D
ENTAL NURSES
IN TRINIDAD AND TOBAGO1
Lhda I? SteeZe2
I
NTRODUCTION
The Dental Nurses Training Scheme in Trinidad and Tobago, that was modelled on the New Zealand program, began operating in 1976. This program produced the island’s first qualified den- tal nurses in 1978. Eight years later, dur- ing the period from December 1986 toFebruary 1987, nearly all the dental nurses employed by the Government Dental Service attended continuing edu- cation seminars at a new Dental Nurses Training School in Arima, St. George County, Trinidad. During this time a study was undertaken, the purpose of which was to determine the dental nurses’ geographic distribution, alloca- tion of time to different activities, knowledge of basic oral health education messages, and problems encountered in their work.
’ This article will also be published in Spanish in the Bo- let% de la Oficina Sanitaria Panamencana.
* Dental Consultant, PAHO, 49 Jemingham Avenue, Belmont, Trinidad, West Indies.
M
ETE-IODOLOGY
Sixty-one of the 77 national graduates who had graduated from the training program between 1978 and 1984 were included in the study (Table1). Of these 61 dental nurses, only five were men. Although there were 66 den- tal nurses employed by the Government Dental Service at the time of the study, five were unable to attend the continu- ing education seminars. Information on the distribution of dental nurses throughout the country was obtained from the study participants. Information on the nonparticipants was obtained from the Chief Dental Offricer. A ques- tionnaire was used to determine alloca- tion of time to different activities, work patterns, and problems encountered by the dental nurses. A quiz (Annex 1) was
used to test their knowledge of basic oral health education messages.
R
ESULTS
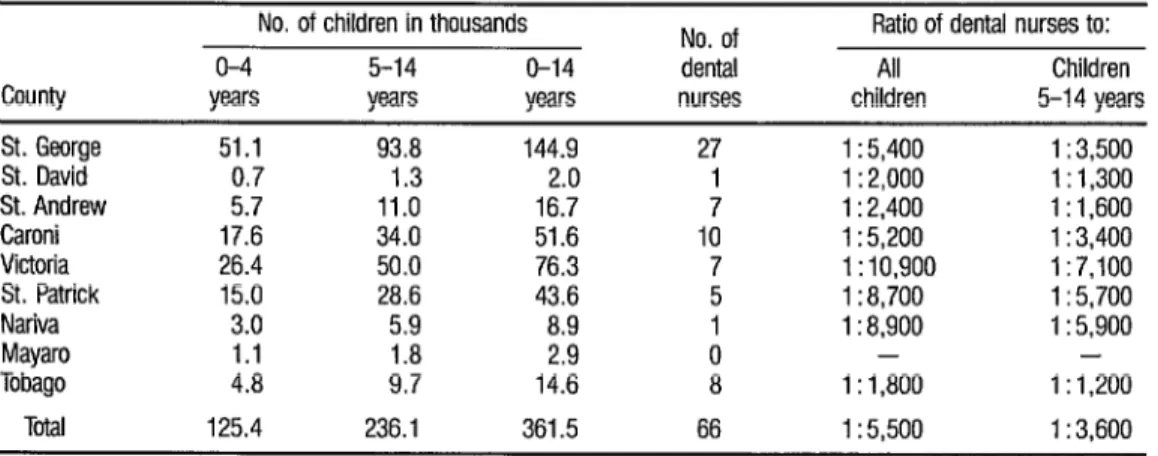
The geographic distribution of dental nurses throughout Trinidad and Tobago is uneven. Table 2 shows that the ratio of dental nurses to children ranged from one per 1,800 children inTABLE 1. The number of students graduating tom the Dental Nurses Training School in 1978- 1984:
Year
1978 1980
1981 1983 1984 Total
Study participants
15 11
17 6 12 61
No. of students graduating National Foreign graduates graduates
21 10
13 6
20 4
11 8
12 4
77 32
Total graduates
31 19
:i 16 109
a This schwl closed its dwrs in 1984.
TABLE 2. Dental nurse to child population ratios by county. Population figures are from the 1981 Census, rounded to the nearest 100 (7).
No. of children in thousands No. of Ratio of dental nurses to:
o-4 5-14 O-14 dental All Children
County years years years nurses children 5-14 years
St. George 51.1 93.8 144.9 27 1 : 5,400 1 : 3,500
St. David ki.3 1.3 1 1 : 2,000 1: 1,300
St. Andrew
17:6 11.0
1:;”
1 : 2,400 1 : 1,600
Caroni 34.0 51:6 1; 1 : 5,200 1 : 3,400
Victoria 26.4 50.0 76.3 7 1 : 10,900 1 : 7,100
St. Patrick 15.0 28.6 43.6 5 1: 8,700 1 : 5,700
Nariva 3.0 5.9 8.9 1 1: 8,900 1 : 5,900
Mayaro 1.1 1.8 2.9 0 - -
Tobago 4.8 9.7 14.6 8 1: 1,800 1 :I,200
Tota 125.4 236.1 361.5 66 1 : 5,500 1: 3.600
two counties. Table 3 shows the dramatic improvement in the dental operator to population ratio that the dental nurses training scheme has brought about over the last 15 years.
Most of the dental nurses’ time (a mean of 6.9 half-day sessions per week) was allocated to treating children in the clinics (Table 4). All but one den- tal nurse spent between one and four ses- sions per week providing dental health education in schools (mean, 2.5 ses- sions). Other dental health education ac- tivities and clerical work took up the re- maining time (mean, 0.7 sessions).
The dental nurses reported treating between four and 20 patients per day, the mean number treated per day being 12. Forty of the dental nurses
2
(66%) reported that they had a dental
2
TABLE 3. Dental operator to population ratios, 1972-1987.
1972 1987 Population
Total number of dentists
Number of government dental officers Number of dental nurses
Total number of dental operators (dentists plus dental nurses)
Total number of government dental operators (dental officers plus dental nurses)
Dental operator: population ratio
Government dental operator: population ratio
1 ,ooo,ooo
1,200,000553 91
16 15
- 66
55 157
16
1 : 18,000 1 : 7,6:: 1: 62,500 1: 14,800
a It is difficuft to obtain accurate figures for the number of dentists in Tnnidad and Tobago before 1980, when the Dental Profession Act came Into force and a dental register was started The number used here is taken from Atwell (2)
TABLE 4. Distribulion of dental nurses according to half-day sessions spent on clinical, dental health education (DHE), and clerical activiis.
Distribution of dental nurses according to number of half-day sessions spent on
different activities
No. Clinical DHE in
of sessions work schools
DHE in prenatal and child welfare clinics or clerical work
0 1
2 3 4 5 6 7 8 9 Mean
- - 33
IO 15
- 21 13
1 28 -
- 2 -
4 - -
10 - -
35 1 -
9 - -
2 - -
6.9 2.5 0.7
2
2
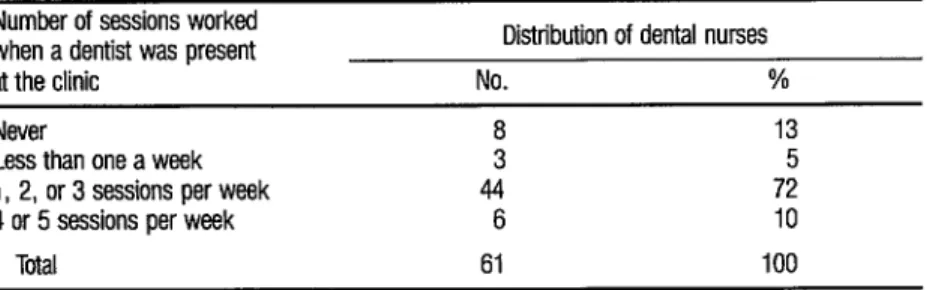
- Most of the dental nurses (53, 2or 87%) worked at a clinic where there
Q was a dentist. However, none of the clin- its had a full-time dentist, the number of ..g
0, half-day sessions that the dentist was a 3 present ranging from fewer than one a 2 week to five per week (Table 5). Many of
2
366
the health clinics have only one dental surgery, so the dental nurse and dentist are unable to run a clinic at the same time. Of those 53 dental nurses who had a dentist at their clinic, 39 (73%) spent no sessions per week, eight (16%) spent
one session per week, and six (11 Oh)
spent two sessions per week working at the same time as the dentist.
TABLE 5. Disbibulfon of dental nurses according to the number of sessions worked when a dentist was present af the dinic.
Number of sessions worked when a dentist was present at the clinic
Distribution of dental nurses
No. %
Never
Less than one a week 1, 2, or 3 sessions per week 4 or 5 sessions per week
Total
13 5
44 72
6 IO
61 100
fects cited most often were increased awareness of oral health, increased accep- tance of dental treatment without fear by children, improved oral hygiene of chil- dren, and assignment of greater value to oral health by the public.
A wide range of problems were mentioned by the dental nurses. Those most frequently cited were inade- quate facilities, equipment, supplies, and maintenance. The 10 problems and
recommended changes most frequently cited are listed in Table 6.
The results of the quiz (‘Table 7) show that there was fairly wide varia- tion of opinion among the dental nurses about basic oral health messages. The four questions that could be answered true or false were included to stimulate discussion during the seminars on the role of toothbrushing per se and the role of fluoride toothpaste in preventing de- cay. Nearly all of the dental nurses (95 % and 97%, respectively) knew of the harmful effects of sugar-containing drinks and consumption of sweets be- tween meals. The most commonly held misconception was that eating fruit helps to clean your teeth. Only 11% knew this to be false.
TABLE 6. The 10 problems and desired changes most frequenfly cited by the suruey respondents.
1 Problems relating to inadequate facilities, equipment, supplies, and maintenance. 2 Problems with transportation to dental heafth education visits.
3 Problems with other members of the staff (particularly the dentist and dental assistant). 4 More dental health education and preventive work should be done.
5 Difficulties in getting children to come to the clinic (attendance, time-keeping, and transporta- tion problems).
6 More in-service training is needed.
7 Dental nurses should be based in the schools.
8 The range of work of dental nurses should be extended to include older children and a wider range of clinical techniques.
9 Administrative changes are needed.
TABLE 7. Quiz questions, answers, and results.
Questions and answers
% giving correct response
1 Eating fruit helps to clean your teeth (false)
2 Rinsing your mouth after eating sweets helps to prevent decay (false) 3 Toothbrushing helps to prevent decay on the smooth surfaces of the teeth 4 Toothbrushing helps to prevent decay in the piis and fissures of the teeth 5 Toothbrushing helps to prevent decay between the teeth
6 Brushing your teeth helps to prevent gum disease (true) 7 It is better to brush your teeth before a meal rather than after
8 You can get decay from a meal which does not contain any foods with sugar in them (false)
9 It is better for children to have sweets at mealtimes rather than between meals (true) 1
10 Honey is less decay-producing than whiie sugar (false) 11 Brown sugar is less decay-producing than white sugar (false) 12 Drinks containing sugar (e.g., Coke) are harmful to teeth (true)
13 Sugar control is more important for preventing decay than any other measure (true)
14 Dental decay increases during pregnancy (false) 15 Teeth decay less as you get older (true)
11 46 a a
ii5 a
56
97 62 74 95
69 66 49
These questions can be answered either true or false.
D
ISCUSSION AND
CONCLUSIONS
This study has shown that the distribution of dental nurses throughout the country is uneven, both geographi- cally and in relation to the child popula- tion. Redistribution of the dental nurses would not solve the problem, because there are too few of them. More dental nurses need to be trained. As there are over 360,000 children, it would be neces-sary to have 120 dental nurses to give a dental nurse to child ratio of 1 to 3,000.
This is nearly twice as many dental nurses as are presently employed. One dental
nurse to 3,000 children would be an ac- ceptable ratio, but it is much higher than in New Zealand, where one dental nurse is responsible for 500 schoolchildren in a nonfluoridated area or 900 schoolchil- dren in a fluoridated area.
The child population figures (see ‘Able 2) can only be used as a guide, for the following reasons. The figures quoted relate to children from birth to
14 years of age. Dental nurses treat chil- dren only up to the age of 12, but as the population census groups children into age groups O-4, 5-9, and 10-14, accu-
rate figures for the number of children below the age of 12 are not available. Also, these figures are from the census of
1981, and the population has increased slightly since then. In calculating dental nurse to child population ratios, children
care for preschool children, in practice they tend to confine their clinical activi- ties to schoolchildren. Nevertheless, par- ticularly with regard to oral health educa- tion, preschool children should be considered.
One very encouraging finding was that of all the dental nurses who have been trained, very few have been lost from the Government Dental Service. It could be predicted that if more dental nurses are trained, there would be a simi- lar low natural wastage rate. However, futher training of dental nurses must be considered in the light of facilities avail- able for them when they qualify. If all of the dental nurses needed were to be trained, many new dental surgeries would need to be built, and it may not be feasible to allocate funds for this pur- pose, when other priorities for spending in the field of health care are considered. The dental nurses were found to spend about three-tenths of their time performing health education activities. This is an encouraging finding, indicat- ing that oral health education is rightly regarded as important. However, there seems to be a basis for inconsistency and confusion in the messages they are giving to children and pregnant women. The continuing education seminars that these dental nurses attended appeared to be useful, but in order to ensure that they give the correct oral health messages, present them effectively, and keep up with new developments, further courses are strongly recommended.
There is wide variation in the average number of patients seen by the dental nurses per day. Perhaps efficiency could be improved if those dental nurses who seldom or never work with a dental assistant could have an assistant working with them all the time.
It is apparent from this study that the dental nurses are working alone most of the time. According to the 1980
Dental Profession Act, “A dental nurse is qualified to treat children only and such treatment shall be carried out in fa- cilities or services operated or conducted by government or under the direct or in- direct supervision of a dentist in private clinics.” This seems to infer that they must be supervised in private clinics, but not necessarily in government clinics. Al- though it is not illegal for them to work alone, a teamwork approach could lead to improvements in the service. The orig- inal scheme made provision for some dental nurses to be appointed as supervi- sors. None have been appointed, so the only people who could help to supervise dental nurses are the government dental officers. Both dental officers and dental nurses could benefit from working more together.
Although all the dental nurses thought that they had had an ef- fect on the oral health of the children in the country, in the absence of data from epidemiologic studies this cannot be evaluated objectively.
The problem of inadequate equipment and supplies must be care- fully investigated to see how the situa- tion could be improved, as this can affect the dental nurses’ efficiency. It might help if they were given training on how to do simple maintenance and repairs themselves.
Despite all the problems, it is clear that the dental nurse program has made a worthwhile improvement in terms of the human resources available for providing dental care to the child population of Trinidad and Tobago.
S
UMMARY
R
EFERENCES
The dental nurse training pro-gram in Trinidad and Tobago has made a substantial improvement in the dental operator to population ratio in the is- lands over the last 10 years. Nevertheless, the 66 dental nurses employed by the Government Dental Service are too few, and are unevenly distributed both geo- graphically and in relation to the child population. Further training of dental nurses, to expand the workforce, must be considered, taking into account the pri- orities for spending in the health care sector.
The dental nurses play an im- portant role in providing oral health edu- cation to children and pregnant women. An ongoing program of continuing edu- cation would help to ensure that their knowledge and skills are kept up to date.
Some of the dental nurses en- counter problems in their work which, if solved, could improve their efficiency and job satisfaction. These problems in- clude maintenance and supply of equip- ment and materials. There is also scope for the dental nurse, dentist, and dental assistant to improve their teamwork.
There is no doubt that the dental nurses training program has had a big impact on oral health services in liin- idad and Tobago, and expansion of this program is to be recommended.
Republic of Trinidad and Tobago, Central Sta- tistical Office. Annual Statistical Digest, vol. 29, 1982.
Atwell. R. V. M. A Plan to Develop the Dental Services of Trinidad and Tobago. Master of Sci- ence Thesis, University of Toronto, 1972. Besford, J. Good Mouth&e
Oxford University Press, 0 J
ing (second ed.). ord, 1984, pp. 51, 53. 88-89, 118, 144-147, and 152.
Health Education Council, En land. The Scien- tif;c Basis of Dental’ Heahh B E ucatzon. London, 1985, pp. 8-11.
Sutcliffe, P Oral Cleanliness and Dental Caries. In: J. J. Murray. The Prevention of Dental Dis- ease. Oxford University Press, Oxford, 1983, pp. 159-174.
World Health Organization. Epidemiology, Eti- ology, and Prevention of Periodontal Disease. WHO Technical Report Series, No. 62 1. Ge- neva, 1978, p. 13.
Silverstone, L. Preventive Dentistry. London, Update Books, 1978, pp. 53-54.
8 Rugg-Gum, A. J. Diet and Dental Caries. In: J. J. Murray. The Preventzon of Dental Disease. Oxford University Press, Oxford, 1983, pp. 3- 82.
ANNEX 1. Answers and Scierdiiic Basis for the Quiz. Question 1: Eating fruit helps to clean your teeth. False.
It is now generally accepted that methods for removing plaque such as eating fibrous foods including apples and carrots are ineffective. Fibrous foods do not reach the recessed areas of the tooth sutface and can never be a substitute for brushing and flossing. (3, 4)
Question 2: Rinsing your mouth after eating sweets helps to prevent decay False.
Rinsing your mouth with water may remove some food particles, but will not remove plaque, or the sugar or acid in the plaque. The carious process will continue undisturbed. Even the effectiveness of an antiseptic mouthwash for caries control has not been established. (4)
Questions 3, 4, and 5: Toothbrushing helps to prevent decay on the smooth surfaces of the teeth, in the pits and fissures, and between the teeth. True or false.
The relationship between oral cleanliness and decay experience is a controversial issue. Sutcliffe (5) reviews the evidence from many studies and concludes that there is no unequivocal evidence that good oral cleanliness reduces caries experience, nor is there sufficient evidence to condemn the value of good oral cleanliness as a caries preventive. However, certain facts about toothbrushing and caries are certain. In order for caries to occur, three factors must be present together: plaque, sugar and a susceptible tooth. Susceptible populations with heavy plaque deposits can remain relatively free from dental caries as long as only small amounts of sugar are eaten. Conversely even with good oral hygiene, twthbrushing inevitably leaves some plaque in fissures and between the teeth, which are prime sites for caries to occur. Therefore individuals who consume a high-sucrose diet will experience decay irrespective of how good or bad their oral hygiene is. Fmm this, the following can be concluded with reasongble certainty: Brushing with a non- fluoride toothpaste will not help to prevent decay except perhaps on the smooth surfaces of the teeth where the plaque is easily accessible. Brushing with a fluoride toothpaste will help to prevent decay, but this effect is attributable to the fluoride in the toothpaste and not to the brushing alone. In view of the controversial nature of these questions, both true and false answers were accepted as correct.
Question 6: Brushing your teeth helps to prevent gum disease. True.
Dental plaque is the prime cause of gingiis and periodontiiis, and there is ample evidence to show that effective removal of plaque bytwthbrushing and other means prevents or causes resolution of gum disease. (6)
Question 7: It is better to brush your teeth before a meal rather than after. True or false.
This is another controversial question. Many dentists now believe that it is better to remove as much plaque as possible before a meal so that any sugar in the food will remain as sugar, because there are no bacteria on the tooth surface to turn it into acid (3). This may be true for the smooth surfaces of the teeth, where the plaque can be adequately removed, but it will make no difference to the pits and fissures and between the teeth, where the plaque is largely inaccessible to the toathbrush. On the other hand, brushing
after a meal with a fluoride twthpaste may help. If &mineralization has occurred, the fluoride in the tooth- paste may swing the balance in favor of rernineralization. (7)
Question 8: You can get decay from a meal which does not contain any foods with sugar in them. False. Sugar, particularly sucmse, would appear to be the most important dietary item in caries etiology, and its presence around plaque-covered tooth surfaces is essential for more than very limited caries development. Although cooked starch can cause some caries, its cariogenicity has been shown to be low, and human epidemiologic studies have frequently recorded low caries experience in people eating high-starch, Iow- sugar diets. (8)
Question 9: It is better for children to have sweets at meattimes, rather than between meals. True. With regard to caries experience, the frequency of sugar intake has been shown to be a more important variable than the total quantity of sugar eaten (8). If sweets are eaten, then it is better to restrict their consumption to specific times, such as mealtimes.
Question IO: Honey is less decay-producing than white sugar. False.
Honey is a very concentrated sugar solution. Sugar and water make up 99.4% of honey If there is any difference, it is very slight. (3)
Question 77: Brown sugar is less decay-producing than white sugar. False.
All variants of white and brown sugar are almost 100% sucrose, and are equally cariogenic. (3)
Question 72: Drinks containing sugar (e.g., Coke) are harmful to teeth. True.
Sugar causes decay and it makes little difference what it is in. Cola drinks have a high concentration of sugar; Coca-Cola has six-and-a-half teaspoons of sugar in one can. (3)
Question 13: Sugar control is more important for preventing decay than any other measure. True, Sugar alone causes decay and eliminating sugar from the diet eliminates decay Fluoride helps to strengthen teeth, but on fts own is not a complete protection (3). The role of oral hygiene has already been discussed.
Question 74: Dental decay increases during pregnancy False.
Contrary to popular belief, there is no evidence that pregnancy has any effect on the rate of decay Neither malnutrition in the mother during pregnancy, nor in the child after birth, increases susceptibilff Calcium cannot be removed from a mother’s teeth during pregnancy (4)
Question 15: Teeth decay less as you get older. True.
Teeth do decay less as you get older because, with time, fluoride builds up in the tooth surface and makes ft less soluble. Also, many of the prime sites for attack may have already been filled. (3)
New Publication
on Caribbean
Medical
litetiure
372
A comprehensive index to the health-related lit- erature of and on the Caribbean area has been published by the University of the West Indies (UWI). Medical Caribbeana, compiled by Laxmi Mansingh, Librarian-in-Charge at the UWI Med- ical Library contains entries on more than 700 monographs and articles gleaned from some 1,100 regional and international journals and dating back to 1679. The literature is indexed under title, names of all authors, and subject, with 1,800 subject cross-references.