UNIVERSITY OF TRÁS-OS-MONTES AND ALTO DOURO
STRENGTH TRAINING AND DETRAINING IN OLDER WOMEN
ACE I/D and ACTN3 R/X polymorphisms and muscle
function
ACADEMIC DISSERTATION OF PHILOSOPHY DOCTOR IN SPORT SCIENCES
Ana de Fátima da Costa Pereira
SUPERVISORS:
MÁRIO ANTÓNIO CARDOSO MARQUES
ANTÓNIO JOSÉ ROCHA MARTINS DA SILVA
ESTELA MARIA BASTOS MARTINS DE ALMEIDA
Ana de Fátima da Costa Pereira
STRENGTH TRAINING AND DETRAINING IN OLDER WOMEN
ACE I/D and ACTN3 R/X polymorphisms and muscle
function
UNIVERSITY OF TRÁS-OS-MONTES AND ALTO DOURO
P
ereira, A. (2013). Strength training and detraining in older women. ACE I/D and ACTN3 R/X polymorphisms and muscle function. University of Trás-os-Montes, Research Centre in Sport, Health and Human Development.KEYWORDS: WOMEN, AGING, ADAPTATION, RESISTANCE TRAINING, POWER OUTPUT, FUNCTIONAL CAPACITY, DETRAINING, ANGIOTENSIN CONVERTING-ENZYME GENOTYPE, ALPHA-ACTININ-3
This
academic
dissertation
was
submitted with the purpose of obtaining
a doctoral degree in Sport Sciences
according
to
the
provisions
of
Portuguese Decree-Law 107/2008 of
June 25th.
Funding
The present thesis was supported by Portuguese Science and Technology
Foundation (FCT) grant SFRH/BD/47114/2008 under the Human Potential
Operating Program, supported by the European Social Found (ESF).
“Imagination is more important than knowledge. For knowledge is limited to all we
now know and understand, while imagination embraces the entire world, and all
there ever will be to know and understand.”
Albert Einstein
Acknowledgements
The elaboration of the doctoral thesis is an arduous task for anyone who wants to achieve academic excellence. This work was only possible to be developed with an important the help of so many people around me. I would like to express my gratitude for all those who have contributed to the construction and direction of this route and who continually help me in outline new ways. I would never have been able to finish this study without the guidance of my thesis advisors, help from my friends, and support from my family.
A special thanks To Mário António Cardoso Marques PhD, my mentor, for sharing his scientific knowledge and for being an example to follow in research, and Estela Bastos PhD, for their excellent patience, teaching, and constant encouragement and counseling.
A singular thanks to António José Silva PhD, my adviser and who led me in this journey. Thanks for setting the necessary institutional contacts. Thank you for the opportunity and the confidence in my work.
To Aldo Costa PhD and Mikel Izquierdo PhD, for their useful collaboration in reviewing and correcting some papers before its submission, who this research would not have been possible without their cooperation.
To Miguel Monteiro PhD and all students, for their contribution during the data collection.
To my friends, students of UTAD and all staff of Department of Sport Sciences, for their constant interest in the status of this thesis.
To all the older women who participate in this research for their cooperation and interest. This work wouldn’t be possible without their dedication.
To my family for their unconditionally support. A distinctive thanks to my mother for the comprehension, love and for having insured me in each stone that I stumbled. To my father by the calm that was always present. And finally my key, sorry for all the moments that I was omnipresent. Together, they were always there cheering me up and stood by me through the good and bad times.
Table of Contents
Acknowledgements ... xvii
Table of Contents ... xxi
List of Publications ... xxv
Figures Index ... xxvii
Tables Index ... xxix
List of Abbreviations ... xxxi
Abstract ... xxxiii
Resumo ... xxxv
Chapter 1 – General Introduction ... 1
Chapter 2 – Review of Literature ... 7
Review. Muscle tissue changes with aging ... 7
Chapter 3 – Experimental Studies ... 17
Study 1. Effects of high-speed power training on functional capacity and muscle performance
in older women ... 17
Study 2. Muscle performance and functional capacity retention in older women after
high-speed power training cessation ... 31
Study 3. ACE I/D and ACTN3 R/X polymorphisms as potential factors in modulating
exercise-related phenotypes in older women in response to a muscle power training stimuli ... 43
Study 4. The influence of ACE I/D and ACTN3 R577X polymorphisms on lower-extremity
function in older women in response to high-speed power training ... 59
Chapter 4 – General Discussion ... 71
Chapter 5 – Overall Conclusions ... 79
Chapter 6 – Suggestions for future Research ... 83
Chapter 7 – References ... 87
List of Publications
The following parts of the present thesis are published: Review
Pereira, A., Silva A.J., Costa A.M., Almeida E.B., Marques M.C. (2012). Muscle tissue changes with aging. Acta Médica Portuguesa (Accepted).
Study 1
Pereira, A., Izquierdo, M., Silva, A.J., Costa, A.M., Bastos, E., Gonzalez-Badillo, J.J., Marques, M.C. (2012). Effects of high-speed power training on functional capacity and muscle performance in older women. Experimental Gerontology, 47, 250-255.
Study 2
Pereira, A., Izquierdo, M., Silva, A.J., Costa, A.M., Gonzalez-Badillo, J.J., Marques, M.C., (2012). Muscle performance and functional capacity retention in older women after high-speed power training cessation. Experimental Gerontology, 47, 620-624.
Study 3
Pereira, A., Costa, A.M., Izquierdo, M., Silva, A.J., Bastos, E., Marques, M.C., (2012). ACE I/D and ACTN3 R/X polymorphisms as potential factors in modulating exercise-related phenotypes in older women in response to a muscle power training stimuli. AGE, DOI 10.1007/s11357-012-9461-3.
The following part of the present thesis have been submitted for publication: Study 4
Pereira, A., Costa, A.M., Leitão J.C., Monteiro A.M., Izquierdo, M., Silva, A.J., Bastos, E., Marques, M.C. ACE I/D and ACTN3 R577X polymorphisms influence on lower-extremity function in response to high-speed power training in elderly women. Plosone.
Figures Index
Chapter 3 - Experimental Studies Study 1
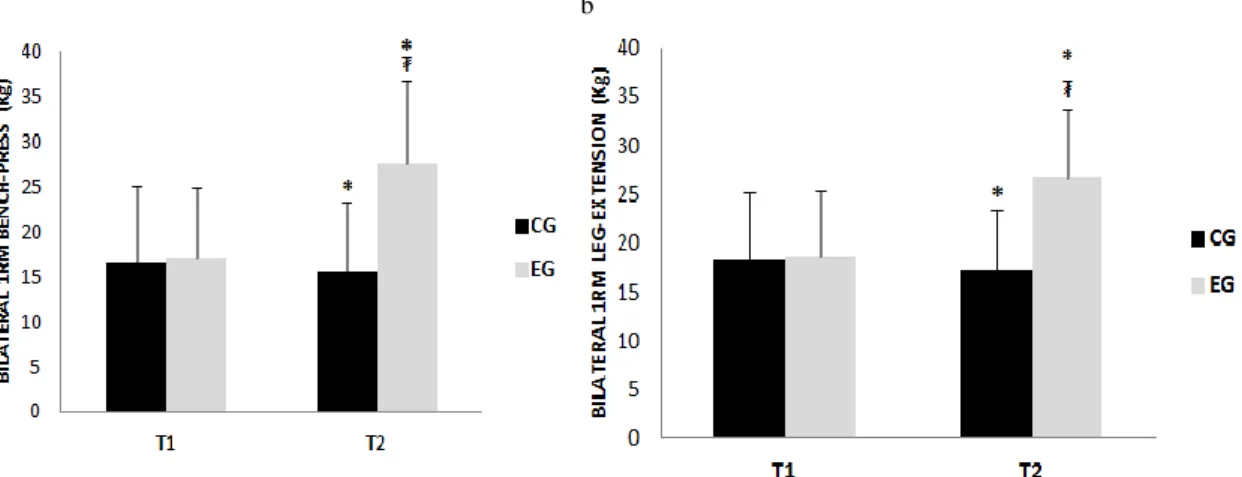
Figure 1. Maximal bilateral concentric one-repetition maximum (1RM) bench-press (a) and leg extension (b) at pre-training (T1) and after 12 weeks of training (T2)
26
Figure 2. Maximum isometric dominant hand (a) and non-dominant (b) at pre-training (T1) and after 12 weeks of pre-training (T2)
26
Figure 3. Vertical jump (CMJ) at pre-training (T1) and after 12 weeks of training (T2)
27
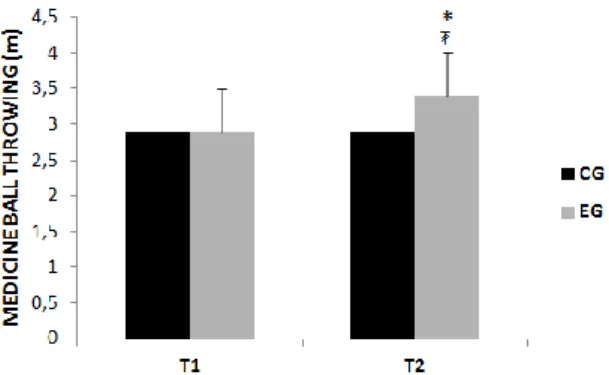
Figure 4. Medicine ball throwing at pre-training (T1) and after 12 weeks of training (T2)
27
Figure 5. Walking velocity test at pre-training (T1) and after 12 weeks of training (T2)
27
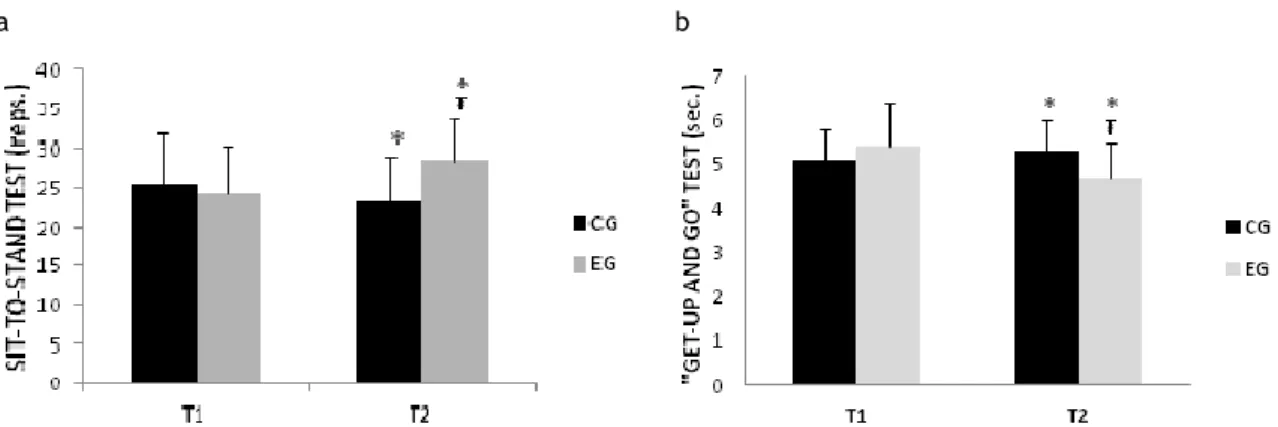
Figure 6. Sit-to-stand (a) and “get-up and go” test (b) at pre-training (T1) and after 12 weeks of training (T2)
28
Study 2
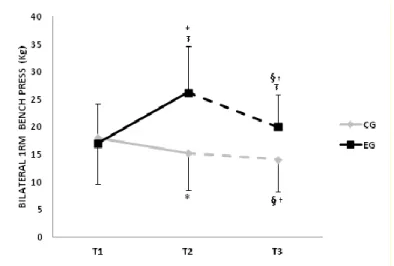
Figure 1. Bilateral 1RM bench press performance at the beginning of the protocol (T1), after 12-weeks (T2) and after stopping strength training (T3)
37
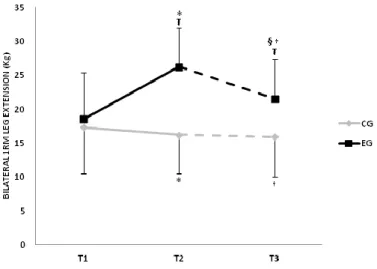
Figure 2. Bilateral 1RM leg extension performance at the beginning of the protocol (T1), after 12-weeks (T2) and after stopping strength training (T3)
38
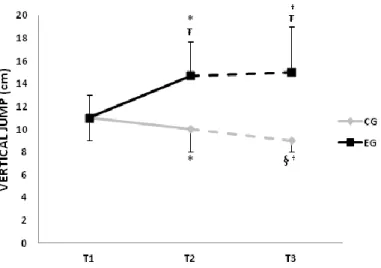
Figure 3. Vertical jump (CMJ) performance at the beginning of the protocol (T1), after 12-weeks (T2) and after stopping strength training (T3)
39
Figure 4. Ball throwing performance at the beginning of the protocol (T1), after 12-weeks (T2) and after stopping strength training (T3)
39
Figure 5. Sit-to-stand test performance at the beginning of the protocol (T1), after 12-weeks (T2) and after stopping strength training (T3)
General Introduction
Strength training, detraining and muscular genotypes in older women
xxviii
Study 3
Figure 1. Bilateral 1RM bench press performance at the beginning of the protocol (T1) and after 12 weeks (T2)
53
Figure 2. Bilateral 1RM leg extension performance at the beginning of the protocol (T1) and after 12 weeks (T2)
53
Figure 3. Vertical jump (CMJ) performance at the beginning of the protocol (T1) and after 12 weeks (T2).
53
Figure 4. Sit-to-stand test performance at the beginning of the protocol (T1) and after 12 weeks (T2).
54
Study 4
Figure 1. Walking velocity test at the beginning of the protocol (T1) and after 12-weeks (T2).
67
Figure 2. “get-up and go” test at the beginning of the protocol (T1) and after 12-weeks (T2).
Tables Index
Chapter 2 – Review of Literature Review
Table 1. Studies of high-velocity resistance training interventions on physical functioning in older people
15
Chapter 3 – Experimental Studies Study 1
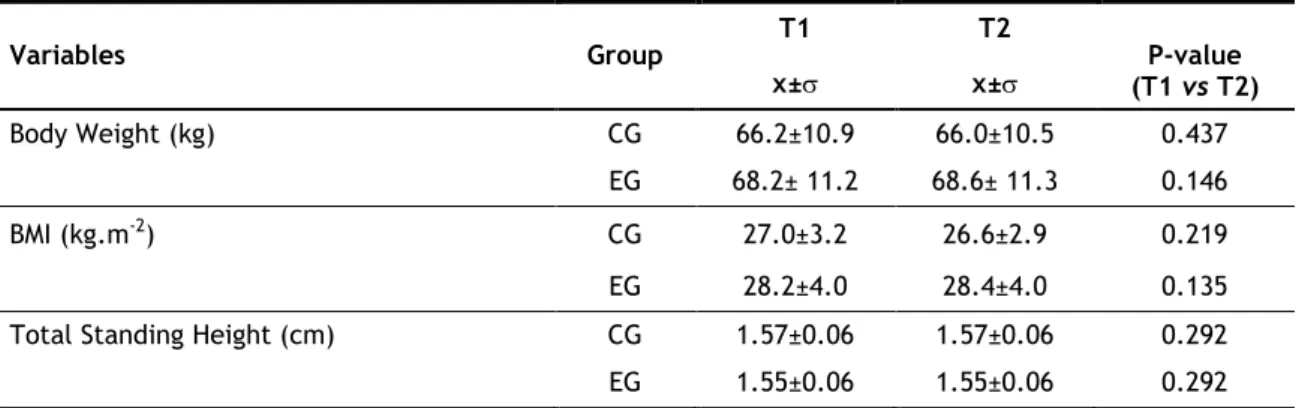
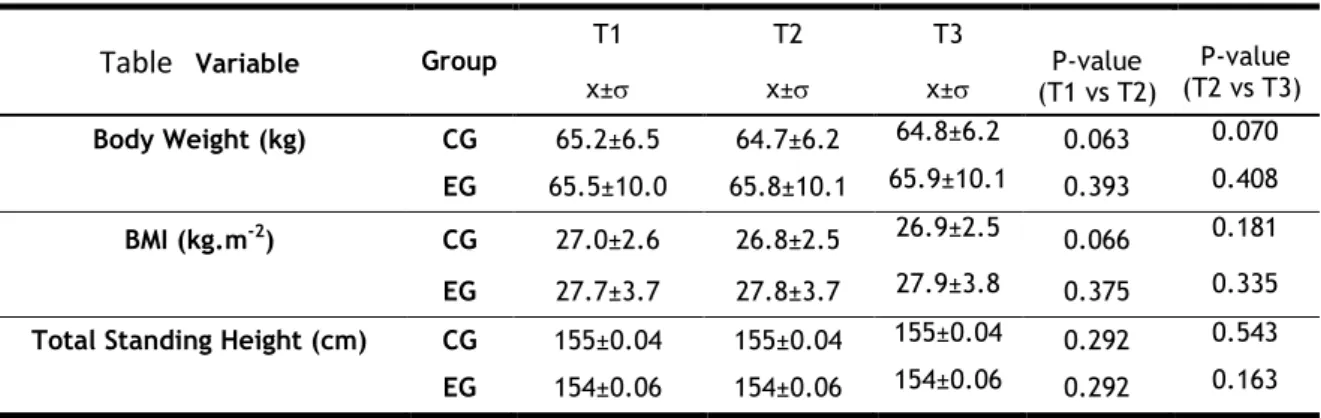
Table 1. High-speed power training between week 1 and week 12 24 Table 2. Mean±standard deviation values regarding the subject's anthropometric
characteristics
25
Study 2
Table 1. Changes in the anthropometric characteristics of the subject’s during baseline, training and detraining
36
Study 3
Table 1. Mean ± standard deviation values regarding the subject’s anthropometric characteristics
50
Table 2. Effect of ACE genotype in older Caucasian women in test performance gains during training
51
Table 3. Effect of ACTN3 genotype in older Caucasian women in test performance gains during training.
52
Study 4
Table 1. Effect of ACE genotype in older Caucasian women in test performance gains during training.
66
Table 2. Effect of ACTN3 genotype in older Caucasian women in test performance gains during training.
List of Abbreviations
1RM one repetition maximal strength 1RMBP one repetition maximum in bench press 1RMLE one repetition maximum in leg extension ACE angiotensin-converting enzyme
ACTN3 alpha-actinin 3
AT-1 receptor At1 of angiotensina2 BMI body mass index
BT ball throwing CG control group
CMJ counter-movement jump DNA deoxyribonucleic acid DT detraining
EG experimental group GUG “get-up and go” test
HGd maximum isometric strength dominant hand HGnd maximum isometric strength non-dominant hand mRNA messenger ribonucleic acid
N number of subjects
PCR-RFLP polymerase chain reaction, restriction fragment length polymorphism RAS rennin–angiotensin system
Reps repetitions RT resistant training
S10 maximum sprints of 10 m Sets series
SD standard deviation
SPPB short physical performance battery STS sit-to-stand test
T1 pre-training T2 post-training
General Introduction
Strength training, detraining and muscular genotypes in older women
xxxii
T3 period of detraining
TNF-α tumoral necrosis factor-alpha TNF-b tumoral necrosis factor-beta Vo2max maximal oxygen consumption X2 chi-square
Abstract
Age-realted declines are more pronounced in muscle power characteristics, a cornerstone of functional limitations and quality of life in older people. Studies have also shown substantial variation among subjects in response of resistant training, indicating the potential role of genetic component to training-induced muscle adaptation. The purpose of this investigation was twofold 1) examine the effect of 12 weeks high-speed power training on isometric contraction (handgrip strength), maximal strength (1RM) of the arm and leg muscles, power performance (walking velocity, counter movement jump and ball throwing) and functional tasks (sit-to-stand and get-up and go tests) in older women and 2) analyze the impact of 6 weeks of detraining on maximal strength (1RM), power performance and functional task (sit-to-stand test). Secondly, it was intended to identify the magnitude of the differences between the subjects according to the genetic variation of the human ACE I/D and ACTN3 R577X polymorphisms (single or combined) before and subsequent to 12 weeks of high-speed power training. For the accomplishment of these purposes the following sequence was used: (i) reviewing available literature; (ii) analyzing the effects of high-speed power training on functional capacity and muscle performance in older women; (iii) examine muscle performance and functional capacity retention after training cessation; (iv) analyzing the association between ACE I/D and ACTN3 R/X polymorphisms (single or combined) in response to training stimuli, (v) and analyze the influence of muscular genotypes on lower-extremity function after the program training. Results suggest that: (i) high-speed power training is an effective exercise approach leading to large gains in upper and lower extremity muscle performance and function capacity in older women; (ii) detraining may induce larger declines in muscle strength than in power output and preserved physical independence, mediated in part, by the effectiveness of high-speed power training; (iii) ACE and ACTN3 genotypes (single or combined) exert a significant influence specially in muscular power phenotypes of older women in response to high-speed power training; (iv) and ACE I/D and ACTN3 R577X polymorphisms are likely candidates in the modulation of exercise-related power phenotypes in older women but not a significant influence in mobility traits.
Keywords
Women, Aging, Adaptation, Resistance training, Power output, Functional capacity, Detraining, Angiotensin Converting-enzyme genotype, Alpha-Actinin-3
Resumo
Os declínios relacionados com o avanço da idade ocorrem de forma mais pronunciada nas características de potência muscular, fator inerente nas limitações funcionais e na qualidade de vida na população idosa. Estudos têm demonstrado uma variação substancial entre indivíduos em resposta ao treino de força, indicando o potencial papel da componente genética na adaptação muscular induzida pelo treino. O propósito desta investigação foi 1) examinar o efeito de 12 semanas de treino de potência com velocidade elevada na contração isométrica (força de preensão manual), força máxima (1RM) dos grupos musculares dos membros superiores e inferiores, potência muscular (velocidade de caminhar, salto com contramovimento e lançamento da bola medicinal) e testes funcionais (levantar e sentar da cadeirae levantar ir e voltar testes) em mulheres idosas; 2) analisar o impacto de 6 semanas de destreino na força máxima (1RM), potência e capacidade funcional (levantar e sentar da cadeira em 30s). Além disso, foi ainda objetivo identificar a magnitude das diferenças entre os sujeitos de acordo com a variação genética dos polimorfismos dos genes ECA (I/D) e ACTN3 (R577X) de forma singular ou combinada, antes e após 12 semanas de treino de potência com velocidade elevada. Para a realização dos nossos objetivos, a seguinte sequência foi utilizada: (i) revisão da literatura existente; (ii) analisar os efeitos do treino de potência com velocidade elevada na capacidade funcional e na performance muscular em mulheres idosas; (iii) examinar a retenção da performance muscular e da capacidade funcional após a cessação de treino; (iv) analisar a associação entre os polimorfismos dos genes ECA (I/D) e ACTN3 (R577X) de forma singular ou combinada, em resposta ao treino, (v) e analisar a influência dos genótipos musculares na funcionalidade da extremidade inferior após o programa de treino. Resultados sugerem: (i) o treino de potência com velocidade elevada é efetivo na melhoria da performance muscular e da capacidade funcional em mulheres idosas; (ii) o destreino parece induzir amplos declínios na força muscular em relação à produção de potência, preservando desta forma a independência física, mediada em parte, pela efetividade do treino com velocidades elevadas; (iii) os genótipos ECA e ACTN3 exercem uma influência significante (singular ou combinada) em fenótipos musculares em mulheres idosas em resposta ao treino de potência com velocidade elevada; (iv) os polimorfismos dos genes ECA (I/D) e ACTN3 (R577X) são candidatos na variação de fenótipos relacionados com a potência muscular em mulheres idosas, no entanto não exercem uma influência significantiva em tarefas de mobilidade.
Palavras-Chave
Mulher, Envelhecimento, Adaptação, Treino de Força, Produção de Potência, Capacidade Funcional, Destreino, Genótipo da Enzima Conversora da Angiotensina, Alfa-Actinina-3
General Introduction
General Introduction
Age-related decrease of skeletal muscle mass and function (sarcopenia) contributes to reduced functional capacity for independent living especially in elderly women (Doherty, 2003). According to the disablement system, impairment refers to a loss of the tissue and body system level. Losses can progress to functional limitations and disability in older people, causing further disease atrophy and a decline in total physical performance (Aagaard et al., 2010; Carvalho et al., 2009). The underlying physiological mechanisms that contribute to this reduction among older adults include also a decrease in muscle power output, alterations in individual muscle fiber contractile properties and modifications in neuromuscular function. Recently, muscular adaptation to resistant training as shown substantial variation between subjects and it has been associated with some genetic variation (Roberts et al., 2010; Tan et al., 2012; Bustamante-Ara et al., 2010; Garatachea et al., 2011).
Genetic factors interact with aging and thus modulate the functional capacity and muscle phenotypes in older adults in response to a resistant training. However, prevention should be the main concern and with increasing age it seems essential the participation in regular resistance exercise programs focus on strength and power exercises complemented with some preventative strategies. For that reason, the increase and maintenance of muscle performance in early adulthood may reduce the risk of developing early sarcopenia status and leads to a healthy aging (Study Review).
Age-related declines more rapidly in muscle power (the product of the force and velocity of muscle contraction) as a proximal determinant of functional limitations in older adults compared with muscle strength (the ability to generate maximal muscle force) (Häkkinen et al., 1998; Izquierdo et al., 2001; Bonnefoy et al., 2007; Arnold et al., 2010). These negatively impact in quality of life specially in older women through their contribution to functional decline in perform daily activities, as clean the house and increase the inability to remain independent and living in the community (Häkkinen et al., 1998; Izquierdo et al., 2001; Bonnefoy et al., 2007; Caserotti et al., 2008; Webber and Porter, 2010). The recognition that resistance training is the most usual intervention to enhance muscular strength and power as well as physical functionality (Reid & Fielding, 2012) has produced a wide range of studies on the influence of various factors on physical fitness, in particular the effect of muscular performance and functional capacity (Kalapotharakos et al., 2005; Holviala et al., 2006; Bonnefoy et al., 2007). However, besides traditional resistant programs in older women, it seems that fast and explosive muscular actions are more useful to the characteristics of this population (Häkkinen et al., 1998; Izquierdo et al., 2001; Caserotti et al., 2008; Webber and Porter, 2010). Thereby, a lower capacity for concentric contractions may result in impaired performance, particularly in activities where rapid movements are essential as, for example, counteracting a forward fall, climbing steps or crossing the road.
General Introduction
Strength training, detraining and muscular genotypes in older women
4
Older women usually experience a large time of interruptions in regular training sessions and little is known about the regressive effects after the training cessation (Ivey et al., 2000; Lemmer et al., 2000; Henwood and Taaffe, 2008). Hence it seems relevant to examine, in this age group, the effect of a high-speed program training based on strength and power exercises in upper and lower-extremity and analyze the changes in physical parameters during detraining, often referenced in the literature for older women (Study 1 and 2). The majority of studies on resistant training focuses in muscular and power performance, but evidence about the contribution of muscle power to various functional tasks and relationships with muscle strength are mentioned (Häkkinen et al., 2000; Henwood and Taaffe, 2008; Henwood et al., 2008) in older population. Thus, develop specific resistant training programs is fundamental to understand some of the physiologic mechanisms in muscular adaptation and their relationship with functional performance. Besides, the advantage of performing high-speed power training instead of traditional training appears to be the higher preservation of muscle power output achieved (Häkkinen et al., 2000; Henwood and Taaffe, 2008). It may also be related to optimize recruitment of fast twitch fibers (Lexell, 1995). As such, it will be relevant to analyze specifically the effects of high-speed power training particularly designed for older women, focused on explosive movement performance to enhance maximal strength, muscle power and functional capacity (Study 1).
Nevertheless, as muscular performance, specially power output, declines earlier with advancing age, there exist evidences suggesting that training cessation among older women is associated with the loss of functional capacity as a consequence of poor muscular performance development during the period of resistant training (Henwood and Taaffe, 2008; Carvalho et al., 2009). However, only a few studies examine the regressive effects of a detraining period in older women (Häkkinen et al., 2000; Ivey et al., 2000; Lemmer et al., 2000; Toraman, 2005;Harris et al., 2007; Henwood and Taaffe, 2008; Carvalho et al., 2009). Indeed, power training development compared to classical strength training intervention may retain muscular gains after a detraining period in older women, if the magnitude of responses during the period of intervention where greater (Bickel et al., 2011). These could be related in part to a better recruitment and synchronization of motor units (Kannus et al., 1992). In this respect, beyond the duty of the professionals of sport science to maximize the muscular adaptations (gains in muscular strength, power and functional capacity) in older population, it is necessary to develop exercises in order to make them appealing and motivating for older women. Besides, it must always be associated with rigorous designs of resistant training programs. Therefore, the knowledge of the main changes in physical parameters produced during a high-speed power training, but also the magnitude of the differences after 6-weeks of detraining can help teachers and trainers in planning programs trainings taking into account the characteristics of older women, and thus, increase their levels of physical fitness
(Study 2).
Substantial variation among subjects in response to resistant training, have been recently attributed to potential genetic component to training-induced muscle adaptation (Ahmetov
General Introduction
and Rogozkin 2009; Bustamante-Ara et al. 2010; McCauley et al. 2010; Garatachea et al. 2011; Garatachea and Lucia, 2011). In general, muscle strength is known to be a heritable phenotype to 30-85% depending on the muscle group (Costa et al., 2012) and the characteristics of type of training and exercise (Ahmetov and Rogozkin, 2009). Recognize this interaction with aging is important for understanding the maintenance of muscular performance
(
Thomis et al., 1998) and provide specific interventions and thus ultimately to prolong an independent lifestyle. Thereby, genetic variation can answer some questions as to adaptations occur and how is the interaction with the type of training (Coffey and Hawley, 2007). However, in order to maximize the benefits of training, previous association studies have suggested a genetic contribution to individual variability but only a few studies (Ahmetov and Rogozkin, 2009; Bustamante-Ara et al. 2010; McCauley et al. 2010; Garatachea et al. 2011) examined the genotype variation in an aged population. Moreover, the genetic contribution to training-induced effects also remains to be clarified (Bouchard and Rankinen 2001; Garatachea and Lucia 2011). Thus, it seems relevant to identify training response of different genotypes associated with decreases of muscular performance (Garatachea and Lucia 2011) (Study 3 and 4).Concerning ACE I/D and ACTN3 R/X polymorphisms, some studies have examined their influence (Bustamante-Ara et al. 2010; Garatachea et al. 2011) but the role of significant cumulative genotype-training effect remains to be explained. Thus, genetic variation may influence the execution of the planned exercises, training intensity and muscular adaptation, resulting in different effects of applying a particular training program for older women. The knowledge of the genetic variation after a period of high-speed power training may partly explain the older individual variability in muscle performance adaptation to resistance training and can help in designing and applying the training programs for older people, in order to improve its efficiency (Study 3). Moreover, as limitations in mobility are an indicative of decline in functional health (Cooper et al., 2011; den Ouden et al., 2011) it will also be relevant to analyze the influence of the ACE I/D and ACTN3 polymorphisms, alone and in combination, in walking performance tests, understanding the relationship between impairments, functional limitations, and resultant disability in older women in response to high-speed power training (Study 5).
Considering the abovementioned, the aim of this thesis was to analyze the effect of high-speed power training and detraining on maximal strength, power output and functional capacity in older women. An additional objective was to identify the possible association between different genotypes (concerning ACE and ACTN3 genes) and the response to the intervention program in older women.
This research project entitled Strength training and detraining in older woman and its relationship with muscular genotypes was supported by the Portuguese Government by a grant of the Science and Technology Foundation (SFRH / BD / 47114 / 2008). In the last four years several works have been presented in International and National Scientific Meetings and others have been published in Scientific Journals.
General Introduction
Strength training, detraining and muscular genotypes in older women
6
The Thesis has the following main chapters:
Chapter 2 presents a review of the literature based on the earlier studies regarding the etiology and prevention of Sarcopenia.
Chapter 3 includes four studies: Study 1 analysis the effects of high-speed power training on muscle performance in older women; Study 2 aims to add new evidence of detraining subsequent to high-speed power training on maximal strength, power performance and functional task; Study 3 demonstrates the differences between older women and ACE I/D and ACTN3 R/X polymorphisms particularly in response to a resistance training stimuli and Study 4 exhibits the influence of ACE ID and ACTN3 R577X polymorphisms on lower-extremity function in older women in response to high-speed power training.
Chapter 4 and Chapter 5 present a general discussion of the results obtained in the five independent studies and the main conclusions of the thesis are displayed.
Chapter 2 – Review of Literature
Muscle tissue changes with aging
Abstract
Sarcopenia is characterized by a progressive generalized decrease of skeletal muscle mass, strength and function with aging. Recently, the genetic determination has been associated with muscle mass and muscle strength in elderly. These two phenotypes of risk are the most commonly recognized and studied for sarcopenia, with heritability ranging from 30 to 85% for muscle strength and 45-90% for muscle mass. It is well known that the development and maintenance of muscle mass in early adulthood reduces the risk of developing sarcopenia and leads to a healthy aging. For that reason it seems important to identify which genetic factors interact with aging and in particular with the musculoskeletal response to exercise in such individuals.
This review is designed to summarize the most important and representative studies about the possible association between certain genetic polymorphisms and muscle phenotypes in older populations. Also we will focuses on nutrition and some concerns associated with aging, including the role that exercise can have on reducing the negative effects of this phenomenon. Some results are inconsistent between studies and more replication studies underlying sarcopenia are needed, with larger samples and with different life cycles, particularly in the type and level of physical activity throughout life. In future we believe that further progress in understanding the genetic etiology and the metabolic pathways will provide valuable information on important biological mechanisms underlying the muscle physiology. This will enable better recognition of individuals at higher risk and the ability to more adequately address this debilitating condition.
Muscle tissue changes with aging
Strength training, detraining and muscular genotypes in older women
10
Introduction
Sarcopenia is characterized by a decline in muscle mass and strength with creasing age. Currently, this is a problem in elderly people because it contributes to reduce the capacity for independent living. Hospitalization and falls often results in further disease atrophy and a decline in physical performance that results in a loss of autonomy (Doherty, 2003). Complications resulting from falls constitute the sixth cause of death in older people (Visvanathan & Chapman, 2009). As a part of normal aging, muscle mass is reduced by approximately one-third between the ages of 50 and 80 years. Although it is possible to increase muscle mass and bone density after the fifth decade (Janssen, Heymsfield, Ross, 2002). However prevention should be the main concern because is difficult to regain muscle tissue after several quantities is lost. For that reason, the increase and maintenance of muscle mass in early adulthood reduces the risk of developing sarcopenia and leads to a healthy aging (Rosenberg, 1997).
It is also important to determine the genetic factors that interact with aging and thus modulate the functional capacity and muscle phenotypes in older adults (Roberts et al., 2010). It is clinically relevant, the identification of “unfavorable” genotypes associated with sarcopenia (Tan et al., 2012). Special emphasis has been placed on two polymorphisms that have been most extensively studied, i.e., the angiotensin converting enzyme gene (ACE) I/D and the alpha-actinin-3 (ACTN3) R577X (Garatachea et al., 2011). Although the published studies indicate that hereditability is an important genetic contribution to individual variability in muscle phenotypes among elderly people, but the published data on specific gene variants are controversial (Bustamante-Ara et al., 2010; Garatachea et al., 2011). Furthermore, with increasing age it seems essential the participation in regular resistance exercise programs focused on strength and power exercises, benefiting muscle anabolism, an effect that can be enhanced if the exercise is followed by a nutrition rich in proteins (Phillips, 2004).To achieve maximum benefit, preventative strategies for sarcopenia should ideally begin before the fourth decade of life and continue long-term (Bickel, Cross, Bammn, 2011). This review article describes some of these preventative strategies.
Etiology of Sarcopenia
The etiology of sarcopenia is not clearly understood, however several mechanisms have been proposed. Ageing is associated with quantity and quality of muscle tissue reductions (Rosenberg, 1997). Usually sarcopenia is defined by determining cut-off measures of skeletal muscle mass below in which there is evidence of functional decline or characterized by values two or more standard deviations below the young adult mean. Janssen et al. (2004) characterized values of cut-off measures of skeletal muscle mass by 5.76-6.75 kg/m2 and 8.51-10.75 kg/m2 for women and men, respectively. These values correspond to the risk of disabilities of muscle function during everyday activities. Social and financial costs associated
Muscle tissue changes with aging
with such disability have been increasing in the past decades, therefore strategies for preventing sarcopenia are of considerable importance. However, prevention requires an understanding of how it develops.
A group of mechanisms are involved in sarcopenia, namely the reduction in the number and size of type I and II fibers, decrease in the number of motor units, accumulation of oxidative products, reduced activation of satellite cells and also reduced excitation–contraction coupling (Lang et al., 2010). Furthermore the reduction of anabolic hormones (testosterone, estrogen, growth hormone and insulin like growth factor-1), increasing inflammatory activity and inadequate nutrition and inactivity also contribute substantially to the development of age-related sarcopenia.
Muscle Tissue
The structure of muscle changes in older people has been well-described (Snijders, Verdijk, Van, 2009). One of the effects of aging is the involuntary loss of muscle mass, strength and function (Janssen, Heymsfield, Ross, 2002). Nevertheless, aging is also characterized by a gradual loss of motor neurons, due to apoptosis, high levels of circulating cytokines (TNF-a and TNF-b) and reduced signaling growth factors. Autopsies in the vastus lateralis muscle have shown that up to 90 years, there is a reduction by 50% in type I and II fibers per decade, when compared to young individuals. Histochemical studies conclude that the reduction and atrophy occurs mainly in type II muscle fibers with age (Frontera et al., 2008). This reduces the excitation–contraction coupling, affecting muscle function with increasing age (Pereira et al., 2012). Indeed, in an attempt to minimize fiber loss, collaterals from the type I motor neurons expand to some of the denervated type II fibers (Verdijk et al., 2009). Therefore, the muscle tissue tends to lose its configuration, affecting the muscular system (disorders of myofilaments and Z-lines) and mechanisms (reduced satellite cell activation/proliferation and changes to mitochondrial function of muscle cells), which decreases muscle performance (reduction of maximum muscle strength and power). This will increase the disabilities and functional capacity for everyday tasks will also be affected reducing the quality of life and decreasing longevity.
ACE and ACTN3 genes and their association with muscle phenotypes
A wide range of human phenotypes (e.g., muscle strength and bone structure) influence muscle function and result in a complex interaction between different systems: anatomic, biochemical and physiological. About 20 000 genes defines each of us as human beings (Tan et al., 2012). However, there is substantial variation among individuals and that can be seen from “replicating” of gene sequences, or changes in base pairs (individual mutations if frequency < 1% and polymorphisms if single nucleotide > 1% frequency). Some polymorphisms
Muscle tissue changes with aging
Strength training, detraining and muscular genotypes in older women
12
can significantly affect muscle structure, the functional performance and even the response to exercise training. One potential candidate gene is the Angiotensin Converting Enzyme (ACE) gene. ACE gene is located at C17 (17q23.3) and has 25 exons resulting in an mRNA with 4022 nucleotides and a protein with 1306 amino acids (ENSG00000159640) (http://www.ncbi.nlm.nih.gov/SNP//snp_ref.cgi?locusId=1636). Multiple alternatively spliced transcript variants encoding different isoforms have been identified (Rieder et al., 1999). ACE has a key role on the endocrine rennin-angiotensin system and is responsible for catalyzing the conversion of angiotensin I into angiotensin II. Research has centered on an insertion– deletion (I/D-allele) polymorphism in intron 16, which is characterized by the presence (I-allele) or absence (D-(I-allele) of a 287 bp Alu repeat sequence with 535 SNPs. This result in three genotypes: II, DD and ID. In Caucasians, the genotype frequency is approximately 25%, 25% and 50%, respectively (Costa et al., 2009). However, there is some evidence of a different distribution in other racial groups (Barley et al., 1996).
In cross-sectional studies, the D allele has been associated with subjects with higher values of muscle mass, volume and strength (Zang et al., 2003; Giaccaglia et al., 2008), while other studies found no association (McCauley et al., 2009; Garatachea et al., 2012). The possibility that the DD genotype may be associated with a greater proportion of fast twitch fibers could explain the possible influence of the ACE D allele upon strength/ power, particularly at high velocities tasks (Giaccaglia et al., 2008). Besides, the II genotype confers some disadvantage in functional tasks and, therefore, may correspond to a lower muscle performance.
Another candidate gene, ACTN3, is located at C11 (11q13.1) and has 21 exons resulting in an mRNA with 3084 nucleotides and a protein with 944 amino acids (ENSG00000248746) (http://www.ncbi.nlm.nih.gov/SNP//snp_ref.cgi?locusId=89). This gene expression is limited to skeletal muscle and is localized to the Z-disc, where it helps to anchor the myofibrillar actin filaments (Lek, Quinlan, North, 2010). Variations in ACTN3 gene can explain individual variability in muscle phenotypes by a substitution of arginine at amino acid residue 577 (R-allele) with a premature stop codon (X-(R-allele). Judson et al. (2011) showed that functional ACTN3 R577X genotype represents a genetic risk factor in older women and reported a strong association between R577X genotype with increased risk of falling (10%-61%). Clarkson et al. (2005) and Walsh et al. (2008) also found that women with the XX genotype had lower strength in the elbow flexors and knee extensors compared with individuals with genotype RR. Thus alpha-actinin-3 577X may induces muscle weakness and some influence in responses to muscle damaging exercise. However, it is necessary to develop and reproduce more studies in the elderly people to strengthen these sentences. Future studies should consider the association between muscle phenotypes in this population and complex gene and gene-environment interactions.
Muscle tissue changes with aging
Prevention of sarcopenia
Nutrition
A variety of hormonal changes that contribute to the loss of muscle mass is observed during the aging process. The body weight and consequently the body mass index (BMI) tend to decline after ages of 50-60 years (Flegal et al., 2002). The weight guidelines for body mass index in older people is in the range of 27–30 kg/m2 and for younger individuals is between 18.5-25 kg/m2 and when is considered ideal weight for older subjects this may already be at malnutrition and sarcopenia risk (Janssen et al., 2004). Besides, the decline in food intake in older persons has been termed “anorexia of ageing” (Flegal et al., 2008). Older subjects should also reduce their nutrition and meals by quantity in food intake, especially dietary protein (Visvanathan & Chapman, 2009). However, the quantities of protein intake in recommended daily allowance may be inadequate for exercising subjects. This remains to determine, whether nutritional supplementation can augment training-induced strength gains in older people. However, the effect of the supplement is not always statistically significant for all exercises (Phillips, 2004; Visvanathan & Chapman, 2009). Comparatively to creatine supplementation may enhanced the increase in lean mass, and only enhanced strength in some exercises (Phillips, 2004; Visvanathan & Chapman, 2009). In older obese, weight loss should be achieved in a way that preserves lean tissue. This should be through the inclusion of an exercise program that includes strength and aerobic exercises, and simultaneous ingestion of protein, calcium and vitamin D. Nutritional interventions, as obtaining nutrients from natural food (soybeans, lentils, beef, peanuts, salami and salmon) are appealing potential means for the prevention and treatment of sarcopenia (Koopman & Van Loon, 2009).
Exercise Training
The best way of preventing sarcopenia appears to be by maintaining a regular exercise program (Bickel, Cross, Bamman, 2011). Strength exercise has been suggested as the preferred strategy to attenuate and reverse the age-related loss of muscle mass and function (Verdijk et al, 2009). Multiple studies have demonstrated that acute resistance exercise increases myofibrillar muscle protein synthesis in older adults (Hasten et al., 2000; Verdijk et al, 2009). Recent studies have shown that the increase in muscle mass and myonuclear content in response to strength exercise is accompanied by an increase in number and activation of satellite cells (Olsen et al., 2006). It has also been associated with improvements in aerobic capacity (VO2max), improved performance on daily tasks, such as climbing stairs, rising from a chair and even walking (Capodaglio et al., 2007).
Muscle tissue changes with aging
Strength training, detraining and muscular genotypes in older women
14
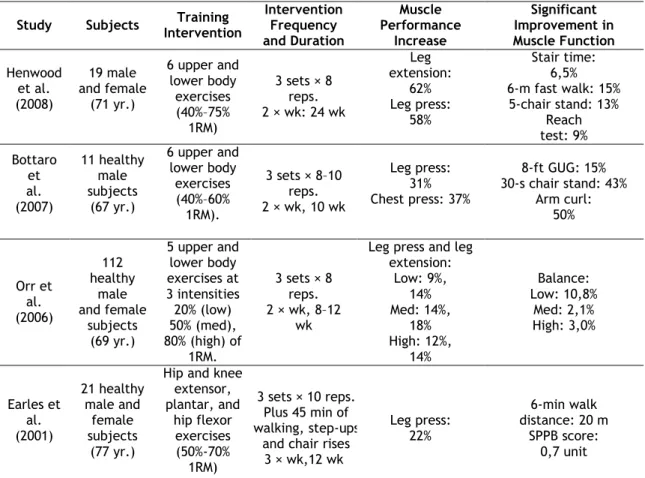
As the area of strength-training investigation progresses, some scientists are trying to identify the best exercise programs for this population, while others continue their research in determining what exercise prescription will confer the most benefits for older adults. Currently, it seems generally agreed that the benefits of strength training can be achieved with low intensities of 50% of one repetition maximum (1˂RM) and not only in greater intensities (to 80% of 1RM). Indeed, a markedly lower capacity for concentric contractions may result in decline in performance, particularly in tasks where rapid movements are essential (counteracting a forward fall, climbing steps or crossing the road) (Pereira et al., 2012). Nevertheless, early studies evaluating whether resistance training interventions could increase especially lower extremity muscle in older people (Pereira et al., 2012; Reid & Fielding, 2012). Thus, recent randomized trials in both men and women, have been designed to maximize muscle performance generally and have demonstrated that high velocity power training is well tolerated and effectively (Pereira et al., 2012) (Table 1). However, the efficacy and feasibility of high-velocity power training in older adults with chronic conditions (osteoarthritis and/or osteoporosis), remains uncertain. Aerobic exercise also helps to delay age-related decline. Although, depending on its type and intensity, aerobic exercise seems to have quite minor beneficial effects to prevent the aging effects in muscle system (Harber et al., 2009).
Muscle tissue changes with aging
Table 1. Studies of high-velocity resistance training interventions on physical functioning in older people.
Study Subjects Intervention Training Intervention Frequency and Duration Muscle Performance Increase Significant Improvement in Muscle Function Henwood et al. (2008) 19 male and female (71 yr.) 6 upper and lower body exercises (40%–75% 1RM) 3 sets × 8 reps. 2 × wk: 24 wk Leg extension: 62% Leg press: 58% Stair time: 6,5% 6-m fast walk: 15% 5-chair stand: 13% Reach test: 9% Bottaro et al. (2007) 11 healthy male subjects (67 yr.) 6 upper and lower body exercises (40%–60% 1RM). 3 sets × 8–10 reps. 2 × wk, 10 wk Leg press: 31% Chest press: 37% 8-ft GUG: 15% 30-s chair stand: 43% Arm curl: 50% Orr et al. (2006) 112 healthy male and female subjects (69 yr.) 5 upper and lower body exercises at 3 intensities 20% (low) 50% (med), 80% (high) of 1RM. 3 sets × 8 reps. 2 × wk, 8–12 wk
Leg press and leg extension: Low: 9%, 14% Med: 14%, 18% High: 12%, 14% Balance: Low: 10,8% Med: 2,1% High: 3,0% Earles et al. (2001) 21 healthy male and female subjects (77 yr.)
Hip and knee extensor, plantar, and hip flexor exercises (50%-70% 1RM) 3 sets × 10 reps. Plus 45 min of walking, step-ups
and chair rises 3 × wk,12 wk Leg press: 22% 6-min walk distance: 20 m SPPB score: 0,7 unit
Legend: reps = repetitions; 1RM = 1 repetition maximum; GUG = timed up and go; SPPB = short physical performance battery
Summary and future directions
There is a need to develop strategies to prevent sarcopenia in both men and women in order to prevent loss of muscle mass and functionality with aging. Further the progress to understanding the genetic etiology of sarcopenia will provide valuable mechanisms that will improve the ability to recognize individuals at risk. Current research has suggested that the optimal intervention program should include predominantly resistance exercises (strength training), complemented with some aerobic stimuli. As older people reduce food intake, an adequate nutrition is essential to obtain all benefits from resistance training.
The main research findings can be summarized as follows:
(i) There is a relationship between sarcopenia and the loss of autonomy;
(ii) Reduction of anabolic hormones, inadequate nutrition and inactivity are detrimental to the increase of sarcopenia;
Muscle tissue changes with aging
Strength training, detraining and muscular genotypes in older women
16
(iii) Nutrition intervention are necessary to prevention and treatment of sarcopenia specially for exercising older people;
(iv) Muscle tissue tends to lose its configuration, as reduction in the number and size of type I and II fibers and decrease in the number of motor units;
(v) Exercise training for preventing sarcopenia are of considerable importance;
(vi) Aerobic exercise seems to have quite minor beneficial effects to prevent the aging effects in muscle system;
(vii) Reduction of maximal strength and power output will increase the disabilities and functional capacity to perform everyday tasks;
(viii) ACE I/D and the ACTN3 R577X5 polymorphisms have relative contribution to individual variability in muscle phenotypes in older people. According to our best knowledge have yet to be investigated;
(ix) The decline in food intake may conditioned the ideal weight for older subjects because of malnutrition;
(x) Participation in regular resistance training focused on strength and power exercises is the preferred strategy to attenuate and reverse the age-related loss of muscle mass and function;
Regarding to the state of the art, researchers should aim future investigation in order to explore issues that are not completely clear in the available literature. Some of those main topics can be:
(i) The effects of strength training in muscular mass and performance focus on explosive exercises in older women;
(ii) The interaction between exercise and nutrition in older population;
(iii) The interaction between muscular performance and genetic variation before and after a program training;
(iv) Association between muscle phenotypes (maximal strength, power and functional capacity) in this population and complex gene-gene and gene-environment interactions.
Muscle tissue changes with aging
Chapter 3 – Experimental Studies
Study 1. Effects of high-speed power training on functional
capacity and muscle performance in older women
Effects of high-speed power training on functional capacity and muscle performance
Abstract
The purpose of the study was to examine the effects of 12 weeks high-speed power training on isometric contraction (handgrip strength), maximal strength (1RM), muscle power (walking velocity, counter movement jump and ball throwing) and functional tasks of the arm and leg muscles (sit-to-stand and get-up and go). Fifty-six older women were divided into an experimental group and a control group [EG, n = 28, 62.5 (5.4) years; CG: n = 28, 62.5 (4.3) years]. The EG was submitted to a high-speed power training that consisted of 40% of one repetition maximum (1˂RM) to 75% of 1RM); 3 sets 4–12 reps, countermovement jump and medicine ball (1.5 kg) throwing. Over the 12-week training period, the EG significantly increased dynamic and isometric strength performance (57% to 61%), muscle power (range from 14% to 40%) (P˂0.05) and function (P˂0.05). No significant magnitudes of increase were observed in the CG. These data indicate that high-speed power training is an effective exercise approach leading to large gains in upper and lower extremity muscle performance and function capacity.
Effects of high-speed power training on functional capacity and muscle performance
Strength training, detraining and muscular genotypes in older women
20
Introduction
In older populations, maintenance of muscle power output is a key factor in everyday task performance, such as climbing stairs, rising from a chair and walking, as well as in decreasing the likelihood of falls, especially in women (Häkkinen et al., 1998; Izquierdo et al., 2001; Bonnefoy et al., 2007; Arnold et al., 2010). Resistance training (RT) in older people encourages slow-velocity contractions at a relatively high percentage of maximal strength (50–80%) to improve muscle strength and power (Porter, 2006). Recently, muscle power training has emerged as an important method in stimulating overall functioning capacity in the elderly (Häkkinen et al., 1998; Izquierdo et al., 2001). Indeed, a markedly lower capacity for concentric contractions may result in impaired performance, particularly in activities where intense and rapid movements are essential as, for example, avoiding oncoming traffic, counteracting a forward fall, climbing steps or crossing the road (Caserotti et al., 2008). The effectiveness of traditional resistance training programs on older populations has recently been questioned since these protocols in untrained older adults do not include fast and explosive activities (Häkkinen et al., 1998; Izquierdo et al., 2001). In fact, few studies have examined the effects of high-speed power training on maximal strength, muscle power and function in older women (Häkkinen et al., 1998; Izquierdo et al., 2001; Caserotti et al., 2008; Webber and Porter, 2010). Understanding the use of explosive training programs in older women is an important task for this relatively unstudied age group. The purpose of this study was therefore to examine the effect of a 12-week high-speed power training program for muscle strength and power development in older women. We hypothesized that a higher velocity RT in this population could be highly effective in promoting significant changes in strength and power values as well as in functional tasks.
Material and Methods
Subjects
Fifty-six older Caucasian women were divided into two groups (hereafter EG and CG): the experimental (age: 62.5±5.4 years; body mass: 68.2±11.2 kg; height: 1.55±0.06 cm) and the control (age: 62.2±4.3 years, body mass: 66.2±10.9 kg and height: 1.57±0.06 cm) each one with 28 participants. Efforts were made to recruit subjects so as to form comparable groups. Apart from routine daily tasks, the experimental group (EG) underwent a resistance training program of three training sessions per week over 12 weeks. The control group did not undergo any specifically orientated physical activity. None of the participants had a history of resistance training. Before inclusion in the study, all candidates were thoroughly screened by a physician. A written informed consent was obtained from each participant. The experimental procedures were approved by the University of Trás-os-Montes and Alto Douro, Department of Sport Sciences, following the Helsinki declaration.
Effects of high-speed power training on functional capacity and muscle performance
Testing procedures
The evaluation process requires reliability, specificity and facility of application, especially when subjects are sedentary and inexperienced. We thus selected protocols that were time-economical and that had been previously used in several studies for the assessment of musculoskeletal function in older people (Häkkinen et al., 1997; Häkkinen et al., 2000; Tolea et al., 2010). All testing procedures were applied to both groups before the experimental period (T1) and after 12 weeks of training (T2). Testing (T1 and T2) took place over a period of three days (three sessions separated by 3 to 5 days), always in the same location and time and supervised by the same researchers. In the first session, all subjects were assessed on anthropometric factors: weight, height, blood-pressure, resting heart rate; some functional parameters (the get-up-and-go test and the sit-to-stand test) and maximum isometric handgrip strength. The second session (3 days later) involved measures of power (maximum walking velocity, vertical jump and medicinal ball throwing) and maximum dynamic strength (one-repetition maximum bench press and leg extension). Before testing, each subject was familiarized with all strength testing procedures, preceded by a general warm-up routine. Verbal encouragement was given throughout the voluntary test and biofeedback provided in order to maximize motivation.
Anthropometric measures
Total height (m) and body weight (kg) were assessed according to international standards for anthropometric assessment (Marfell-Jones et al., 2006). To evaluate height (cm) a stadiometer (SECA, model 225, Germany) with a scale range of 0.10 cm was used and body mass (kg) was measured to the nearest 0.1 kg using a digital scale (Philips, type HF 351/00). These parameters were assessed prior to any physical performance test. Subjects were tested whilst wearing shorts and tshirts (shoes and socks were removed).
Strength tests
One repetition maximum leg-extension: Lower-body maximal strength was assessed using one
repetition maximum leg-extension (1RMLE) (Izquierdo et al., 2005). The shoulders were in contact with the machine, and the starting point knee angle was 90° measured with a goniometric. On command, the subject performed a concentric leg extension (as fast as possible) starting from the flexed position to reach the full extension of 180° against a resistance determined by given weight plates. Specific warm-up was allowed consisting of 1 set of 5 repetitions at 40–60% of the perceived maximum. Thereafter, 4 to 5 separate attempts were performed until the subject was unable to extend the legs to the required position. The last acceptable extension with the highest possible load was determined as 1RMLE.
Effects of high-speed power training on functional capacity and muscle performance
Strength training, detraining and muscular genotypes in older women
22
One repetition maximum bench press: Each subject was tested for maximal bilateral
concentric one-repetition bench press (1RMBP). In the 1RMBP concentric performance, the bar was positioned 1 cm above the subject's chest, supported by the bottom stops of the measurement device. The subject was instructed to perform from the starting position a purely concentric action maintaining the shoulders in a 90° abducted position (Newton et al., 1997). Specific warm-up was allowed. Thereafter, three to four trials were performed until the subject was unable to reach the fully extended position of the arms. The last acceptable extension with the highest possible load was determined as 1RMBP.
Maximum isometric handgrip: Maximum isometric strength of the forearm muscles (handgrip
test) was measured in both hands (dominant — HGd; non-dominant — HGnd), using an adjustable mechanical hand dynamometer (Lafayette Instrument, Lafayette, IN). After a standard warm-up period, the subject was placed seated on a chair in an erect position with the 90° hip, knee and elbow flexion position. The subjects were then instructed to exert maximal grip over three trials, with brief pauses (3 min) between each attempt, the best result being chosen for analysis (Haidar et al., 2004).
Power tests
Vertical jump: A trigonometric carpet (Ergojump Digitime 1000; Digitest, Jyvaskyla, Finland)
was used to assess maximum height in counter-movement jump (CMJ) (Marques et al., 2008). Each subject started from an erect standing position and the end of the concentric phase corresponded to a full leg extension (180°). The test was performed three times, each separated by a 2-minute rest period. The average maximum height of three trials was adopted and expressed in centimeters (cm).
Medicine ball throwing: Ball throwing performance (BT) was tested with a 1.5 kg medicine
ball (Ø 0.60 m). Prior to commencement, the participants were familiarized in throwing with different weighted balls in order to avoid a learning effect. Each subject sat on a chair with the posterior trunk region positioned against the chair back and held the ball to the front with both hands. They were instructed to throw the medicine ball as far and fast as possible. Torso and hip rotation was not allowed. Three approved attempts were made with one-minute rest intervals between each attempt to ensure that fatigue or learning effects did not influence the performance. The maximal throwing distance was determined using a flexible steel tape. Only the best attempt was used for further analysis (Marques et al., 2008).
Walking velocity: Subjects were instructed to perform three maximum effort sprints of 10 m
(S10) (Holviala et al., 2006) beginning 2 m before the start line, in order to achieve optimal velocities over the test distance. Time at 0–10 m (S10) was recorded using Micrograte equipment (Racetime2 Light Radio Kit, USA). Subjects performed trial sprints, separated by 3 min of rest, in an indoor rubberized track.
Effects of high-speed power training on functional capacity and muscle performance
Functional tasks
Walking 2.44 m, turning, and returning to seated position “get-up and go”: This test (GUG)
enables dynamic balance assessment, represented by the total time required for the subjects to rise from a seated position, walk eight feet (2.44 m), turn and return to a seated position. Subjects were instructed to sit on the chair with back straight, feet flat on the floor, and hands on thighs (Rikli and Jones, 1999). The timer was started on the signal “go” whether or not the participant actually started to move and terminated when the subject sat back down on the chair. The procedure was visually demonstrated in advance, and each participant was allowed to practice it once. Following the practice, two test trials were administered.
Sit-to-stand test: Before starting the 30-second sit-to-stand test (STS) a straight-backed chair
was placed next to a wall; subjects were asked to flex their arms across the chest and to stand up from a seated position on the chair. From the sitting position, the subject stood up to full height, then completely back down, this cycle being repeated as quickly as possible for 30 s. The total number of repetitions was recorded. Where the subject was in process of completing a full stand from the sitting position when the time elapsed, the final stand was counted in the total (Hallage et al., 2010).
High-speed power training protocol
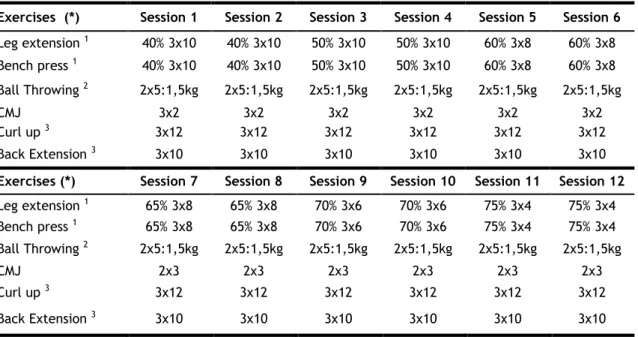
The RT program consisted of three sessions per week over 12 consecutive weeks. Table 1 provides a detailed description of the training program. The RT program was supervised by two resistance training specialists to ensure that the participants correctly followed the training schedule.
Effects of high-speed power training on functional capacity and muscle performance
Strength training, detraining and muscular genotypes in older women
24
Table 1. High-speed power training between week 1 and week 12.
Exercises (*) Session 1 Session 2 Session 3 Session 4 Session 5 Session 6
Leg extension 1 40% 3x10 40% 3x10 50% 3x10 50% 3x10 60% 3x8 60% 3x8 Bench press 1 40% 3x10 40% 3x10 50% 3x10 50% 3x10 60% 3x8 60% 3x8 Ball Throwing 2 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg CMJ 3x2 3x2 3x2 3x2 3x2 3x2 Curl up 3 3x12 3x12 3x12 3x12 3x12 3x12 Back Extension 3 3x10 3x10 3x10 3x10 3x10 3x10
Exercises (*) Session 7 Session 8 Session 9 Session 10 Session 11 Session 12
Leg extension 1 65% 3x8 65% 3x8 70% 3x6 70% 3x6 75% 3x4 75% 3x4 Bench press 1 65% 3x8 65% 3x8 70% 3x6 70% 3x6 75% 3x4 75% 3x4 Ball Throwing 2 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg 2x5:1,5kg CMJ 2x3 2x3 2x3 2x3 2x3 2x3 Curl up 3 3x12 3x12 3x12 3x12 3x12 3x12 Back Extension 3 3x10 3x10 3x10 3x10 3x10 3x10
1: Example: 40%: 3 ×10: 3 sets of 10 reps with 40% of 1RM.
2: Example: 2 ×5: 1.5 kg — 2 sets of 5 reps with a 1.5 kg medicinal ball. 3: Example: 3 ×12: 3 sets of 12 reps.
(*) Rest intervals of 2 min were permitted between sets and between categories.
The control group was permitted the same recreational and social activities as the experimental group. After a 10 minute warm-up, which included brisk walking and several joint mobilization exercises, the leg extension and bench press training was initiated. Subjects performed 3 sets of 10 reps with a load of 40% of 1RM at the outset of their predetermined 1-repetition maximum up until 3 sets of 4 reps with load of 75% towards the end of the 12-week period. In each session, they performed curl-ups (3 sets of 12 reps) and lumbar exercises (3 sets of 10 reps). Two power exercises were then performed: the counter movement jump and medicine ball throw (1.5 kg). Rest intervals of 2 min between sets and 3 min between exercises were deployed. Although utilizing the bench press and leg extension, the program gradually progressed so that the subjects were performing all exercises at high velocity, with instructions to do them “as fast as you can”. Before completing the session, the participants performed a few exercises to improve stability, balance and stretching. The RT was conducted every Monday, Wednesday and Friday (10:00 p.m.), throughout the 12 weeks of training (during Spring 2011). The subjects did not undertake any additional formal strength training activities during the testing or training period. Each RT session lasted for approximately 60 min including the warm-up period.
Statistical analysis
Standard statistical methods were used for the calculation of means and standard deviations. The normality and homoscedasticity assumptions were checked respectively with the Shapiro– Wilk and the Levene Tests. The training-related effects were assessed using a two-way ANOVA with repeated measures (groups × time). Results were significant in the interaction (P≤0.05). A significant F value was observed (F = 46.0, P = 0.000). A t-test for independent samples