www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
CRUSADE:
Is
it
still
a
good
score
to
predict
bleeding
in
acute
coronary
syndrome?
夽
Dina
Bento
a,∗,
Nuno
Marques
a,b,
Pedro
Azevedo
a,
João
Guedes
a,
João
Bispo
a,
Daniela
Silva
a,
José
Amado
a,
Walter
Santos
a,
Jorge
Mimoso
a,
Ilídio
de
Jesus
aaServic¸odeCardiologia,CentroHospitalarUniversitáriodoAlgarve,Faro,Portugal bAlgarveBiomedicalCenter,Faro,Portugal
Received12October2017;accepted1February2018 Availableonline30November2018
KEYWORDS Majorbleeding; Acutecoronary syndrome; CRUSADEbleeding score; In-hospitalprognosis Abstract
Introduction:Majorbleedingisaseriouscomplicationofacutecoronarysyndrome(ACS)and isassociatedwithaworseprognosis.TheCRUSADEbleedingscoreisusedtostratifytheriskof majorbleedinginACS.
Objective: ToassessthepredictiveabilityoftheCRUSADEscoreinacontemporaryACS popu-lation.
Methods:Inasingle-centerretrospectivestudyof2818patientsadmittedwithACS,the CRU-SADE scorewas calculated for eachpatientandits discriminationandgoodnessoffit were assessedbytheareaunderthereceiveroperatingcharacteristiccurve(AUC)andbythe Hosmer-Lemeshowtest,respectively.Predictorsofin-hospitalmajorbleeding(IHMB)weredetermined. Results:TheIHMBratewas1.8%,significantlylowerthanpredictedbytheCRUSADEscore(7.1%, p<0.001).TheincidenceofIHMBwas0.5%intheverylowriskcategory(ratepredictedbythe score3.1%),1.5%inthelowriskcategory(5.5%),1.6%inthemoderateriskcategory(8.6%), 5.5%inthehighriskcategory (11.9%),and4.4%inthevery highriskcategory (19.5%).The predictiveabilityoftheCRUSADEscoreforIHMBwasonlymoderate(AUC0.73).
Thein-hospital mortalityratewas4.0%.Advancedage(p=0.027),femoralvascularaccess (p=0.004),higherheartrate(p=0.047)andticagreloruse(p=0.027)wereindependentpredictors ofIHMB.
Conclusions: TheCRUSADEscore,althoughpresentingsomediscriminatorypower,significantly overestimated the IHMB rate, especially in patients at higher risk. These results question whethertheCRUSADEscoreshouldcontinuetobeusedinthestratificationofACS.
©2018SociedadePortuguesadeCardiologia.PublishedbyElsevier Espa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽 Pleasecitethisarticleas:BentoD,MarquesN,AzevedoP,etal.ScoreCRUSADE---Seráaindaumbomscoreparapreverahemorragia nasíndromecoronáriaaguda?RevPortCardiol.2018;37:889---897.
∗Correspondingauthor.
E-mailaddress:[email protected](D.Bento).
2174-2049/©2018SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE ScoreCRUSADE; Síndromecoronária aguda; Hemorragiamajor; Prognóstico intra-hospitalar
ScoreCRUSADE---Seráaindaumbomscoreparapreverahemorragianasíndrome
coronáriaaguda?
Resumo
Introduc¸ão:Ahemorragiamajor(HM)éumacomplicac¸ãogravedasíndromecoronáriaaguda (SCA)eestáassociadaapiorprognóstico.OscoreCRUSADEpermiteestratificaroriscodeHM naSCA.
Objetivo:AvaliaracapacidadepreditivadoscoreCRUSADEnumapopulac¸ãocontemporâneade SCA.
Métodos: Estudounicêntrico e retrospetivo com 2.818 doentesadmitidos porSCA. Oscore CRUSADEfoicalculadoparacadadoente,asuadiscriminac¸ãoecalibrac¸ãoforamavaliadaspela áreaabaixodacurva(AUC)ReceiverOperatingCharacteristicepelotesteHosmer-Lemeshow, respetivamente.ForamdeterminadosospreditoresdeHMintra-hospitalar(HMIH).
Resultados: A taxade HMIHfoi de 1.8%,valor significativamente inferiorao estimadopelo scoreCRUSADE(7,1%,p<0,001).AincidênciadeHMIHnasdiferentescategoriasfoide0,5%na demuitobaixorisco(taxaestimadapeloscorede3,1%);1,5%nadebaixo(estimadade5,5%); 1,6%nademoderado(estimadade8,6%);5,5%nadeelevado(estimadade11,9%)e4,4%nade muitoelevado(estimadade19,5%).AcapacidadepreditoradoscoreCRUSADEparaHMIHfoi apenasmoderada(AUC0,73).Ataxademortalidadeintra-hospitalarfoide4,0%.Aidademais avanc¸ada(p=0,027),oacessovascularfemoral(p=0,004),afrequênciacardíacamaiselevada (p=0,047)eoticagrelor(p=0,027)forampreditoresindependentesdeHMIH.
Conclusão:OscoreCRUSADE,apesardeapresentaralgumpoderdiscriminatório,sobrestimou deformasignificativaataxadeHMIH,principalmentenosdoentesdemaiorrisco.Esses result-adosquestionamseoscoreCRUSADEdeverácontinuaraserusadonaestratificac¸ãodaSCA. ©2018SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Listofabbreviations
ACS acutecoronarysyndrome AUC areaunderthecurve
CABG coronaryarterybypassgrafting CI confidenceinterval
COPD chronicobstructivepulmonarydisease GP glycoprotein
IHMB in-hospitalmajorbleeding LVEF leftventricularejectionfraction MI myocardialinfarction
OR oddsratio
PCI percutaneouscoronaryintervention
Introduction
Patientswithacutecoronarysyndrome(ACS)area hetero-geneouspopulation, withvarying levelsofriskfor events, andsoinitialassessmenthasacrucialroleindecidingthe mostappropriatetherapeuticstrategy.1Treatmentofthese
patientsincludes antithrombotictherapyandinvasive pro-cedures, which carry an increased risk of bleeding,2 the
incidenceofwhichrangesbetween1%and10%.3This
vari-abilityintheincidenceofbleedingcomplicationsisdueto
variousfactors,includingdifferencesinpatient character-istics,concomitanttreatmentanddefinitionsofbleeding.3
Nevertheless,whateverdefinitionisused,multiple studies haveshownthatbleedingcomplicationsareassociatedwith adverseeventsincludingdeath,non-fatalmyocardial infarc-tion(MI),stroke,andstentthrombosis.3---5
Assessment of the risk of bleedingincludes a detailed historyofbleedingsymptoms,identificationofpredisposing comorbidities,laboratorydata,andcalculationofableeding riskscore.6
The CRUSADE score7 was developed to assess
bleed-ing risk based on a varied population of patients with non-ST-elevationACS(NSTE-ACS),andwassubsequently val-idated for ST-elevation myocardial infarction (STEMI).8 It
is calculated from eight variables that include baseline characteristics,clinical variablesandadmissionlaboratory values.7 It is currently the most commonly usedscore to
determine bleeding risk, due to itsproven discriminatory power.6,9,10
The main purpose of the CRUSADE score is to strat-ify bleeding risk in patients with ACS, in order to select appropriatetherapeuticstrategiesthatwillreducebleeding eventsandhenceimproveprognosis.9
The aimof thisstudy is toanalyzetheapplicability of theCRUSADEscoreinACSpatients,inlightofthesignificant changesthathavetakenplaceoverthelastdecadeinthe managementandtreatmentofthesepatients.
Methods
Studydesign
Thiswasaretrospective,descriptive,correlationalstudyof patientsadmittedwithadiagnosisofACStothecardiology department of Centro Hospitalar Universitário do Algarve between October 1, 2010 andAugust 31, 2014. The CRU-SADEscorewascalculatedfor eachpatientand itsability topredict in-hospitalmajorbleeding(IHMB)wasassessed. PredictorsofIHMBweredetermined.
Patientselection
Atotalof2818patientsdiagnosedwithACSintheprevious 48hourswereincluded. MIwasdiagnosedinthepresence ofchestpainoranginalequivalentintheprevious48hours together with ischemic electrocardiographic changes (ST-segment deviation or negative T waves) and elevation of troponinlevelsabovethereferencevalue.Unstableangina wasdefinedasthepresenceofchestpainoranginal equiv-alent with or without with ischemic electrocardiographic changesintheabsenceofelevationoftroponinlevelsabove thereferencevalue.
Patients withMI associated withrevascularization pro-cedures (types 4 and 5) or type 2 MI according to theESC/ACCF/AHA/WHFuniversaldefinitionofmyocardial infarction11wereexcluded.
IntheanalysisofthepredictiveabilityoftheCRUSADE score,203ofthe2818patients(7.2%)wereexcludeddueto inabilitytocalculatethescore.
Datacollection
Data were collected on demographics (age and gender), relevant personal history (MI, heart failure,percutaneous coronary intervention [PCI], coronary artery bypass graft surgery,chronicobstructivepulmonarydisease[COPD]and cancer),andcardiovascularriskfactors(hypertension, dia-betes, dyslipidemia and smoking status). Data were also analyzedonhospitalstay,includingclinicalparametersat admission(systolic blood pressure, heart rateand hemat-ocrit),coronaryangiography(vascularaccessandPCI),left ventricular ejection fraction (LVEF), type of ACS (STEMI, non-ST-segmentMI[NSTEMI],MIofundeterminedlocation, or unstable angina), and medication (aspirin, clopidogrel, ticagrelor, enoxaparin, unfractionated heparin, warfarin, andglycoprotein[GP]IIb/IIIainhibitors).
Creatinine clearance was estimated by the Cockcroft-Gaultformula.12
Vasculardiseasewasidentifiedonthebasisofahistory ofperipheralarterialdiseaseand/orstroke.
In-hospitalmortalitywasdefinedasdeathfromanycause duringhospitalizationforACS.
Studyobjectives
The study objectives were assessment of the predictive abilityoftheCRUSADEscoreforin-hospitalmajorbleeding
(IHMB) and determination of independent predictors of IHMB.
IHMBwasdefinedaccordingtotheGUSTOclassificationas intracerebralbleedingorbleedingresultinginhemodynamic compromiserequiringtreatment.13TheCRUSADEscorewas
calculatedfromeightvariables(baselinehematocrit, esti-matedcreatinine clearance, baselineheart rate,baseline systolicbloodpressure,gender,signsofheartfailureon pre-sentation, prior vascular disease, and diabetes). The five bleedingriskcategoriesdefinedbytheCRUSADE investiga-torswereused:verylowrisk(score≤20),lowrisk(21-30), moderaterisk(31-40),highrisk(41-50),andveryhighrisk (>50).
Statisticalanalysis
A descriptiveanalysis was performed to characterize the studysample. Continuousvariablesarepresentedasmean ±standard deviation andcategorical variablesasnumber (percentage).
ThepredictiveabilityoftheCRUSADEscoreinour pop-ulationwastestedusingtheareaunderthecurve(AUC)on receiveroperatingcharacteristicanalysis14andthemodel’s
goodness of fit was assessed by the Hosmer-Lemeshow test,15 inwhich adequategoodness offitisindicated bya
non-significantpvalue.
Associations between categorical variables were ana-lyzed using the chi-square test and continuous variables usingtheStudent’sttest.
Binarylogisticregressionanalysiswasusedtodetermine predictors of IHMB.A p-valueof <0.05 wasconsidered to indicatea95%significancelevel.IBMSPSSStatistics(version 20.0)wasusedforthestatisticalanalysis.
Results
Populationcharacteristics
Thebaselinecharacteristicsofthestudypopulationare pre-sentedinTable1.
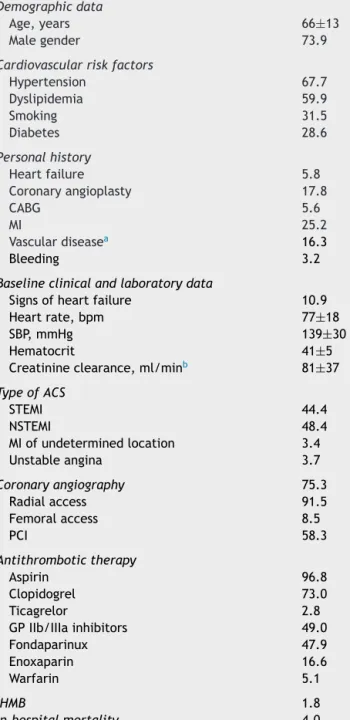
Atotalof2818ACSpatientswereincluded,73.9%male, meanage66±13years.Atadmission,meanhematocritwas 41±5%, mean heart rate was 77±18 bpm, mean systolic bloodpressurewas139±30mmHg,meancreatinine clear-ancewas81±37ml/min,and10.9%presentedsignsofheart failure.
The most frequent diagnosis at admission was NSTEMI (48.4%),followed bySTEMI (44.4%).Coronaryangiography wasperformedin75.3%ofpatients(91.5%byradialaccess), and58.3%underwentPCI.
Withregardtoantithrombotictherapyduring hospitaliza-tion,96.8%ofthepatientsreceivedaspirin,73%clopidogrel, 2.8%ticagrelorand47.9%fondaparinux.
During hospital stay, 113 (4.0%) patients died and 52 (1.8%)presentedIHMB.
DiscriminatorypoweroftheCRUSADEscore
TherateofIHMBpredictedinthestudypopulationwas7.1%, whiletheobservedratewas1.8%,astatisticallysignificant difference(p<0.001)(Table2).
Table1 Baselinecharacteristicsofthe study population (n=2818).
Demographicdata
Age,years 66±13
Malegender 73.9
Cardiovascularriskfactors
Hypertension 67.7 Dyslipidemia 59.9 Smoking 31.5 Diabetes 28.6 Personalhistory Heartfailure 5.8 Coronaryangioplasty 17.8 CABG 5.6 MI 25.2 Vasculardiseasea 16.3 Bleeding 3.2
Baselineclinicalandlaboratorydata
Signsofheartfailure 10.9
Heartrate,bpm 77±18
SBP,mmHg 139±30
Hematocrit 41±5
Creatinineclearance,ml/minb 81±37 TypeofACS STEMI 44.4 NSTEMI 48.4 MIofundeterminedlocation 3.4 Unstableangina 3.7 Coronaryangiography 75.3 Radialaccess 91.5 Femoralaccess 8.5 PCI 58.3 Antithrombotictherapy Aspirin 96.8 Clopidogrel 73.0 Ticagrelor 2.8 GPIIb/IIIainhibitors 49.0 Fondaparinux 47.9 Enoxaparin 16.6 Warfarin 5.1 IHMB 1.8 In-hospitalmortality 4.0
ACS:acutecoronarysyndrome;CABG:coronaryarterybypass graft surgery; GP: glycoprotein; IHMB: in-hospital major bleeding;MI:myocardial infarction;NSTEMI:non-ST-elevation myocardialinfarction;PCI:percutaneouscoronaryintervention; SBP: systolicblood pressure; STEMI: ST-elevation myocardial infarction.Dataare presentedasmean ± standarddeviation oraspercentage.
aDefinedasperipheralarterialdiseaseorpreviousstroke. b EstimatedbytheCockcroft-Gaultformula.
Table2 In-hospitalmajorbleedingobservedinthestudy populationandpredictedbytheCRUSADEscore.
Observed, n(%) Predictedbythe CRUSADEscore,% p IHMB 52(1.8) 7.1 <0.001
IHMB:in-hospitalmajorbleeding.
TheincidenceofIHMBinthedifferentcategoriesofthe CRUSADEscorewas0.5%intheverylowriskcategory(rate predictedbythescore3.1%),1.5%inthelowriskcategory (5.5%),1.6%inthemoderateriskcategory(8.6%),5.5%inthe highriskcategory(11.9%),and4.4%inthehighriskcategory (19.5%)(Table3).
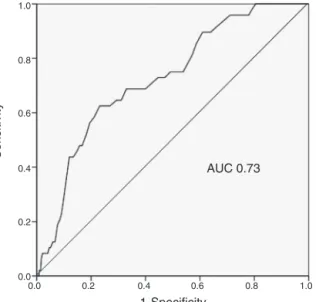
ThepredictiveabilityoftheCRUSADEscoreinthestudy populationwasmoderate,withanAUCof0.73(Figure1).
Predictorsofin-hospitalmajorbleeding
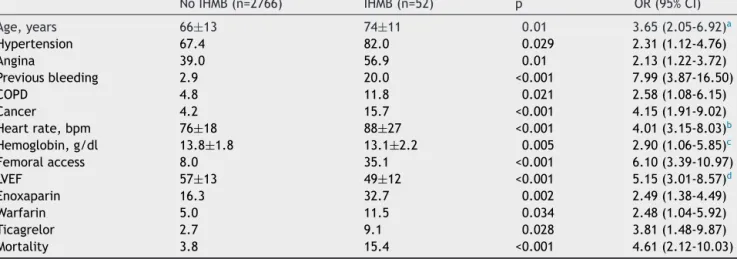
The occurrence of IHMB was associated with the fol-lowing variables: advanced age (p=0.01), hypertension (p=0.029), angina (p=0.01), previous bleeding (p<0.001), COPD (p=0.021), cancer (p<0.001), higher baseline heart rate(p<0.001),lowerhemoglobin(p=0.005),femoralaccess (p<0.001),andlowerLVEFatdischarge(p<0.001).IHMBwas alsoassociatedwithhigherin-hospitalmortality(15.4%vs. 3.8%;p<0.001)(Table4).
When the above significant associations were included in multivariate analysis,advanced age (p=0.027), femoral access (p=0.004), higher heart rate (p=0.047) and medi-cation withticagrelorduring hospitalstay (p=0.027)were identifiedasindependentpredictorsofIHMB(Table5).
Discussion
Inthis contemporarypopulationof patientswithACS, the CRUSADEscoreoverestimatedtheriskofIHMB.
In-hospitalmajorbleeding
The incidenceofIHMBintheliteratureis1-10%;this vari-ability is due to various factors including differences in patientcharacteristics,concomitanttherapyanddefinitions ofbleeding.3
The rateof IHMB inour study was1.8%. This is signif-icantly lower than that predicted by the CRUSADE score (7.1%)(p<0.001).TheCRUSADEscoreoverestimated bleed-ing risk in all risk categories, withgreater differences in higherriskcategories(moderate,highandveryhigh).
These findings may beexplained by evidence that the rateofIHMBinpatientswithACShasdecreasedovertime, despite the use of more aggressive drug therapies and interventions.Foxetal.reportedasignificantfallin bleed-ing rates in patients with ACS between 2000 and 2007, from2.6%to1.8%(p<0.001).16 Factorscontributingtothis
decrease includeimprovements in cardiaccatheterization techniques, theintroductionofsmaller catheters,theuse
Table3 In-hospitalmajorbleedingobservedinthestudypopulationandpredictedbytheCRUSADEscoreaccordingtoCRUSADE riskcategories.
Bleedingrisk n=2615 ObservedIHMB,n(%) IHMBpredictedbytheCRUSADEscore,%
Verylow(1-20) 931 5(0.5) 3.1
Low(21-30) 681 10(1.5) 5.5
Moderate(31-40) 509 8(1.6) 8.6
High(41-50) 289 16(5.5) 11.9
Veryhigh(>50) 205 9(4.4) 19.5
IHMB:in-hospitalmajorbleeding.
AUC 0.73 1-Specificity 0.0 0.0 0.2 0.2 0.4 0.4 0.6 0.6 0.8 0.8 1.0 1.0 Sensitivity
Figure1 Receiveroperatingcharacteristiccurveofthe CRU-SADE score for predicting in-hospital major bleeding in our population.
ofradialaccess,betterselectionofantithrombotictherapy andchangestothresholdsforredbloodcelltransfusion.16
PatientswithIHMBhaveaworseprognosis,withgreater riskforin-hospitalmortality.16,17InastudybySpenceretal.
of40087patientswithMI,IHMBwasassociatedwithgreater mortality(21%vs.6%,p<0.001).17IHMBwasalsoassociated
withhighermortalityinourstudy(15.4%vs.3.8%,p<0.001). Measuresmustbetakentoreduce thenegativeimpactof IHMBonprognosisinACS.However,severalriskfactorsfor bleedingarealsopredictorsofischemicevents, complicat-ingthetaskofmaximizinganti-ischemiceffectivenesswhile minimizingbleedingrisk.7,10
DiscriminatorypoweroftheCRUSADEscore
The ability of the CRUSADE score to predict IHMB in our populationwasacceptable,withanAUCof0.73.However, thisishardlyanoptimalresult.Inacohortof4500patients withACS,Abu-Assietal.assessedtheperformanceof the CRUSADE score,findingac-statistic of0.80 forpredicting majorbleedingevents,9and similarly,Manzano-Fernández
etal.calculatedanAUCof0.79inastudyof1587patients withACS.1However,otherstudieshavereportedlower
fig-ures: the AUC was0.70 in a study of 1976 patients with
ACS by Ariza-Solé et al.,18 while Amador et al. found an
AUCof0.61intheirpopulationof516ACS patients.19 The
CRUSADE score has been shown to have poor predictive ability,withAUCvaluesbelow 0.70,incertainsubgroups, including those aged over 75 years, those who have not undergone coronary angiography, and those not receiving anticoagulant therapy.9,20,21 Its performance was actually
rathermodest (AUC 0.68) in the population in which the scorewasdeveloped.7
There is thus considerable variability in the discrimi-natorypower of the CRUSADE score in ACS patients. This maybeduetoarangeoffactorsthathinderassessmentof bleedingrisk,includingage,comorbidities,antithrombotic therapy,choiceof strategy(invasiveorconservative),and siteofvascularaccessforangiography.Thereisaneedfor ascorethatissuitableforcurrentclinicalpracticeandthat can provide accurate, individualized and simple bleeding riskstratificationinpatientswithACS.
Predictorsofin-hospitalmajorbleeding
TheindependentpredictorsofIHMBidentifiedinourstudy wereadvancedage,higherheartrateonadmission,femoral accessandmedicationwithticagrelorduringhospitalstay.
As pointed outabove,patients withACS are a hetero-geneouspopulation,whichmeansthatdifferentpredictors ofmajorbleedingwillbefoundindifferentpatient popu-lations. A study by Mehran et al. in 17421 patients with ACSidentifiedsevenpredictorsofbleeding,includingfemale gender,advancedage,elevatedserumcreatinine,whitecell count, anemia and use of unfractionated heparin plus a GPIIb/IIIa inhibitor.22 Moscucci et al. determined female
gender, advanced age, renal insufficiency and history of bleeding as independent predictors of bleeding among 24045 ACS patients in the GRACE registry.23 As well as
age,femalegender andrenalinsufficiency,Nikolsky etal. identifiedpre-existinganemia,administrationoflow molec-ular weight heparin within 48 hours pre-PCI, and use of intra-aorticballoonpumpaspredictorsofmajorbleeding.24
Althoughtherearedifferencesbetweenthesestudiesinthe incidence and definitionof bleeding, age, female gender andrenalfailurearefrequentlyidentifiedvariables.2,22,23In
ourstudy,ticagrelorusewasapredictorofIHMB,although itshouldbeborneinmindthatonly2.8%ofourpopulation weretakingthedrug.InthePLATOtrial,comparedto clopid-ogrel,treatmentwithticagrelorreducedvascularmortality, MIandstroke,butwasassociatedwithahigherrateof
bleed-Table4 Variablesassociatedwithin-hospitalmajorbleeding.
NoIHMB(n=2766) IHMB(n=52) p OR(95%CI)
Age,years 66±13 74±11 0.01 3.65(2.05-6.92)a Hypertension 67.4 82.0 0.029 2.31(1.12-4.76) Angina 39.0 56.9 0.01 2.13(1.22-3.72) Previousbleeding 2.9 20.0 <0.001 7.99(3.87-16.50) COPD 4.8 11.8 0.021 2.58(1.08-6.15) Cancer 4.2 15.7 <0.001 4.15(1.91-9.02) Heartrate,bpm 76±18 88±27 <0.001 4.01(3.15-8.03)b Hemoglobin,g/dl 13.8±1.8 13.1±2.2 0.005 2.90(1.06-5.85)c Femoralaccess 8.0 35.1 <0.001 6.10(3.39-10.97) LVEF 57±13 49±12 <0.001 5.15(3.01-8.57)d Enoxaparin 16.3 32.7 0.002 2.49(1.38-4.49) Warfarin 5.0 11.5 0.034 2.48(1.04-5.92) Ticagrelor 2.7 9.1 0.028 3.81(1.48-9.87) Mortality 3.8 15.4 <0.001 4.61(2.12-10.03)
CI:confidenceinterval;COPD:chronicobstructivepulmonarydisease;IHMB:in-hospitalmajorbleeding;LVEF:leftventricularejection fraction;OR:unadjustedoddsratio.Dataarepresentedasmean±standarddeviationoraspercentage.
aForeachadditional5years. b Foreachadditional5bpm. c Foreachreductionof0.5g/dl. d Foreachreductionof5%.
Table5 Predictorsofin-hospitalmajorbleeding.
p OR(95%CI)
Age 0.027 4.89(3.01-7.13)
Heartrate 0.047 3.95(1.87-8.10)
Femoralaccess 0.004 8.29(5.01-10.18)
Ticagrelor 0.027 4.92(1.89-8.15)
CI:confidenceinterval;OR:adjustedoddsratio.
ingnotrelatedtocoronaryarterybypassgraftsurgery(4.5% vs.3.8%;p=0.03).25
Vascularaccessforcoronaryangiography
Inourstudy,91.5%ofpatients underwentangiographyvia radial access, a higher proportion than in other studies assessing the applicability of the CRUSADE score, which reportedratesbetween64%and83.1%.1,9,18,26In
multivari-ateanalysis,femoralaccesswasanindependentpredictor of IHMB (p=0.004), which is in line with recent clinical evidence.27,28 However, when interpreting this result it
shouldbe bornein mind thatfemoral accesswas usedin only8.5%ofpatients.
Periproceduralmajorbleedingisacomplicationthatcan affect patients undergoing PCI, withan incidence of 1.7-3.5%inrecentstudies.29---31Multiplestudieshaveshownthat
radialaccessisassociatedwithlowerratesofperiprocedural bleedingthanfemoralaccess.32---35
The RIVAL trial reported a lower rate of major vas-cular complications for radial access in patients with ACS (1.4% vs. 3.7%; p<0.0001).35 However, results for
mortality were inconsistent, with lower mortality in patientswithSTEMIbutnotinthosewithnon-ST-elevation
ACS(NSTE-ACS).IntheMATRIXtrial,radialaccessreduced bleedingcomplicationsandoverallmortalityinpatientswith ACS (STEMIandNSTEMI) comparedtofemoral access.27 In
theEuropeanguidelinestheuseofradialaccessisaclassI recommendation,levelofevidenceA.10
Thehighrateofradialaccessinourstudymayhave con-tributedtothelowrateofIHMBinourpopulation.Thefact thataccesstypeisnotincludedinitsparametersconstitutes alimitationoftheCRUSADEscore.
Fondaparinux
Regardinganticoagulation,fondaparinuxwasusedin47.9% of our population, considerably more than enoxaparin (16.6%).
In the OASIS-5 trial in patients with NSTE-ACS, fon-daparinux significantly reduced major bleeding events compared to enoxaparin(p<0.001).36 Fondaparinux is the
parenteral anticoagulant recommended in the current guidelines for NSTE-ACS patients, due to its safety and efficacy profile.10 Despite this recommendation, rates of
fondaparinuxuseinotherseriesarelowerthaninours (1.6-14%).1,9,37
Webelievethattheuseofthisanticoagulantinour pop-ulationmayalsohavecontributedtothelowrateofIHMB.
GlycoproteinIIb/IIIainhibitorsandP2Y12 receptor
inhibitors
GP IIb/IIIa inhibitors wereused in 49% of our population, a higher rate than in other series (5.7-40.2%).1,9,18,19,37 It
should,however,benotedthatinmostcasesthisconsisted onlyoftheadministrationofabolusofeptifibatideduring
coronaryangiographyandthatthedrugwasnotinfusedafter angioplasty,whichmayhavecontributedtoourlowrateof periproceduralbleedingcomplications.
There is evidence that in patients with NSTE-ACS undergoing PCI, GP IIb/IIIa inhibitors reduce ischemic events, mainly reinfarction, although they also increase bleeding.6,38
Following the HORIZONS-AMI trial, which showed that anticoagulation with bivalirudin alone was superior to heparin plus GP IIb/IIIa inhibitors in patients undergoing primary PCI, with significantly reduced 30-day rates of majorbleedingandmortality,39useofGPIIb/IIIainhibitors
declined.The current EuropeanguidelinesrecommendGP IIb/IIIainhibitorsonlyforbailoutorincasesofthrombotic complications(classIIarecommendation,levelofevidence C).10,40
Bycontrast,theUSguidelines6statethatinpatientswith
NSTE-ACSandhigh-riskfeaturesnotadequatelypretreated withclopidogrelorticagrelor,itisusefultoadministeraGP IIb/IIIainhibitor(classIrecommendation,levelofevidence A),and in NSTE-ACS patients treated withunfractionated heparin andadequately pretreated withclopidogrel, it is reasonable to administer a GP IIb/IIIa inhibitor (class IIa recommendation,levelofevidenceB).
Itshouldbenotedthatourpatientspreferablyreceived aP2Y12receptorinhibitorduringorafterangioplasty,which
mayalsohavecontributedtothelowrateofmajorbleeding. Currentguidelines recommendpretreatment with aP2Y12
receptor inhibitor for patients with ACS.6,10,40 However,
questionshavebeenraised41,42concerningpretreatmentin
NSTE-ACS, such asby the ACCOAST trial,42 which
demon-stratedthatpretreatmentwithprasugreldidnotreducethe rateofischemicevents,butdidincreasetherateofmajor bleeding.
Clinicalimplications
Antithrombotictherapy,whichisan essentialpartof anti-ischemic therapy in ACS, also increases bleeding risk. PatientswithACSareahighlyheterogeneouspopulationand stratification ofbothischemic andbleedingrisk isneeded in ordertoinstitute appropriatetherapy withthedesired efficacywhile minimizingundesiredeffects.31 However,in
thelasttenyearstherehavebeensignificantchangesinthe managementandtreatmentofACSpatientsthatmayhave alteredthepredictivevalueof riskscores.10 Thereisthus
aneedtodeveloptoolstostratifybleedingriskthataimto promotestrategiesthatreducebleedingratesandthereby improveprognosisinthesepatients.9
Limitations
Thiswasasingle-center,retrospective,observationalstudy, andwasthussubjecttotheinherentbiasesofsuchstudies. The low rate ofbleeding events mayhave influenced the results,whichshouldbevalidatedinalargerpatientcohort. The use of different definitions of major bleeding is another limitation of our study. In the CRUSADE trial, major bleeding was defined as intracranial hemorrhage, documentedretroperitoneal bleed,hematocrit drop≥12% (baseline to nadir), any red blood cell transfusion when
baseline hematocrit ≥28%, or any red blood cell trans-fusion when baseline hematocrit <28% with witnessed bleed. In our study the GUSTO classification was used, whichdefinesmajorbleedingasintracerebral bleedingor bleeding resulting in hemodynamic compromise requiring treatment.13
Conclusions
TheIHMBrateinourstudywas1.8%.The CRUSADEscore, althoughpresentingsomediscriminatorypower,significantly overestimatedtheIHMBrate,especiallyinpatientsathigher risk. These results question whether the CRUSADE score shouldcontinuetobeusedinthestratificationofbleeding riskinACSandwhetherspecificmeasuresshouldbetaken onthebasisofthescoreresult.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.Manzano-FernándezS,Sánchez-MartínezM,Flores-BlancoPJ, etal.Comparisonoftheglobalregistryofacutecoronaryevents riskscore versus thecanrapidriskstratificationof unstable anginapatientssuppressadverse outcomeswithearly imple-mentation of the ACC/AHA guidelines risk score to predict in-hospitalmortalityandmajorbleedinginacutecoronary syn-dromes.AmJCardiol.2016;117:1047---54.
2.StegPG,HuberK,AndreottiF,etal.Bleedinginacutecoronary syndromesand percutaneouscoronaryinterventions:position paperbytheWorking Groupon ThrombosisoftheEuropean SocietyofCardiology.EurHeartJ.2011;32:1854---64.
3.MehranR,RaoSV,BhattDL,etal.Standardizedbleeding def-initions for cardiovascular clinicaltrials: a consensus report fromtheBleedingAcademicResearchConsortium.Circulation. 2011;123:2736---47.
4.Eikelboom JW, Mehta SR, Anand SS, et al. Adverse impact ofbleedingonprognosisinpatientswithacutecoronary syn-dromes.Circulation.2006;114:774---82.
5.RaoSV,O’GradyK,PieperKS,etal.Impactofbleeding sever-ityonclinicaloutcomesamong patientswithacutecoronary syndromes.AmJCardiol.2005;96:1200---6.
6.AmsterdamEA,WengerNK,BrindisRG,et al.2014AHA/ACC Guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the Amer-ican College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64: e139---228.
7.SubherwalS,Bach RG,ChenAY,etal.Baselineriskofmajor bleeding in non-ST-segment-elevation myocardial infarction: theCRUSADE(CanRapidriskstratificationofUnstableangina patients Suppress Adverse outcomes withEarly implementa-tionoftheACC/AHAGuidelines) BleedingScore.Circulation. 2009;119:1873---82.
8.Ariza-SoléA,Sánchez-ElviraG,Sánchez-SaladoJC,etal. CRU-SADEbleeding riskscore validation for ST-segment-elevation myocardialinfarctionundergoing primarypercutaneous coro-naryintervention.ThrombRes.2013;132:652---8.
9.Abu-AssiE,Raposeiras-RoubinS,LearP,etal.Comparingthe predictivevalidityofthreecontemporarybleedingriskscores inacutecoronarysyndrome.EurHeartJAcuteCardiovascCare. 2012;1:222---3.
10.Roffi M,Patrono C,ColletJP, etal. 2015 ESCGuidelines for themanagementofacutecoronarysyndromesinpatients pre-senting without persistent ST-segment elevation: TaskForce fortheManagementofAcuteCoronarySyndromesinPatients Presenting without Persistent ST-Segment Elevation of the European SocietyofCardiology (ESC). Eur HeartJ. 2016;37: 267---315.
11.ThygesenK, AlpertJS, WhiteHD,JointESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Eur Heart J. 2007;28:2525---38.
12.Cockcroft DW, Gault MH. Prediction ofcreatinine clearance fromserumcreatinine.Nephron.1976;16:31---41.
13.The GUSTO investigators. An international randomized trial comparing fourthrombolytic strategiesfor acutemyocardial infarction.NEnglJMed.1993;329:673---82.
14.HanleyJA,McNeilBJ.Themeaninganduseoftheareaunder a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29---36.
15.LemeshowS,Hosmer D.Areviewofgoodnessoffitstatistic foruseinthedevelopmentoflogisticregressionmodels.AmJ Epidemiol.1982;115:92---106.
16.FoxK,CarruthersK,StegG,etal.Hasthefrequencyofbleeding changedovertimeforpatientspresentingwithanacute coro-narysyndrome?TheGlobalRegistryofAcuteCoronaryEvents. EurHeartJ.2010;31:667---75.
17.Spencer FA, Moscucci M, Granger CB, et al. Does comor-bidity account for the excess mortality in patients with major bleeding in acute myocardial infarction? Circulation. 2007;116:2793---801.
18.Ariza-Solé A, Salazar-Mendiguchía J, Lorente V, et al. Predictive abilityofbleeding riskscores in theroutine clin-ical practice. Eur Heart J Acute Cardiovasc Care. 2015;4: 205---10.
19.AmadorP,SantosJF,Gonc¸alvesS,etal.Comparisonofischemic and bleeding risk scores in non-STelevation acutecoronary syndromes.AcuteCardCare.2011;13:68---75.
20.Faustino A, Mota P, Silva J, et al. Non-ST-elevation acute coronary syndromes in octogenarians: applicability of the GRACE and CRUSADE scores. Rev Port Cardiol. 2014;33: 617---27.
21.Ariza-SoléA,FormigaF,LorenteV,etal.Efficacyofbleeding riskscoresinelderlypatientswithacutecoronarysyndromes. RevEspCardiol.2014;67:463---70.
22.MehranR,PocockSJ,NikolskyE,etal.Ariskscoretopredict bleedinginpatientswithacutecoronarysyndromes.JAmColl Cardiol.2010;55:2556---66.
23.Moscucci M, Fox KA, Cannon CP, et al. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2003;24: 1815---23.
24.Nikolsky E, Mehran R, Dangas G, et al. Development and validation of a prognostic risk score for major bleeding in patients undergoing percutaneous coronary interven-tion via the femoral approach. Eur Heart J. 2007;28: 1936---45.
25.WallentinL,BeckerRC,BudajA,etal.Ticagrelorversus clopid-ogrelinpatientswithacutecoronarysyndromes.NEnglJMed. 2009;361:1045---57.
26.Flores-RíosX,Couto-MallónD,Rodríguez-GarridoJ,etal. Com-parisonoftheperformanceoftheCRUSADE,ACUITY-HORIZONS, andACTIONbleedingriskscoresinSTEMIundergoingprimary PCI: insights from a cohort of 1391 patients. Eur Heart J. 2013;2:19---26.
27.ValgimigliM,GagnorA,CalabróP,etal.Radialversusfemoral accessinpatientswithacutecoronarysyndromesundergoing invasivemanagement:arandomisedmulticentretrial.Lancet. 2015;385:2465---76.
28.Vranckx P, Frigoli E, Rothenbühler M, et al. Radial versus femoral access in patients with acute coronary syndromes withorwithoutST-segment elevation.EurHeartJ.2017;38: 1069---80.
29.FeitF,VoeltzMD,AttubatoMJ,etal.Predictorsandimpactof majorhemorrhageonmortalityfollowingpercutaneous coro-nary intervention from the REPLACE-2 Trial. Am J Cardiol. 2007;100:1364.
30.Doyle BJ, Ting HH, Bell MR, et al. Major femoral bleeding complicationsafterpercutaneouscoronaryintervention: inci-dence,predictors, and impact on long-termsurvival among 17,901patientstreatedattheMayoClinicfrom1994to2005. JACCCardiovascInterv.2008;1:202.
31.Chhatriwalla AK, Amin AP, Kennedy KF, et al. Association betweenbleedingeventsand in-hospitalmortalityafter per-cutaneouscoronaryintervention.JAMA.2013;309:1022.
32.SciahbasiA, PristipinoC,Ambrosio G, etal. Arterial access-site-relatedoutcomesofpatientsundergoinginvasivecoronary proceduresforacutecoronarysyndromes(fromthe ComPaR-isonofEarlyInvasiveandConservativeTreatmentinPatients WithNon-ST-ElevationAcuteCoronarySyndromes[PRESTO-ACS] VascularSubstudy).AmJCardiol.2009;103:796---800.
33.RomagnoliE,Biondi-ZoccaiG, SciahbasiA,et al.Radial ver-susfemoralrandomizedinvestigationinST-segmentelevation acute coronary syndrome: the RIFLESTEACS (Radial Versus FemoralRandomizedInvestigationinSTElevationAcute Coro-narySyndrome)study.JAmCollCardiol.2012;60:2481---9.
34.Généreux P, Mehran R, Palmerini T, et al. Radial access in patients with ST-segment elevation myocardial infarction undergoingprimaryangioplastyinacutemyocardialinfarction: theHORIZONS-AMItrial.EuroIntervention.2011;7:905---16.
35.JollySS,YusufS,CairnsJ,etal.,RIVALtrialgroup.Radial ver-susfemoralaccessforcoronaryangiographyandinterventionin patientswithacutecoronarysyndromes(RIVAL):arandomised, parallelgroup,multicentretrial.Lancet.2011;377:1409---20.
36.YusufS,MehtaSR,ChrolaviciusS,etal.,FifthOrganizationto AssessStrategies in AcuteIschemic Syndromes Investigators. Comparisonoffondaparinuxandenoxaparininacutecoronary syndromes.NEnglJMed.2006;254:1464---76.
37.CorreiaLC,FerreiraF,KalilF,etal.ComparisonofACUITYand CRUSADEscoresinpredictingmajorbleedingduringacute coro-narysyndrome.ArqBrasCardiol.2015;105:20---7.
38.BoersmaE,AkkerhuisKM,TherouxP,etal.Plateletglycoprotein IIb/IIIareceptorinhibitioninnon-ST-elevationacutecoronary syndromes:earlybenefitduringmedicaltreatmentonly,with additionalprotectionduringpercutaneouscoronary interven-tion.Circulation.1999;100:2045---8.
39.StoneGW,WitzenbichlerB,GuagliumiG,etal.Bivalirudin dur-ingprimaryPCIinacutemyocardialinfarction.NEnglJMed. 2008;358:2218---30.
40.Ibanez B, James S, Agewall S, et al. 2017 ESC Guide-lines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017,
http://dx.doi.org/10.1093/eurheartj/ehx393.
41.Bellemain-Appaix A, Kerneis M, O’Connor SA, et al. Reap-praisalofthienopyridinepretreatmentinpatientswithnon-ST elevationacutecoronarysyndrome:asystematic reviewand meta-analysis.BMJ.2014;349,g6269.
42.Montalescot G, Bolognese L, Dudek D, et al. Pretreatment withprasugrelinnon-ST-segmentelevationacutecoronary syn-dromes.NEnglJMed.2013;369:999---1010.