital craniofacialabnormalitiesorsyndromes,38(80.9%); hyper-bilirubinemia, 31 (66%); birth weight<1500g, 31 (66%); neonatalstress,30(63.8%);familyhistoryofhearinglossin infancy,30(63.8%);severeneonatalsepsis,30(63.8%);and mechanical ventilation for morethan 10 days,18 (38.3%) (Table2).
Table2 Riskfactorsforhearinglossreportedby respon-dents(n=47).
Riskfactorsforhearingloss n %of responses
Congenitalinfections 46 97.9
Ototoxicmedicationformorethan fivedays
41 87.2
Bacterialmeningitis 39 83.0
Congenitalcraniofacialanomaliesor syndromes
38 80.9
Hyperbilirubinemia 31 66.0
Birthweight<1500g 31 66.0
Neonatalstress 30 63.8
Familyhistoryofhearinglossin childhood
30 63.8
Severeneonatalsepticemia 30 63.8 Mechanicalventilationformorethan
10days
18 38.3
34 13
Yes
No
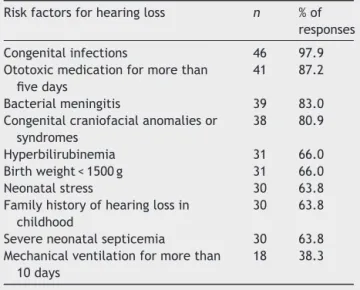
Figure2 Performprocedureswithnewbornsat‘‘highrisk’’ forhearingloss(n=47).
Regardingthequestionconcerningtheroleofthe physi-cianwhentreatingachildat‘‘high risk’’forhearingloss, 34 (72.3%)respondents saidtheyperformed sometype of procedure,while13(27.7%)saidtheydidnot.Ofthe affir-mativecases,all34performeditwithinthefirstsixmonths ofthechild’slife(Fig.2).
Professionalswereaskedtodefineat whatagehearing could be evaluated in children, and 47 (100%) physicians responded that it is possible to do it within the first six monthsofachild’slife.
Fifteen(31.9%)reportedhavingknowledgeaboutspecific teststoassesshearinginchildren,and32(68.1%)answered notothatquestion(Fig.3).Oftheaffirmative cases,five physicians (33.3%) said they knew of the OAE test, five (33.3%) reported having knowledge of OAE and ABR, two (13.3%)onlyofABR, andthree(20.1%)didnotanswer the question.
Twenty-fourphysicians(51.1%)confirmedthatthey rou-tinelycheckhearingintheirpatients,while23(48.9%)said theydidnotcheck(Fig.4).Ofthe24whostatedthatthey assesshearing,22(91.7%)dosointhefirstsixmonthsoflife,
15
32
Yes
No
24
23 Yes
No
Figure4 Routinelyassesshearinginchildren(n=47).
one(4.2%)performsthetestattheendofthefirstyear,and one(4.2%)didnotrespond.
Using anopen question,respondentswereaskedwhich hearing test is appliedin the routine care; theresponses were diverse. Ten (41.6%) answered that they applied coarseexaminations(suchassoundstimuli,clapping, rat-tles,buzzers),eight(33.3%)appliedtheOAEtest,two(8.3%) referred the patients to the audiologist, one (4.1%) per-formed the ABR (auditory brainstem response) test, one (4.1%) performed theOAE and ABR tests,one (4.1%) per-formedaudiometry,andone(4.1%)didnotrespond.
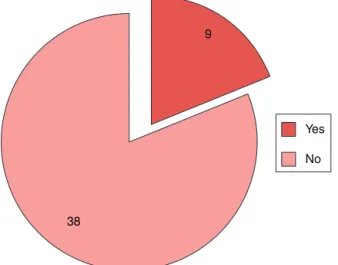
Regardingtheknowledgeofaclassificationfordifferent degreesofhearingloss,only nine(19.1%)reportedhaving this knowledge, while 38 (80.9%) said they did not know aboutit(Fig.5).Oftheaffirmativeresponses,three respon-dents(33.3%)classifiedhearinglossasmild,moderate,and severe,one(11.1%)classifieditasmild,moderate,severe, andprofound,andone(11.1%)classifieditascongenitalor acquired.Four(44.4%)didnotanswerthequestion.
Regardingthequestiononhavingknowledgeofthe differ-enttypesofhearingloss,12(25.5%)answered‘‘yes’’and35 (74.5%)answered‘‘no’’(Fig.6).Participantswhoanswered yes(n=12)hadtospecifyhowtheydifferentiatedhearing
9
38
Yes
No
Figure5 Knowledgeaboutthedifferentdegreesofhearing loss(n=47).
Yes 12
35
No
Figure6 Knowledgeaboutthedifferenttypesofhearingloss (n=47).
loss:three(25%)answeredas‘‘peripheral/central’’,three (25%)as‘‘conductive/sensorineural’’,andsix(50%)didnot answer.
Respondentswereaskedamultiple-choicequestionwith four alternatives, regarding the situation in which the respondentwould send a child to a hearing specialist. In descendingorder,theanswerswerewhenyounotice some-thingduringyourassessment,34(72.3%);whenthemother hasacomplaint,29(61.7%);whenthechildisat highrisk forhearingloss, 28(59.6%);and asaroutine,15(31.9%). Seven respondents (14.9%) gave two answers, 20 (42.5%) gavethreeanswers,andfour(8.5%)gavefouranswers.
Regardingtheageatwhichthechildshouldbereferred toaspecialist, theresponseswere:39 (83%)inthefirst6 monthsofage,four(8.5%)attheendofthefirstyear,two (4.2%)inthesecondyearoflifeandtwo(4.3%)inthethird yearoflife.
Regardingtheageatwhichthechildcanwearahearing aid,18(38.3%)saiditwaspossibletousethemwithinthe firstsix monthsof life, 13 (27.6%) at the end of thefirst year,eight(17%)inthesecondyearoflife,two(4.2%)after 3yearsofage,andthree(4.2%)inthethirdyearoflife.Four respondents(8.5%)didnotanswerthisquestion.
Regarding the question, ‘‘at what age the respondent considers that the child can undergo speech therapy for deafness?’’,18(38.2%)saidattheend ofthefirstyearof life,13(27.7%)insecondyear,10(21.2%)answeredwithin thefirstsixmonths,four(8.5%)after3yearsofage,andtwo respondents(4.2%)didnotanswerthisquestion(Fig.7).
Allparticipantsbelievethatphysicianshavethe respon-sibilitytoassessthechild’scommunicationcapacity.
Discussion
Themeanageandthetimesincegraduationof the physi-cianswhoparticipatedinthisstudywerehigh,inagreement with the literature,3,11 but different from the study by
ColozzaandAnastasio,10 inwhichmostoftheparticipants
First six months of life
End of the first year of life 10
18 13
4 2
Second year of life
Third year of life
Did not answer
Figure7 Ageatwhichthechildcanundergospeechtherapyforhearingloss(n=47).
theUNHSandhearinglosshadtheirdisseminationrestricted tootorhinolaryngologistsandaudiologists.
Most participants in the present study were pediatri-cians(55.3%),whereastheotherswereneonatologistsand medical residents in pediatrics. Colozza and Anastasio10
showedthatmostrespondentswereresidents(61.1%);two otherstudies8,12 includedpediatriciansonly,andonestudy
assessedonlyneonatologists.3Thestudysamplepopulation
representedapproximately15%ofpediatriciansinthecityof Jundiaí,anditwasverifiedthatsomeparticipantsworkedin morethanoneoftheselectedhospitals,resultinginamore restrictedsample.
This study showed a predominance of participants that worked in both private and publichospitals (40.4%). Regardingthoseworking inonly onetypeof hospital, pri-vatehospitalspredominated.Apreviouslypublishedstudy10
didnotspecifythetypeofhospitalwheretherespondents worked, but most worked in hospitals, and a minority in privateclinicsandotherplaces.
It canbe observedthat mostof the respondents(83%) reportedhavingobtainedinformationabouthearing impair-ment during medical school, similar to the results found by other studies.3,8,10 In this study, the majority (68.1%)
ofrespondents saidthey hadnoknowledge of techniques to assess children’s hearing, a finding similar to that in literature.3,8,10Thisresultmaydemonstratethatthefederal
requirementofperformingtheOAEtestdidnotleadthese expertstoseekfurtherinformationonthesubjectand/or therewerenoprogramsthatreportedtheimportanceofthe UNHS,whichhampersearlydiagnosisandtreatment.
The present study included 10 risk factors for deaf-ness,considering thatthe respondents hadthe possibility ofmultiple-choiceanswersforthesefactors,with71% pos-itiveresponses,indicatinggoodknowledgeofpediatricand neonatal clinical practice on the subject (Table 2). This resultwassimilartothat foundinthe literature.3,8,10 The
sevencriteriaofhigh-riskfactorsforhearinglossfromthe JointCommitteeonInfantHearingwerementionedinthe literature: family history, intrauterine or perinatal infec-tions,malformationsinvolvingtheheadandneck,neonates weighinglessthan 1500gat birth,severeneonatal hyper-bilirubinemia,bacterialmeningitis, andsevere hypoxia at
birth. Three additional risk factors were included in this study: ototoxic medications, mechanical ventilation, and neonatal septicemia, following the example of another studyintheliterature.10
All physicians in this study agreed that it is possible toevaluate thechild’shearing withinthefirstsix months of life, which is in agreement with the literature.10,12
This result shows that physicians are concerned with an early diagnosis of children with risk factors for deafness, thus allowingearly treatment andpreventingmajor prob-lemsduringtheirdevelopment.TheBrazilianCommitteeon Hearing Loss in Childhood(Comitê BrasileirosobrePerdas Auditivasna Infância---CBPAI)recommends thattheUNHS be performed in the first three months of life, and that the educationalintervention beperformed in thefirst six monthsoflife.2Thereislossintheoveralldevelopmentof
thechildifthehearinglossisnotdetectedandtreatedin a timely manner, withemotional, educational, and social consequences.
With regard to high-risk children, most respondents (72.3%)repliedthattheyperformhearingassessmentwithin thefirstsix monthsoflife,andthe majority(68.1%)have noknowledgeoftechniquestoevaluatethechild’shearing. In another study,10 75% chose to assess high-risk children
in the firstsix months, and 52.7% of respondents had no knowledge on assessment techniques. Table 2 shows that therespondentshaveknowledgeaboutthecausesofhearing impairment.
Regardingtheroutinehearingassessmentofnewbornsby theparticipants,therewasabalancebetween‘‘yes’’and ‘‘no’’ responses, consistent with the literature,10 except
in one publication,8 which had more positive responses.
Regarding the applied tests spontaneously reported by respondents,theOAE,theABR,andothercoarsertestswere mentioned,similartotheliterature.10Thereported
meth-odsarefast,noninvasive,andeasilyapplied.
AccordingtotheBureauInternationald’Audiophonologie (BIAP),13hearinglossisclassifiedasmild,moderate,severe,
threeoftherespondentscorrectlydescribedthisresponse, similartotheliteratureresults.8,12
Mostrespondentsreportedthattheyhadnoknowledge ofhearingassessmenttechniquesandwereunableto clas-sifythedifferenttypesanddegreesofhearingloss,whichis asourceofconcern,asitsuggestsliteratureand undergrad-uatemedicalcourse deficiencies.Similardiscussionswere conductedinotherstudies,8,10 thatreportedthatknowing
howtodefinethetypeanddegreeofhearinglossisofutmost importance,sothatthedoctorcanperformanappropriate interventionandmakeapredictionofresidualhearing.
Concerningthereferraltoaspecialistinhearing assess-ment,therearesmalldifferencesbetweentheresponsesof thisstudyandtheliterature.3,8,10,12 Mostphysicians
evalu-atedinthisstudy(72.3%)reportedtheyreferthechildwhen thereis a suspected problemduring assessment, whereas anotherstudy10indicatedthat80.5%referthepatientwhen
the child is at high risk of hearing loss, although fewer respondentswereincluded.Onestudy3reportedthatmost
choosetoroutinelysendtheirpatientstospecialized evalu-ation,whereasanother12reportedthatmostchoosetorefer
whenthemotherhasacomplaint,andathird8reporteda
balanceofreferrals,consideringthesuspectedclinical his-toryorthephysician’sownclinicalsuspicion.However,there isanagreementthatthechildcanbereferredtoaspecialist withinthefirstsixmonthsoflife.
Asforthepossibilityofusingahearingaid,respondents thinkthatitcanbeusedbeforetheendofthefirstyearof life.8,10,12 The literature shows similarresults, once again
demonstrating the physician’s concern in relation to the properdevelopmentofpatients.
The physicians assessed in this study had different responsesregardingtheageatwhichthechildcanundergo auditoryrehabilitation,withapredominanceattheendof thefirstyearandthesecondyear oflife,afindingthatis notinagreementwiththeliterature,10inwhichmost
physi-cianssaidthatthechildcanreceivethistypeoftreatment asearlyassixmonthsoflife.
Allparticipantsbelievethatitisthedoctor’s responsibil-itytoassessthechild’scommunication capacity,afinding consistentwithotherstudies.8,10,12
Conclusion
and
comments
Accordingtotheresults,it isclear thatrespondentshave inadequate and incomplete medical knowledge regarding UNHS and hearing impairment. Although it may be con-sidered that there are conditions and trends for early diagnosis of neonatal deafness, there is also a need for
greater exchange between pediatricians, neonatologists, otorhinolaryngologists,andspeechtherapists,comprisinga multidisciplinaryteamaimingtoshareinformation, result-inginbetterprognosisforthesechildren.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.RussoICP,SantosTMM.Audiologiainfantil.4thed.SãoPaulo: Cortez;1994.p.232.
2.Comitê Brasileiro sobre Perdas Auditivas na, Infância., Recomendac¸ão,01/99.JConsFedFonoaudiol.2000;5:3---7.
3.SoaresCP,MarquesLR,FloresNGC.Triagemauditivaneonatal: aplicabilidadeclínicanarotinadosmédicospediatras neona-tologistas.RevCEFAC.2008;10:110---6.
4.BassetoMCA.Triagemauditivaemneonatos.In:CampiottoAR, LevyC,RedondoMC,AnelliW,LopesFO,editors.Tratadode fonoaudiologia.RibeirãoPreto:Tecmedd;2005.p.223---33.
5.TochettoT,VieiraEP.TAN:legislac¸ãobrasileirasobretriagem auditivaneonatal.Barueri:Pró-Fono;2006.p.57.
6.BRASIL.Lein◦ 12.303,de2 deagostode2010. Dispõesobre
aobrigatoriedade derealizac¸ãodoexamedenominado Emis-sõesOtoacústicasEvocadas;2010.Availablefrom:http://www. planalto.gov.br/ccivil03/Ato2007-2010/2010/Lei/L12303.htm
7.SociedadeBrasileiradePediatria.Educac¸ãoMédicaContinuada. Leituras Orientadas --- Neonatologia.Comitê Brasileiro sobre perdasauditivasnainfância.1arecomendac¸ão---período
neona-tal.CorreiosSBP.2001;7:5---9.Availablefrom:http://www.sbp. com.br/showitem.cfm?idcategoria=24&iddetalhe=520&tipo=S
[cited03.03.09].
8.Tschiedel RS, Bandini HHM, Bevilacqua MC. Diagnóstico da deficiênciaauditivanainfância:umaavaliac¸ãodonívelde con-hecimentodospediatrasdeumacidadedaregiãoCentro-Oeste paulista.PediatrMod.2000;36:607---17.
9.Sousa LCA, Piza MRT, Costa SS, Colletes HM, Pipano PC. A importância do diagnóstico precoce da surdez infantil na habilitac¸ãododeficienteauditivo.ActaAWHO.1998;17:120---8.
10.ColozzaP,AnastasioART.Avaliac¸ão,diagnósticoetratamento dasurdez---conhecimentoecondutademédicoscomatuac¸ão emneonatologiae/oupediatriadeumhospital-escolaterciário. SãoPauloMedJ.2009;127:61---5.
11.HilúMRPB,ZeigelboimBS.Oconhecimento,a valorizac¸ãoda triagemauditiva neonataleaintervenc¸ãoprecocedaperda auditiva.RevCEFAC.2007;9:563---70.
12.Barros ACT, Galindo MAC, Jacob RTS. Conhecimento e con-duta de pediatras frente à deficiência auditiva. Pediatria. 2002;24:25---31.