13
THREE LEVELS MODEL FOR DIFFERENTIATED
PHARMACIST CLINICAL ACTIVITIES
IN THE COMMUNITY PHARMACY – THE PRACTICAL
APPLICATION
Mónica Condinho
ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Margarida Cavaco
ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Fernando Miranda
Motta pharmacy, Évora, Portugal. ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Carlos Sinogas
ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal. Universidade de Évora, Portugal
Abstract
Introduction: In order to contribute for the real implementation of cognitive pharmaceutical services in
Portugal, a three levels model of pharmacist clinical intervention in the community pharmacy, based on the differentiated patient´s health needs, was proposed by the authors («Three Levels Model for Differentiated Pharmacist Clinical Activities in the Community Pharmacy – The Proposal», accompanying paper).
Objective: To test the practical application of the proposed three levels model for differentiated pharmacist
clinical activities in the community pharmacy.
Methods: The three levels model was implemented in several community pharmacies. The philosophy
of the model, to change the focus of community pharmacies from the product to the patient, was intro-duced under the supervision of a specialized pharmacist, responsible for the pharmacotherapeutic follow-up program. All the pharmacy professionals were instructed to ask the customer about the control of his health problem, whenever applicable. When no non-controlled health problem was detected, dispensing the product fulfils the customer needs and is considered the level 1 service. If a non-controlled health problem was detected, the pharmacist considers the clinical situation and delivers the appropriate counseling, either immediately or delayed for a pharmaceutical consultation, configuring the level 2 service. When, at level 2, emerges the perception that simple and immediate actions would not control the health problem, the patient was invited to integrate the pharmacotherapeutic follow-up program, corresponding to the level 3 service.
Results: The implementation of pharmacotherapeutic follow-up consultations (level 3) started in 2008
and paved the way for the development of this model. Until September 2013, one specialized pharmacist followed 430 patients with recurrent non-controlled health problems, performing around 3200 pharma-ceutical consultations in 20 community pharmacies. The results available for one pharmacy (46 patients) show mean reductions of 26.4±7.68 mg/dL on total cholesterol (n=28; p=2.510x10-3), 1.9±0.73 % on glycated
haemoglobin (n=29; p=0.022) and 26.2±3.79 mmHg on systolic blood pressure (n=23; p=6.197x10-7).
Level 2 consultations started in May 2012. During the first 16 months of implementation in 5 pharmacies, 346 patients were enrolled. A total of 371 consultations were performed and mean reductions of 53.3±9.27 mg/ dL in total cholesterol (n= 19; p=1.913x10-5), 18.3±2.26 mmHg in systolic blood pressure (n=42; p=4.657x10-10)
and 0.2% in glycated haemoglobin (n=2) have been registered.
Conclusion: The three levels model for differentiated pharmacist intervention, based on the pharmacy
customer´s health needs, seem to be a suitable model for the routine implementation of cognitive pharma-ceutical services in Portuguese community pharmacies. Based on this model, the pharmacy can answer to all their customer´s health needs and contributes for significant improvements on patient´s health condition.
Keywords: Cognitive pharmaceutical services, model of pharmacist clinical intervention,
14
Resumo
Introdução: Considerando a limitada implementação de serviços farmacêuticos cognitivos em Portugal, em
particular no que à consulta farmacêutica diz respeito, propôs-se um modelo de intervenção farmacêutica diferenciada, por forma a responder às diferentes necessidades de saúde dos utentes da farmácia, otimizando recursos e valorizando a intervenção clínica do farmacêutico («Three Levels Model for Differentiated Pharma-cist Clinical Activities in the Community Pharmacy – The Proposal», artigo também publicado nesta edição).
Objetivo: Testar a aplicabilidade prática do modelo proposto para intervenção farmacêutica diferenciada
em três níveis de atuação na farmácia comunitária.
Metodologia: Implementação do modelo proposto em várias farmácias comunitárias. A filosofia de
tra-balho subjacente foi apresentada à equipa de cada uma das farmácias pelo farmacêutico especializado em acompanhamento farmacoterapêutico, que supervisionou a sua implementação. A primeira etapa consistiu na mudança de foco da intervenção dos diferentes profissionais de saúde da equipa da farmácia, do produto e da sua venda para o doente e suas necessidades de saúde. Para tal, toda a equipa foi instruída no sentido de, em cada atendimento, questionar, sempre que aplicável, o utente acerca do seu problema de saúde. Perante a ausência de problema de saúde, ou nas situações em que este estava controlado, o profissional satisfez as necessidades do utente pela dispensa solicitada (nível 1). Nos casos em que um ou mais problemas de saúde foram percecionados como não controlados, o colaborador avaliou, em primeiro lugar, a recetividade do doente para o aconselhamento. Em caso afirmativo, um farmacêutico analisou a situação e decidiu a in-tervenção a tomar: um aconselhamento imediato ou um convite com marcação de consulta farmacêutica de nível 2. De imediato ou no âmbito da consulta farmacêutica de nível 2, nas situações mais complexas, com problemas de saúde recorrentemente não controlados, o doente foi encaminhado para a consulta de nível 3, o acompanhamento farmacoterapêutico. O doente manteve-se nesta consulta até ao controlo do proble-ma de saúde ou até que nenhuproble-ma outra intervenção fosse possível ou desejável. Terminado o prograproble-ma de acompanhamento farmacoterapêutico, o doente retornou ao nível 2, onde o seu estado de saúde continuou a ser monitorizado pelo farmacêutico residente.
A prestação de cada um dos níveis foi acompanhada da devida formação da equipa da farmácia e do farma-cêutico indicado para realizar as consultas de nível 2.
De uma maneira geral, o nível 1 (nível básico de serviço) necessitou apenas de ser consolidado e aperfeiçoado com introdução de alguns procedimentos técnicos e clínicos e protocolos de intervenção em transtornos
minor. A implementação do nível 2, executado pelo farmacêutico residente, focou-se sobretudo na consulta
farmacêutica, com ensino metodológico e em exercício. Trabalhou-se o guião para recolha de informação, as intervenções a prestar e a forma de comunicar com o doente. Todas as consultas e intervenções foram supervisionadas pelo farmacêutico responsável pelo nível 3. Os resultados clínicos, bem como as interven-ções efetuadas, foram registados no processo clínico do doente. Sempre que o problema de saúde não era suscetível de controlo a este nível, o doente era encaminhado para o nível 3 ou, em situações particulares de urgência, para o médico. No que ao nível 3 diz respeito, o serviço era prestado por farmacêutico externo especializado e inteiramente dedicado à prática de acompanhamento farmacoterapêutico.
Fluxogramas de intervenção acerca do modelo e da técnica de recrutamento de doentes foram criados e implementados para auxiliar a equipa.
Resultados e Discussão: A implementação das consultas de acompanhamento farmacoterapêutico, no
ní-vel 3 de serviço, iniciou-se em 2008 e induziu o desenvolvimento do modelo proposto, devido à perceção (adquirida na prática) de que muitos doentes poderiam controlar o seu problema de saúde mediante «sim-ples» intervenções, sem necessidade de estudo específico. Até setembro de 2013 foram acompanhados, por um farmacêutico especializado em acompanhamento farmacoterapêutico, 430 doentes com problemas de saúde recorrentemente não controlados em 20 farmácias comunitárias. Cerca de 3200 consultas farmacêu-ticas foram efetuadas. Os problemas de saúde mais prevalentes foram a dislipidemia, a diabetes e a hiper-tensão arterial. Em virtude da intervenção farmacêutica a este nível, os resultados clínicos disponíveis, para uma farmácia (46 doentes), mostram reduções médias de 26,4±7,68 mg/dL nos níveis séricos de colesterol total (n=28; p=2,510x10-3), 26,2±3,79 mmHg na pressão arterial sistólica (n=23; p=6,197x10-7) e 1,9±0,73% na
15 O acompanhamento farmacoterapêutico desenvolvido por farmacêutico externo à equipa da farmácia já deu
pro-vas da sua aplicabilidade prática e de significativa mais-valia para a saúde do doente. Por isso, este artigo foca-se mais na consulta farmacêutica de nível 2, no enquadramento da aplicação do modelo de três níveis proposto. A consulta farmacêutica de nível 2 iniciou-se em maio de 2012. Nos últimos 16 meses de implementação deste serviço em cinco farmácias comunitárias, 346 doentes foram incluídos. De um total de 516 consultas marcadas, efetuaram-se 371 pelos farmacêuticos residentes das farmácias envolvidas, traduzindo uma taxa de desistência de, aproximadamente, 28 por cento. Diabetes, hipertensão e dislipidemia foram as patologias mais prevalentes. Como resultado das intervenções farmacêuticas direcionadas a estas patologias, os dados disponíveis para 65 doentes revelam reduções médias de 53,3±9,27 mg/dL nos níveis séricos de colesterol total (n=19; p=1,913x10-5), de 18,3±2,26
mmHg na pressão arterial sistólica (n=42; p=4,657x10-10) e de 0,2 por cento na hemoglobina glicada (n=2).
Considerando o curto período de implementação da consulta de nível 2 em comparação com a consulta de nível 3, o número relativamente maior de doentes envolvidos no nível 2 apoia um dos pressupostos do modelo: a maioria dos doentes pode controlar o seu estado de saúde mediante intervenções farmacêuticas «simples» (adesão à tera-pêutica, toma correta, melhoria de hábitos de vida, etc.), sem exigir um estudo pormenorizado como aquele que é feito ao nível 3. Acresce que a altura em que a consulta de acompanhamento farmacoterapêutico começou a ser implementada corresponde a um período em que a cultura de serviço farmacêutico orientado para o doente ainda não estava ao nível que hoje se regista.
Conclusão: O modelo de intervenção farmacêutica diferenciada em três níveis de atuação, baseado nas diferentes
necessidades de saúde dos doentes, parece adequado à implementação da prática de serviços farmacêuticos cog-nitivos na rotina diária da farmácia comunitária. Adicionalmente, através deste modelo, a farmácia responde às diferentes necessidades de saúde dos seus utentes e contribui, de forma significativa, para a melhoria do estado de saúde dos seus doentes.
Palavras-chave: Serviços farmacêuticos cognitivos, modelo de intervenção farmacêutica, consultas de
acompa-nhamento farmacoterapêutico.
Introduction
In order to contribute for the real implementation of pharmaceutical care services in Portugal, a three levels model of pharmacist clinical intervention in the community pharmacy, based on the differenti-ated patient´s health needs, was proposed by the authors. This model is a result of several years deliv-ering pharmacotherapeutic follow-up consultations in Portuguese community pharmacies. In the practi-cal experience, the authors perceived that the major-ity of patients with non-controlled health problems could be controlled through “simple” interventions as medication adherence, medicines’ intake according with the indications or healthy lifestyle habits change, not requiring the specific and personalized study applied by pharmacotherapeutic follow-up. Simul-taneously, several barriers1 has prevented the
imple-mentation of more clinical oriented pharmaceutical services by the community pharmacy.
In theory, through the three levels model the phar-macy answer to all their customer´s health needs, from the “simple” non-controlled health problem (with level 2 pharmaceutical consultation) to a more complicated and recurrent non-controlled clinical situation (with level 3 consultation, the pharmaco-therapeutic follow-up program).
Objective
To test the practical application of the proposed three levels model for differentiated pharmacist clini-cal activities in the community pharmacy.
Methodology
Implementation and development of the three levels model in several community pharmacies, structuring the pharmacist interventions and optimizing human resources, according to patient´s health needs.
A specialized pharmacist in pharmacotherapeutic follow-up, responsible for the level 3 pharmaceutical consultations, introduced the philosophy of the three levels model, in each pharmacy team, supervising its implementation.
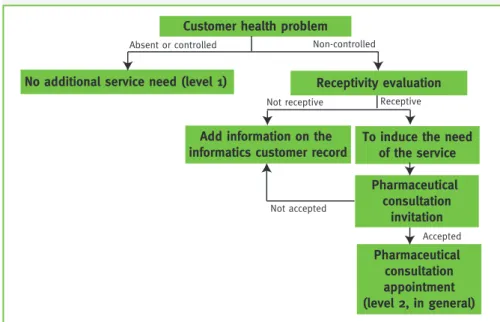
The first change induced was the pharmacist activity focus, changing from the product and its selling to the patient and his health needs. All the pharmacy profes-sionals were instructed to ask the customer about the health problem control (when applicable) and to get the perception of “what the customer needs and what he wants”. This procedure, common to all attendance, was essential for the success of the model implementa-tion. Two situations can be anticipated (Figure 1): - Absence of non-controlled health problem or specific counseling. Dispensing the requested
16
product completes the attendance. This is the level 1 service offered by all the pharmacy professionals.
- Presence of non-controlled health problem or re-quest for specific counseling. The pharmacy
profes-sional should consider the receptivity of the patient to the pharmacist intervention and decide accordingly. If the patient is not receptive this is registered in the informatics patient record. When receptive, the phar-macist evaluates the clinical situation and provides immediate counseling or schedules a pharmaceutical consultation (level 2, in general) to take in account other aspects of the medication or the pathology. In general, at least in Portugal, the concept of phar-maceutical consultations is not common. The patient should first understand his non-controlled health problem and the contribution that the pharmacist could provide to control it. The meeting with the pharmacist is scheduled during the period reserved for the level 2 pharmaceutical consultations. The patient is invited to bring all his medicines, within respective boxes, and the last clinical laboratory test results. The resident pharmacist applies the guidance formulary for level 2 first consultation (see accompa-nying paper).
When the health problem cannot be controlled by “sim-ple” interventions as medication adherence, medicine´s intake according to the indication or lifestyle habits changes, the patient was invited to integrate the level 3 consultations, for more detailed study.
Pharmacotherapeutic follow-up was provided in a patient-centered approach using a logical and
Figure 1 – Flowchart suggested for the professional behavior intervention during first attendance in the Community Pharmacy
methodological reasoning (adapted from Dáder’s method2) to detect, prevent and solve negative
clini-cal outcomes. When all the health problems were solved or no additional interventions were foreseen, the patient was returned for level 2 pharmacist with a detailed written report.
To implement the model in the adherent commu-nity pharmacies, specific formation was offered to the pharmacy team. In general the importance of the concept for changing the focus in the Commu-nity Pharmacy from the product to the patient was the starting point. Teaching of procedures for some health parameters measurements, as blood pressure, respiratory parameters or capillary blood testing and protocols for minor diseases were performed for all
the pharmacy professionals to provide level 1 service. For level 2 service, in particular for the delivering of pharmaceutical consultations, the resident pharma-cist appointed was the target for specific education on communication with the patient, methodology, including specific formularies, and clinical interven-tions to be applied. Weekly there was a personal contact between the resident pharmacist, respon-sible for level 2 pharmaceutical consultations and the specialized pharmacist, responsible for the pharma-cotherapeutic follow-up, usually via “Skype”, to dis-cuss specific clinical and methodological aspects. Level 3 service was provided by the Community Phar-macy through an external specialized pharmacist on pharmacotherapeutic follow-up offering pharmaceu-tical consultations according with clinical needs and
therapeutic objectives of the patients enrolled.
Need for Differentiated Services
In order to evaluate the percentage of pharmacy customers requiring pharma-cist intervention to improve health condition, a brief sur-vey was conducted in 2011. During six random selected days all the attendance events (customers older than 18 years) were analyzed. Based on a specific flowchart each attendance was classified in one of the three service levels, according with the perceived patient´s health needs. At the end of the study, two pharma-Customer health problem
No additional service need (level 1) Receptivity evaluation
Add information on the
informatics customer record To induce the needof the service Pharmaceutical consultation invitation Pharmaceutical consultation appointment (level 2, in general)
Absent or controlled Non-controlled
Not receptive Receptive
Not accepted
17 cists validated all the level classifications
indepen-dently. Questionnaires with divergent evaluation by both pharmacists were excluded from the study. The clinical data presented here was treated using Microsoft Excel™, with t-student tests and
signifi-cance levels of p=0.05.
Results
Level 2 Pharmacist Consultations
From May 2012, the beginning of implementation of the model, to September 2013, about 346 patients was enrolled in the level 2 pharmaceutical consultations. Results from 5 community pharmacies show that during 16 months, 513 pharmaceutical consulta-tions were scheduled, corresponding to an average of 6.4 consultations per month per pharmacy. A drop out rate of about 28 % was registered. From the scheduled consultations only 371 were really per-formed by 5 pharmacists, corresponding to an aver-age of 4.6 consultations per month per pharmacy. Following the first consultation, 76 patients were ap-pointed for a second level 2 consultation, 39 patients were referred to pharmacotherapeutic follow-up (lev-el 3) and 21 to other services offered by the pharma-cies. The remaining 211 patients controlled immedi-ately the health problem, sometimes with additional recommendations outside formal consultations. Diabetes (33.5 %), hypertension (36.1 %), dyslipi-daemia (18.7 %) were the most prevalent pathologies registered at the level 2 service. A total of 963 pharmacist interventions were performed and registered. About 75 % of these interventions were considered as non- -pharmacological (721), with a predominance of life-style modification recommendations, especially healthy eating habits (474 interventions). More than 25 % of the pharmacist interventions were considered pharma-cological (242), with a predominance of recommenda-tions for therapeutic adherence (156 intervenrecommenda-tions). The clinical outcomes achieved by level 2 pharmacist interventions were considered by comparison with the starting point inducing the invitation to the con-sultations. Data on hypertension, diabetes and cho-lesterol levels changes are available for 65 patients. For 42 patients with non-controlled hypertension, pharmacist intervention induced a mean reduc-tion of 18.3±2.26 mmHg on systolic blood pressure (from 153.2 mmHg to 134.9 mmHg; p=4.657x10-10)
and 8.1±1.50 mmHg on diastolic blood pressure (from 80.8 mmHg to 72.7 mmHg; p=2.975x10-6). It was
pos-sible to control 24 patients. Nineteen patients were identified with hypercholesterolemia diagnosed and non-controlled. After pharmacist interventions, total
cholesterol levels registered a mean reduction of 53.3±9.27 mg/dL (from 236.8mg/dL to 183.5 mg/dL; p=1.913x10-5), achieving guideline therapeutic goals
for 10 patients.
The pharmacist interventions on 20 diabetic patients induced mean reductions of 0.2 % in glycated haemo-globin (n=2), 29.9±26.30 mg/dL (from 151.7 mg/dL to 121.8 mg/dL; p=0.285) in fasting glucose (n=10) and 74.2±20.48 mg/dL (from 237.2 mg/dL to 163.0 mg/dL; p=3.511x10-3) in post-prandial blood glucose (n=13).
Pharmacotherapeutic Follow-up – Level 3 Service
Since September 2008 to September 2013, a total of 430 pa-tients with recurrent non-controlled health problems were involved with the specialized pharmacist and more than 3200 pharmaceutical consultations were provided to these patients. The most prevalent diseases registered were dys-lipidemia, diabetes and hypertension. Mean reductions of 26.4±7.68 mg/dL on total cholesterol (n=28; p=2.51x10-3),
1.9±0.73 % on glycated haemoglobin (n=29; p=0.022) and 26.2±3.79 mmHg on systolic blood pressure (n=23; p=6.197x10-7) are attributed to the
pharmaco-therapeutic follow-up, corresponding to significant improvements on patient’s health condition [“A new approach for the implementation of pharmaceutical care”, paper in preparation].
The Quantitative Needs for Differentiated Services
During the period of the survey, 405 attendances were registered, 392 (96.8 %) of them were considered vali-dated by convergent opinions of the two pharmacists. The results shown that the majority of the consum-ers (320) would not require clinical services provided by the pharmacist. Around 81.6 % of attendances, un-related with non-controlled health problems, would be satisfied by level 1 service. Forty-four attendees (around 11.2 %) were evaluated as requiring level 2 service by rapid and simple pharmacist interven-tions for controlling respective health problems. The remaining 28 attendances (around 7.1 %) were con-sidered as requiring specialized intervention of the pharmacist through pharmacotherapeutic follow-up at level 3 service.
Discussion
The practice of pharmacotherapeutic follow-up, ini-tiated in 2008, paved the way for the development of the integrated model presented due to the perception (acquired in the practice) that many patients could control their health problem through “simple” inter-ventions, without specific study. The added value of
18
pharmacotherapeutic follow-up program implemented through an external specialized pharmacist for pa-tient’s health condition is known and documented3.
In the same way, international literature abundantly documents the practice of this service and the posi-tive outcomes for the patient´s health condition4,5.
According to the first results of conSIGUE study, the practice of pharmacotherapeutic follow-up applied to elderly polimedicated patients induced a reduc-tion of 58 % of patient’s health problems, 30 % of emergency visits and 50 % of hospitalizations6.
The new proposal and development of the three levels model and its practical applicability should document the value of the level 2 pharmaceutical consultations in addition to the pharmaceutical care activities, already known. This justifies the main fo-cus of this paper on the results of level 2 consulta-tions.
Most of the non-controlled health problems improved by correcting the errors on medication process use, being the poor adherence the most relevant. The level 2 consultations delivered by the resident pharmacist revealed to be appropriate and sufficient for control-ling these health problems. Interventions at this level are not time consuming and do not require dedicated study due to the supervision and constant support provided by the specialized pharmacist responsible for the level 3 consultations. These level 2 consulta-tions can easily be added to the routine activities of the resident pharmacist.
For refractory patients, with recurrent non-con-trolled health problems, more specialized and time-consuming pharmacist consultations are need, the pharmacotherapeutic follow-up should be applied. On practice the relative small number of patients involved in level 3 consultations (430 patients, 5 years) compared with the data from level 2 consul-tations (346 patients, 1.3 years), support one of the premises of this model: the majority of patient´s health problems could be controlled through “simple” inter-ventions (medication adherence, medicines intake according the indication, healthy lifestyle habits, between others), at level 2. The number of patients requiring specialized service at level 3 is lower. Regarding the clinical outcomes from level 2 con-sultations, with a relative small number of patients with data available, the added value of this consul-tation for patients is clear. Significative reductions in total cholesterol and systolic blood pressure were achieved. For diabetic patients, mean reductions were also registered in glycaemia, but only in post--prandial the values are statistical significant, due to
the small number of patients with data available for fasting glycaemia and glycated haemoglobin.
Considering that the concept of level 2 pharmaceuti-cal consultations is new, the comparison with other results from pharmacist interventions in the litera-ture is difficult. Nevertheless, a systematic review and meta-analysis of 30 randomized trials conducted in 2011, in order to determine the impact of pharmacist care on the management cardiovascular diseases risk factors, concluded that, in spite of some heterogene-ity, the majority of the studies points for a positive impact of the pharmacist intervention. This review shows that the pharmacist’s care induces a mean re-duction of 8.1 mmHg on systolic blood pressure and 17.4 mg/dL on total cholesterol7. The discrepancies
with the three levels model here proposed could be due to different number of patients, studies’ design and the type of pharmacist interventions. In type 2 diabetes, the results of a controlled trial conducted in Brazil showed mean reductions in fasting glycaemia with similar amplitude: 20.1 mg/dL5.
Other different studies have been reported8-10, all of
them showing positive clinical outcomes with differ-ent objective improvemdiffer-ents due to the pharmacist in-tervention to manage non-controlled health problems. This model, to provide differentiated services to the community pharmacy customers, according with their health needs, proved to be viable in practice, present-ing global positive results for the health parameters studied either on the level 2 or level 3 environment. Dif-ferent outcomes from both consultations are the result of pharmacist interventions with different target pa-tients. At level 2 the patients have non-controlled situ-ations due to “simple” causes, while at the level 3 con-sultations the patients are recurrently non-controlled or having complex pharmacotherapeutic profiles. The level 2 consultations implemented in the com-munity pharmacies, where the three levels model was experimented, were previously scheduled for half-a-day per week, while the level 3 consultations were previously scheduled half-a-day every two weeks. These frequencies proved to be adequate for the needs registered and agrees with the brief survey performed, where most of the pharmacy customers did not need clinical interventions, evaluated to be more than 80 %. From the remaining customers that would benefice from pharmacist clinical interven-tion, only around 7 % would require the specialized pharmacotherapeutic follow-up.
Data reported in this paper would require longer implementation of the model for more consolidated results, especially in what concerns the level 2
con-19 sultations. There is a perception that this three levels
model improves loyalty of customers, but additional studies are required to demonstrate this added value for the community pharmacy implementing the model.
Conclusion
The three levels model for differentiated pharma-cist intervention, based on the pharmacy customer´s health needs, seem to be a suitable model for the routine implementation of pharmaceutical care and other cognitive pharmaceutical services in Portu-guese community pharmacies. Based on this model, the Community Pharmacy can answer to all their customer´s health needs and contributes for signifi-cant improvements on patient´s health condition, which rewards them and the pharmacist.
References
1. Gastelurrutia MA, Fernández-Llimos F, Benrimoj SI, Castrillon CC, Faus MJ. Barriers for the Implementation of Cognitive Services in Spanish Community Pharmacies. Aten Primaria. 2007;39(9):465-72.
2. Faus MJ, Amariles P, Martínez-Martínez F. Atención Farmacéutica – conceptos, processos y casosprácticos. Ergon. 2008, ISBN: 978-84-8473-609-7.
3. Cavaco M, Condinho M, Miranda F, Sinogas C. A Farmacoterapia Aplicada a Doentes com Factores de Risco Cardiovascular Modificáveis. O Exercício do Acompanhamento Farmacoterapêutico. Rev Port Farmacoter. 2010 Abr;2(2):79-88. 4. Amariles P, Sabater-Hernández D, García-Jiménez E, Rodríguez-Chamorro MÁ, Prats-Más R, Marín-Magán F, Galón-Ceballos JA, Jiménez-Martín J, Faus MJ. Effectiveness of Dader Method for pharmaceutical care on control of blood pressure and total cholesterol in outpatients with cardiovascular disease or cardiovascular risk: EMDADER-CV randomized controlled trial. J Manag Care Pharm. 2012;18(4):311-23.
5. Correr CJ, Melchiors AC, Fernandez-Llimós F, Pontarolo R. Effects of a pharmacotherapy follow-up in community pharmacies on type 2 diabetes patients in Brazil. Int J Clin Pharm. 2011 Apr;33(2):273-80.
6. Community Pharmacy, the Accessible Local Healthcare Resource. Annual Report 2013. Pharmaceutical Group of European Union. Available on www.pgeu.eu/en/library/1-annual-report/224-annual-report-2013.html (last access 18 April, 2014). 7. Santschi V, Chiolero A, Burnand B, Colosimo AL, Paradis G. Impact of pharmacist care in the management of cardiovascular disease risk factors: a systematic review and meta-analysis of randomized trials. Arch Intern Med. 2011;171(16):1441-53. 8. Isetts BJ, Schondelmeyer SW, Artz MB, Lenarz LA, Heaton AH, Wadd WB, Brown LM, Cipolle RJ. Clinical and economic
outcomes of medication therapy management services: the Minnesota experience. JAPhA. 2008 Mar/Apr;48:2, 203-211. 9. Houle SK, Chuck AW, McAlister FA, Tsuyuki RT. Effect of a pharmacist-managed hypertension program on health system costs: an evaluation of the Study of Cardiovascular Risk Intervention by Pharmacists-Hypertension (SCRIP-HTN). Pharmacotherapy. 2012;32(6):527-37.
10. Bunting SA, Smith BH, Sutherland SE. The Asheville Project: clinical and economic outcomes of a community-based long-term medication therapy management program for hypertension and dyslipidemia. J Am Pharm Assoc. 2008 Jan-Feb;48(1):23-31.
Acknowledgments
The authors would like to thank the community pharmacies, where data reported was acquired: Farmácia Central, Mora, Portugal; Farmácia Paula Santos, Pêra, Portugal; Farmácia Helena, Faro, Portugal; Farmácia Motta, Évora, Portugal; Farmácia Ribeiro Soares, Santa Iria de Azóia, Portugal.
Funding
No funding was received for this work.