Botulinum Toxin A in the Treatment of Spinal Cord Injury Patients
with Refractory Neurogenic Detrusor Overactivity
Ronaldo A. Alvares, Jose A. F. Silva, Andre L. Barboza, Raphael T. M. Monteiro
SARAH Network of Rehabilitation Hospitals, Belo Horizonte Unit, Belo Horizonte, MG, Brazil
ABSTRACT
Purpose: To evaluate the eficacy of botulinum toxin type A injections in the detrusor muscle in patients with spinal cord
injury and urinary incontinence due to detrusor overactivity and refractory to anticholinergic agents.
Materials and Methods: We prospectively evaluated 22 patients with spinal cord injuries, whose bladders were emptied
by intermittent catheterization. All patients had detrusor overactivity and urinary incontinence that proved dificult to treat, despite using high doses of two different anticholinergics. The pre-treatment assessment included a complete urodynamic study and ultrasonography of the kidneys and urinary tract. A one-month follow-up was completed with urodynamic evalu-ation and the clinical response was evaluated through outpatient consultevalu-ations and telephone contact.
Results: After the procedure, the maximum cystometric capacity and the bladder relex volume increased, whereas the
maximum detrusor pressure and compliance decreased. The mean duration of continence was 7 ± 7 months. In 18 patients (81.8%), it was necessary to administer anticholinergics to achieve continence. Five patients (22.7%) had indication of reinjection, and augmentation cystoplasty was indicated in 9 patients (40.9%).
Conclusion: The use of botulinum toxin in the treatment of neurogenic detrusor overactivity refractory to anticholinergics
is an option before more invasive treatments, such as augmentation cystoplasty, are attempted. In our study as well as in the literature, there was improvement in most urodynamic parameters. Overall, 40.9% of patients underwent augmentation cystoplasty and 81.8% of patients needed anticholinergic agents to reach urinary continence. Further studies are necessary to improve the procedure and to achieve better clinical results.
Key words: neurogenic bladder; spinal cord injury; botulinum toxin A, anticholinergic refractory
Int Braz J Urol. 2010; 36: 732-7
INTRODUCTION
Suprasacral spinal cord lesions induce neu-rogenic detrusor overactivity and concurrent detru-sor sphincter dyssynergia that impairs the storage and emptying functions of the urinary bladder. The subsequent high intravesical pressure leads to re-duced bladder capacity and incontinence and induces potential structural damage to the bladder wall and upper urinary tract. Current treatment options rely
Botulinum toxin was described by Van Ermengem (3) in 1897, and it has evolved from a potent biologic poison to a versatile clinical tool with an expanding list of uses. Botulinum toxin exists as seven serotypes, designated A, B, C, D, E, F, and G (4). At present, serotypes A and B are available for clinical use. Injected into muscle, botulinum toxin causes laccid paralysis by inhibiting the release of acetylcholine at the presynaptic cholinergic junction. The clinical effect of botulinum toxin is transient and dose related. In smooth muscles, Smith et al. (5) have demonstrated the effect of botulinum toxin type A on acetylcholine and norepinephrine release from the bladder and urethra, respectively.
The botulinum toxin type A injection into the detrusor muscle for treatment of neurogenic detrusor overactivity was introduced in 2000. This therapy is a minimally invasive treatment option positioned between oral anticholinergic treatment that was inef-fective or not tolerated and invasive surgery (6). Its safety and eficacy have been conirmed in a random-ized placebo-controlled study (7). Several studies have evaluated the use of botulinum toxin type A injections into the detrusor muscle of spinal cord injury patients in an attempt to reduce neurogenic detrusor overactivity, increase bladder capacity, and reduce urge incontinence (6,8). In our practice, we have observed differing clini-cal responses following the use of this drug, despite the improvements in most urodynamic parameters.
We evaluated the effect of botulinum-A toxin injection in the detrusor overactivity in spinal cord injury patients, clinical response correlation and im-plications for other treatments.
MATERIALS AND METHODS
A total of 22 patients with spinal cord injuries (16 traumatic patients and 6 non-traumatic patients), whose bladders were emptied by intermittent cath-eterization, had detrusor overactivity and urinary incontinence that proved dificult to treat, despite using high doses of two different anticholinergics. These patients were included in our prospective study between January 2006 and January 2009.
All methods and deinitions were based on the standardization of terminology of lower urinary
tract function (9). The study was done in accor-dance with the Ethics Committee of our institution. Written informed consent was obtained from all patients.
Patient evaluations included a complete medi-cal history, physimedi-cal examination, ultrasonography of the kidneys and urinary tract and an urodynamics assessment (Multichannel urodynamics studies - Medtronic Duet systems, version 8.20, Minneapolis, MN, USA) before botulinum-A toxin injection. Maxi-mum cystometric bladder capacity corresponded to the volume at which involuntary voiding occurred, urinary loss started or illing was stopped. The urody-namic parameters measured included relex volume, maximum detrusor pressure during voiding, blad-der compliance, and maximum cystometric bladblad-der capacity. Relex volume is the infused volume that induces the irst detrusor contraction. Bladder compli-ance is calculated by the change in volume divided by the change in detrusor pressure.
All procedures were done on an outpatient basis using general anesthesia. Perioperative antibiot-ics were administered orally for seven days, according to urine culture, and the botulinum toxin A injection performed on the ifth day of drug administration. All patients exhibited bacteriuria. Botulinum-A toxin (Alergan) was diluted in sterile normal saline to a inal concentration of 10 units/mL. Using a Storz cystoscope 19 F and 23 gauge needle, a total of 300 IU (30 mL) was injected at 30 detrusor muscle sites sparing the trigone as described by Schurch et al. (6). Patients were instructed to progressively taper and then discontinue their anticholinergic medications within the irst 3 weeks following the procedures. The response was considered effective when a patient sustained 4 months without urinary losses even while using anticholinergic agents.
RESULTS
A total of 22 patients, 19 males and 3 females aged to 13 to 61 years (33.6 ± 13.6) with refractory neurogenic incontinence participated in our study. All patients had urinary incontinence that was refrac-tory to anticholinergic treatment (high doses of two anticholinergic drugs). According to impairment 16 were paraplegic, six tetraplegic.
All procedures were performed with general anesthesia and were well tolerated. There were no acute complications related to the injections, such as gross hematuria, injury to adjacent structures, autonomic dysrelexia, or urinary tract infection. No complications possibly related to toxin, such as dysphagia, diplopia, or general paralysis of remote musculature occurred.
The ultrasonography of the urinary tract showed 15 patients with normal results (68.2%), 5 who had hydronephrosis (22.7%), 1 with nephropa-thy (4.5%) and 1 with a parapielic cyst (4.5%). Of the 15 patients with normal exams, 9 obtained good responses, and the 5 subjects with hydronephrosis presented only 1 patient with a good response. The patient with nephropathy did not respond and the pa-tient with a parapielic cyst showed a good response. Thirteen patients (59%) were completely continent, including two patients whose clinical responses lasted only two months and were con-sidered not effective. At the four-week follow-up, four patients with good responses had discontinued anticholinergic medications. Among the continent pa-tients, seven needed anticholinergic agents to maintain continence. However, the amount of anticholinergic medication that they needed to become continent
was less than their pre-botulinum treatment dosages. Eleven patients were incontinent despite baseline anticholinergic agent therapy and were considered failures. Nine patients (40.9%) underwent augmenta-tion cystoplasty.
At the 4-week follow-up, urodynamic evalu-ation revealed increases in mean relex volumes from 175 ± 79 mL to 312 ± 227 mL (P = 0.010) and mean maximum cystometric bladder capacity from 219 ± 113 mL to 404 ± 216 mL (p = 0.001). The compliance decreased from 30.6 ± 23.8 mL/cm H2O to 22.2 ± 11.9 mL/cm H2O (p = 0.067). Detrusor overactiv-ity decreased from 78 ± 27 cm H2O to 49 ± 30 cm H2O (Table-1). Nine patients remained incontinent at one month following treatment, despite the fact that urinary losses had decreased, and these patients expe-rienced improvements in all urodynamic parameters. Nine patients remained continent for more than six months. Therefore, we believe that the treatment was not effective in 11 patients (nine with incontinence and two with only short-lived responses).
COMMENTS
Botox injections into the detrusor provide clinically signiicant improvement in patients with neurogenic detrusor overactivity refractory to anti-muscarinics and are very well tolerated (7). In our study, we observed continence during a period of more than 4 months in 50% of patients undergoing treat-ment, while 81.8% of patients continued anticholin-ergic therapies to achieve continence. In other studies with similar populations of patients, the percentage of continents after toxin injection ranged from 42-87%
Table 1 –Urodynamic parameters before and after botulinum toxin A injection.
Urodynamic Parameters Before After p Value *
Maximum cystometric bladder capacity (mL) Mean (SD) 219 (113) 404 (216) 0.001 Detrusor overactivity (cm / H2O) Mean (SD) 78 (27) 49 (30) 0.001
Relex volume (mL) Mean (SD) 175 (79) 312 (227) 0.010
Compliance Mean (SD) 31 (24) 22 (12) 0.067
and 28-58% discontinued use of anticholinergics (10).
In our study, we observed decreased of bladder compliance in urodynamic parameters after botulinum toxin injection, in contrast to other reports in the literature (10). In our opinion, this could occur because some cases have low rates of compliance as-sociated with overactivity not previously identiied. This may bias results, as treating the neurogenic detru-sor overactivity can not only lead to gains in bladder capacity function but also to a loss of compliance that may be more evident in the urodynamic study.
There are some reported limitations with respect to botulinum A toxin injections into the detrusor. Most studies, as well as our own, were small-scale studies enrolling fewer than 50 patients. The doses of anticholinergics considered high in patients who are refractory to medical treatment are not well deined. We believe that some cases could also beneit from higher doses of these drugs. In our study, we included only cases that used at least two anticholinergic agents in high doses with no satisfactory outcomes. Those cases may have a more dificult clinical solution.
Although there is no consensus regarding the optimal dose of botulinum toxin or a standard injec-tion procedure in the detrusor muscle, most studies have used the technique described by Schurch et al. at a dose of 300 IU (6,11). Some studies such as Kuo et al. have showed similar responses at doses of 200 IU. However, this study was conducted in pa-tients with neurogenic detrusor overactivity and id-iopathic detrusor overactivity (12). Recently Gomes et al. suggested that different pharmaceutical for-mulations of botulinum toxin A might inluence the inal results. Although further evaluation will be re-quired to assess these formulations (13). Regarding the injection technique, it is important to consider that the neurogenic bladder wall has varying levels of thickness. This may lead to inadvertent injection of the medication outside the bladder wall, even in procedures performed by the same surgeon using standard endoscopy materials. Additionally, the in-jection can often occur in a subendothelial region. The Kuo study showed that there was no difference in response in this instance, but the patient cohort was of limited size (14). In our study, as well as
oth-ers, we recommended botulinum toxin injection in accordance with the clinical response to treatment (incontinence despite anticholinergic in high doses) and urodynamic results. Our results were not as sat-isfactory as other studies, probably because of the fact that many of these patients presented bladders with major structured deformities such as a large number of diverticula, low capacity and signiicant changes in their shape. These bladder morphology variations have been observed during the procedure as well as in cystography. Currently, we are study-ing the role of bladder morphology in the light of the results of botulinum toxin A injection into detru-sor.
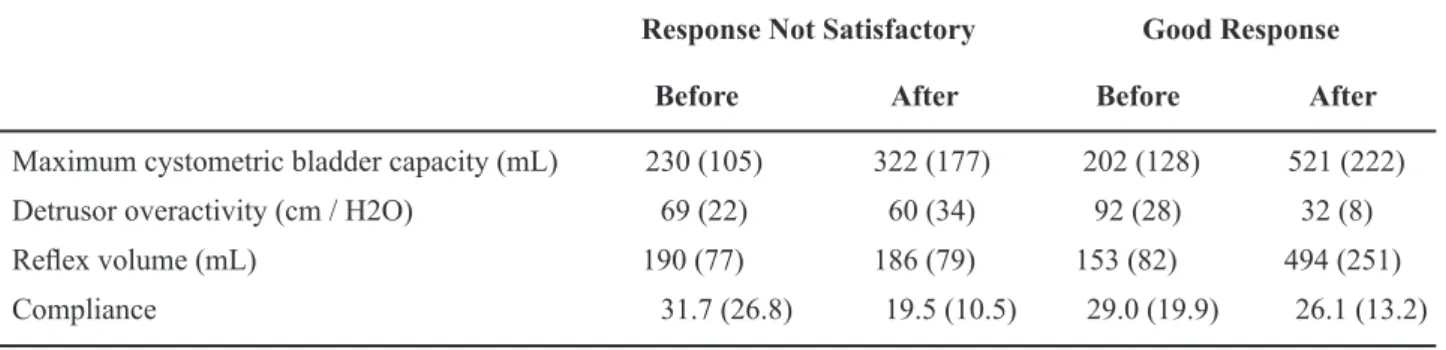
Despite the small number of patients in our study, those with hydronephrosis experienced less satisfactory responses, a inding that may help in identiication of patients to be treated. We have also compared the urodynamic parameters before and af-ter botulinum toxin A injection separately in patients who had good response and those in which the re-sponse was not satisfactory (Table-2). We observed that urodynamic parameters were similar before the procedure, although the response was different in the two groups. This allows us to conclude that urody-namic evaluation does not predict how will be the response to the procedure.
Also, note that most patients require anticholinergics to achieve and maintain continence. We believe that the effect of this therapy should last a least 4 months and that the procedure should be performed up to 3 times a year. We believe that a greater number of pro-cedures per year would be impracticable, especially for patients who require treatment for an indeinite period, but we also agree that it is not a factor that contraindicates a new injection of medication.
CONCLUSION
The use of botulinum toxin in the treatment of neurogenic detrusor overactivity refractory to anti-cholinergics is an option to consider before more inva-sive treatments, such as augmentation cystoplasty, are implemented. In our study as well as in the literature, there was improvement in most urodynamic param-eters analyzed following botulinum toxin injection. Overall, 40.9% of patients underwent augmentation cystoplasty and 81.8% of patients continued to take anticholinergic agents to reach urinary continence. Further studies are necessary to improve the proce-dure and to achieve better clinical results.
CONFLICT OF INTEREST
None declared.
REFERENCES
1. Abrams P, Larsson G, Chapple C, Wein AJ: Factors involved in the success of antimuscarinic treatment. BJU Int. 1999; 83 (Suppl 2):42-7.
2. Chartier-Kastler EJ, Mongiat-Artus P, Bitker MO, Chancellor MB, Richard F, Denys P: Long-term re-sults of augmentation cystoplasty in spinal cord injury patients. Spinal Cord. 2000; 38: 490-4.
3. van Ermengem E: Classics in infectious diseases. A new anaerobic bacillus and its relation to botulism. E. van Ermengem. Originally published as “Ueber einen neuen anaëroben Bacillus und seine Beziehungen zum Botulismus” in Zeitschrift für Hygiene und Infektion-skrankheiten 26: 1-56, 1897. Rev Infect Dis. 1979; 1: 701-19.
4. Comella CL, Pullman SL: Botulinum toxins in neuro-logical disease. Muscle Nerve. 2004; 29: 628-44. 5. Smith CP, Franks ME, McNeil BK, Ghosh R, de Groat
WC, Chancellor MB, et al.: Effect of botulinum toxin A on the autonomic nervous system of the rat lower urinary tract. J Urol. 2003; 169: 1896-900.
6. Schurch B, Stöhrer M, Kramer G, Schmid DM, Gaul G, Hauri D: Botulinum-A toxin for treating detrusor hyperrelexia in spinal cord injured patients: a new al-ternative to anticholinergic drugs? Preliminary results. J Urol. 2000; 164: 692-7.
7. Schurch B, de Sèze M, Denys P, Chartier-Kastler E, Haab F, Everaert K, et al.: Botulinum toxin type a is a safe and effective treatment for neurogenic urinary incontinence: results of a single treatment, randomized, placebo controlled 6-month study. J Urol. 2005; 174: 196-200.
Table 2 – Urodynamic parameters (mean ± standard deviation) in patients with response not satisfactory and with good response before and after botulinum toxin A injection.
Response Not Satisfactory Good Response
Before After Before After
8. Schurch B, Denys P, Kozma CM, Reese PR, Slaton T, Barron RL: Botulinum toxin A improves the quality of life of patients with neurogenic urinary incontinence. Eur Urol. 2007; 52: 850-8.
9. Abrams P, Cardozo L, Fall M, Grifiths D, Rosier P, Ulmsten U, et al.: The standardisation of terminol-ogy in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003; 61: 37-49. 10. Karsenty G, Denys P, Amarenco G, De Seze M, Gamé
X, Haab F, et al.: Botulinum toxin A (Botox) intradetru-sor injections in adults with neurogenic detruintradetru-sor over-activity/neurogenic overactive bladder: a systematic literature review. Eur Urol. 2008; 53: 275-87. 11. Rapp DE, Lucioni A, Bales GT: Botulinum toxin
injec-tion: a review of injection principles and protocols. Int Braz J Urol. 2007; 33: 132-41.
12. Kuo HC: Urodynamic evidence of effectiveness of botulinum A toxin injection in treatment of detrusor overactivity refractory to anticholinergic agents. Urol-ogy. 2004; 63: 868-72.
13. Gomes CM, de Castro Filho JE, Rejowski RF, Trigo-Rocha FE, Bruschini H, de Barros Filho TE, et al.: Experience with different botulinum toxins for the treatment of refractory neurogenic detrusor overactiv-ity. Int Braz J Urol. 2010; 36: 66-74.
14. Kuo HC: Will suburothelial injection of small dose of botulinum A toxin have similar therapeutic effects and less adverse events for refractory detrusor overactiv-ity? Urology. 2006; 68: 993-7; discussion 997-8.
Accepted after revision: June 23, 2010
Correspondence address: Dr. Ronaldo Alvarenga Álvares
Rede Sarah de Hospitais de Reabilitação Av. Amazonas 5953, Gameleira