Melissa de Oliveira Melchior1, Marcelo Oliveira Mazzetto2, Cláudia Maria de Felício3
Temporomandibular disorders and parafunctional oral habits:
An anamnestic study
Objective: To assess the frequency and severity of the signs and symptoms of temporomandibular disorders (TMD), the frequency of parafunctional oral habits and the correlation between the variables by means of the pa-tients’ perception regarding their problem.
Methods: One hundred patients diagnosed with TMD, through a clinical examination of their masticatory system, answered the questions of a previously published protocol concerning the signs and symptoms most frequently reported in the literature.
Results: According to the results from the non parametric statistical analysis, the frequency for the following signs and symptoms was significant: Fatigue and muscle pain, joint sounds, tinnitus, ear fullness, headache, chewing impairment and difficulty to yawn (p<0.01) and otalgia (p<0.05). As to the parafunctional oral habits, there was a significant presence of teeth clenching during the day and night (p<0.01) and teeth grinding at night (p<0.05). The variable correlation analysis showed that there was a positive correlation between symptom frequency and sever-ity; age was correlated with the presence of otalgia, cervical pain and teeth sensitivity, besides being correlated with muscle and joint pain severity. Habit frequency was negatively correlated with age. TMD duration was also positively correlated with the symptoms of tinnitus, ear fullness, muscle and joint pain.
Conclusion: The study results showed that the anamnestic assessment using ProDTMMulti can predict the sever-ity of the TMD case.
Keywords: Temporomandibular Joint disorders. Signs and symptoms. Habits.
How to cite this article: Melchior MO, Mazzetto MO, Felício CM. Temporoman-dibular disorders and parafunctional oral habits: An anamnestic study. Dental Press J Orthod. 2012 Mar-Apr;17(2):83-9.
Submitted: August 27, 2008 - Revised and accepted: December 30, 2009
» The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
Contact address: Melissa de Oliveira Melchior
Av. do Café, s/n. – CEP: 14.040-904 – Ribeirão Preto/SP – Brazil E-mail: [email protected].
1 Speech Pathologist, School of Dentistry of Ribeirão Preto - USP;
2 Head Professor, Department of Restorative Dentistry, School of Dentistry of
Ribeirão Preto - USP;
3 Professor, Department of Ophthalmology, Otolaryngology and Surgery of Neck and
INTRODUCTION
Temporomandibular disorders (TMD) have been recognized as a common condition of orofa-cial pain and its clinical manifestation includes a set of signs and symptoms. Among them, pain al-most always takes a prominent role, which can im-pair the functioning of the stomatognathic system and the quality of life.7,21,36 TMD diagnosis is mainly clinical and maybe supplemented by images.43 But often what drives the patient to seek treatment is the sign and symptom perception.
Pain in the masticatory muscles and temporo-mandibular joint (TMJ), difficulty in jaw move-ment, joint sounds, difficulties related to stomato-gnathic functions and otologic symptoms are com-monly reported by affected subjects.7,26
It is believed that habits can act as an important etiologic factor of TMD, as they lead to a traumat-ic dental occlusion that may affect the teeth and the masticatory muscles and temporomandibular joints, causing the disruption of the functional balance stomatognathic system, or worsening the already installed TMD.16,19,30,31,32 Thus, some studies have reported that the amount, frequency, inten-sity and duration of habits can determine the se-verity of signs and symptoms of TMD, as they re-late to fatigue and muscle pain, in addition to joint compression.13,15,30
Onychophagy, gum chewing, biting or clench-ing objects between the teeth, constantly bitclench-ing cheeks and lips, resting the jaws on the hands, clenching and/or bruxism, among other habits, are commonly reported by TMD patients.16,31,32
Studies have shown that anamnestic investiga-tion is valid for the identificainvestiga-tion of TMD14 and it may also give positive correlations with clinical findings.14,28 Previously, our team standardized the patient records about signs and symptoms of TMD, which allowed the definition of the frequency and severity of the condition, as well as verification of the treatment effects.13
The objective of this study was to determine the frequency and severity of TMD signs and symptoms and the frequency of deleterious oral habits present in a sample by means of a questionnaire to assess self-perception of symptoms, and to examine pos-sible correlations between the variables: Age of the
subjects, severity of symptoms, frequency of signs and symptoms, number of habits, duration of TMD.
MATERIAL AND METHODS
The project was approved by the Ethics Committee of the School of Dentistry of Ribeirão Preto, Univer-sity of São Paulo (process number 2001.1.266.58.5). All subjects were informed about the objectives of the study and signed an informed consent.
One hundred female subjects, with ages ranging from 11 to 74 years (mean 33.49 years) participated in this study. They were choose because they were the majority seeking for treatment on the waiting list.
Procedures
The patients were called for treatment of TMD, in a waiting list of the university.
The inclusion criterion was to present classifi-cation of muscular and/or articular TMD accord-ing to Research Diagnostic Criteria for Temporo-mandibular Disorders (RDC/TMD),9 applied by a trained examiner. Therefore, the subjects should have TMD signs and symptoms and the presence of pain in the masticatory muscles and/or the tem-poromandibular joint, limitation or deviation of mandibular movements, TMJ sounds and static and/or unusual dynamic occlusal relationship.7
Exclusion criteria were patients with central or peripheral neurological disorders, or who had suf-fered trauma or tumors in the head and neck.
The subjects were examined while seated in a dental chair with adequate lighting. To check the conditions, morphofunctional evaluation was made of the static and dynamic occlusion. To iden-tify the regions of pain, it was performed palpation of the masseter, temporal, suprahyoid, medial and lateral pterygoid, the insertion of the temporalis muscles (intraoral) and TMJs. The region of TMJ was also palpated during mandibular motion for the identification of joint noises, which were con-firmed by auscultation. Clinical examination was carried out based on the criteria required by the protocol RDC/TMD.9
(ProDTMMulti), which contains 2 parts. Patients answered questions of the first part of the proto-col, which admitted only affirmative or negative answers about the signs and symptoms and dele-terious oral habits. In the second part, they were asked to express the severity of signs or symptoms questioned according to the situation, that is, at waking up, chewing, speaking and at rest, using a 11-point numerical scale, with the help of a printed graduated scale: Zero was considered complete absence of symptoms or signs, and 10 the greatest severity possible. The severity scale was composed by the sum of the scores assigned to each sign and/ or symptoms in the four questioned situations. The procedures were performed individually and patients’ responses to each item were marked by the same examiner in the protocol.
To obtain data on deleterious oral habits, sub-jects were asked about the presence of the follow-ing behaviors: Clenchfollow-ing durfollow-ing day and/or night-time, grinding teeth during day and/or nightnight-time, chewing gum, biting objects and nails, and some other habit that had not been questioned. The sub-jects should answer each question with affirmative or negative answers.
Analysis of data
The data were described in terms of frequencies and analyzed using nonparametric statistics. The binomial test was employed to analyze the pres-ence of significance in relation to the abspres-ence of signs and symptoms of deleterious oral habits and Spearman correlation analysis for the correlation between the variables: Age of the subjects with the severity of symptoms and the number of habits; se-verity of symptoms with a duration of TMD, with the frequency of signs and symptoms and the num-ber of deleterious oral habits.
RESULTS
In this study, 65 out of 100 subjects had 21 to 40 years, 11 patients with less than 21 years and 24 subjects with more than 40 years. The time between the first symptoms reported by patients and the first assessment date in FORP/USP ranged from 1 to 23 years.
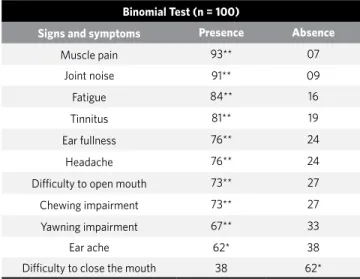
In this sample, there was significant presence
of signs and symptoms of muscle pain, joint noise, fatigue, tinnitus, ear fullness, headache, difficulty opening the mouth, chewing and yawning impair-ment (p <0.01) and otalgia (p <0.05).
A significant number of patients did not related difficulty to close the mouth. The frequencies and levels of significance are shown in Table 1.
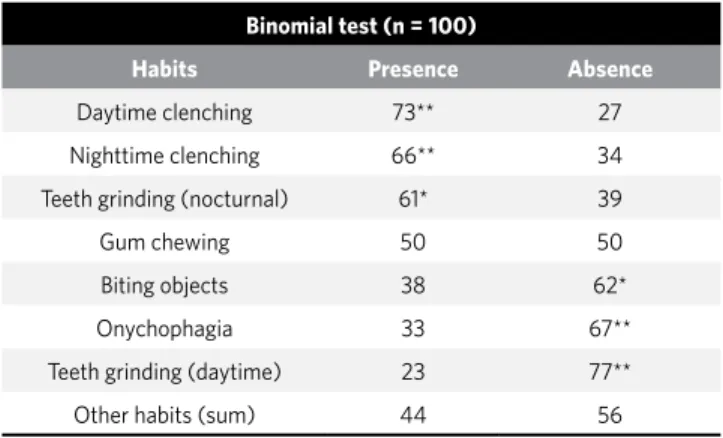
Frequency of deleterious oral habits
Only four sample subjects reported no delete-rious oral habits. Thirty-five reported 1 to 3 hab-its, while 61 subjects reported having 4 to 8 habits. There were reports of significant presence from di-urnal and noctdi-urnal clenching (p <0.01) and grind-ing of teeth at night (p <0.05). The other deleteri-ous habits did not show significant presence in the sample or their absence were significant (Table 2).
Correlations
The age of subjects was positively correlated to the severity of muscle pain (r = 0.26, p <0.01), TMJ pain (r = 0.28, p <0.01), ear ache (r = 0.32, p <0.01), neck pain (r = 0.27, p <0.01) and tooth sensitiv-ity (r = 0.28, p <0.01). Also the length of the TMD was related to the severity of muscle pain (r = 0.37, p <0.01), TMJ pain (r = 0.28, p <0.01), tinnitus (r = 0.21, p <0.05) and ear fullness (r = 0.21, p <0.05).
Table 1 - Frequency of TMD symptoms and noise signs present in the sample.
Binomial test: *0.05 level of significance; **0.01 level of significance. Binomial Test (n = 100)
Signs and symptoms Presence Absence
Muscle pain 93** 07
Joint noise 91** 09
Fatigue 84** 16
Tinnitus 81** 19
Ear fullness 76** 24
Headache 76** 24
Difficulty to open mouth 73** 27
Chewing impairment 73** 27
Yawning impairment 67** 33
Ear ache 62* 38
There were positive and significant correlation between the number of symptoms and the sever-ity of each TMD sign and/or symptoms (p <0.001). Sample distribution according to the severity of each sign and/or symptom, and the Spearman cor-relation coefficients are shown in Table 3.
The frequency of habits was negatively correlated with age of the subjects (r = 0.24, p <0.05). There was no significant correlation between the number of deleterious oral habits and TMD severity (p> 0.05).
DISCUSSION
The time between the first symptoms reported by patients and the date the first assessment in FORP/ USP ranged from 1 to 23 years, indicating that the treatment usually begins at the stage of chronic or recurrent disorder. The duration of symptoms is far beyond the time established by the International Association for the Study of Pain (IASP) in 199423 to describe a clinical state of chronic pain, which would be at least 6 months history of pain, and more an attempt to unsuccessful treatment.
By the variety of symptoms present in TMD, it is common that people affected by the problem look different professionals and specialists such as neurologists, otorhinolaryngologists and general practitioners before arriving and/or referred to a specialist service in DTM,11 which ends up making
Table 2 - Frequency of deleterious oral habits in the studied sample.
Table 3 - Distribution of absolute frequencies of the severity of the TMD signs and symptoms and Spearman correlation coefficients (r) between the number of signs and symptoms and the severity of each one.
Binomial test: *0.05 level of significance, **0.01 level of significance.
**0.01 level of significance; *** 0.001 level of significance.
treatment to be initiated already in a chronic stage of the disorder. This suggests the existence of diffi-culties in reaching the correct diagnosis and, conse-quently, to indicate the most appropriate treatment for each case, which in turn may be due to a lack of consensus on the methods of diagnosis, lack of preparation of professionals to recognize dysfunc-tion and difficulty in identifying the etiology.19,46 In addition, there is the fact that many patients seek treatment only when the disorder is recognized by them due to the increased symptomatology.
Binomial test (n = 100)
Habits Presence Absence
Daytime clenching 73** 27
Nighttime clenching 66** 34
Teeth grinding (nocturnal) 61* 39
Gum chewing 50 50
Biting objects 38 62*
Onychophagia 33 67**
Teeth grinding (daytime) 23 77**
Other habits (sum) 44 56
Severity of TMD Signs and Symptoms
Symptoms Grade 0 Grade 1
(1-10)
Grade 2 (11-20)
Grade 3 (21-30)
Grade 4
(31-40) r
Muscular pain 03 22 33 24 18 0.45***
TMJ pain 08 22 32 21 17 0.53***
Neck pain 12 25 22 22 19 0.48***
Ear ache 32 33 19 07 09 0.50***
Tinnitus 27 37 18 12 06 0.38***
Ear fullness 22 37 22 11 08 0.29**
Tooth sensitiveness 20 34 14 21 11 0.33**
In this study, subjects were selected based on RDC/TMD,9 which has been widely adopted as a method of classifying DTM.8,9,42,45 However, this is not the most appropriate method to understand the level of severity. Thus, we used the ProDTM-Multi previously constructed to standardize the records about the signs and symptoms of patients in multidisciplinary clinics, and to identify what are the signs and symptoms that affect the patient and their severity, and what are the most critical conditions on a daily basis.13
The significant presence of several signs and symptoms investigated in this study confirms the features found in other populations with TMD,6,13,19,46 as well as the presence of significant re-ports of day and nighttime clenching and grinding of teeth at night.30,31,32 Although these are expected results, because it is a preselected population with TMD, it was interesting to note the patient’s abil-ity to affirm or deny what they felt, which comple-mented the clinical assessments effectively. So this is confirmed as a useful method to identify a dysfunction,13 which can be easily applied by dif-ferent health professionals, as is their proposal.
Among the deleterious oral habits, bruxism has been considered an important maintenance fac-tor of TMD.15,18,31,32,41 The significant presence of diurnal and nocturnal clenching and teeth grind-ing (nocturnal) in this study, but not other hab-its, suggests the importance of bruxism on the progression and/or on non-remission of the dis-order, being the clenching a more important risk factor than grinding.6,15,30,31,40,41 And while Choi and Choung Moon6 have reported that bruxism cannot be a direct risk factor for TMD, there are reports showing that clenching was more often associated with TMJ symptoms and clinically relevant to the occurrence of the same, increasing the risk of man-ifestation of TMJ pain and noise and losses in the mouth opening.17,22,24,29,44
Therefore, a likely association between brux-ism and TMD signs/symptoms supports the theory that repetitive loads on the masticatory system can cause functional disorders.3
Regarding the positive correlation observed be-tween age and severity of signs and symptoms, it should be considered that only 24 sample subjects
had more than 40 years. Therefore, it did not neces-sarily mean that the more advanced the age of the subject, the greater the severity of the pain present in the TMJ and muscles. As recognized in the lit-erature, the age group most affected by TMD is the young and middle-aged adults.3,7,10,19,39 Epidemiolog-ical studies revealed that, unlike many other mus-culoskeletal conditions, the TMD has no increase in incidence or prevalence with increasing age.19,25
The higher frequency of TMD between 21 and 40 years of age over the older age groups was con-sidered suggestive of the influence of psychologi-cal tensions that are inherent to the time of great-est productivity of these individuals, over the pain-ful symptoms of TMD.5
The duration of the TMD was correlated with muscle pain, TMJ pain and tinnitus and ear full-ness. In the presence of pain and other symptoms, many compensations in the stomatognathic sys-tem can occur to allow that chewing, swallowing and speech might be carried out within the limit of efficiency and comfort. However, the actual compensation may have negative medium and long term effects, causing more imbalance and cu-mulative losses, because such compensations are not necessarily healthy2,47. Moreover, the process of chronic pain and the indiscriminate use of an-algesics without medical control, as often occurs among patients with TMD, may worsen the case.20,37
Significant relationships have been found be-tween the otologic symptoms and other TMD signs and symptoms,4,38 as well as the functional difficul-ties of the stomatognathic system.12
In the present study, we observed that the per-ception of severity of ear pain was correlated with the age of subjects. Meanwhile, the consciousness of severity of tinnitus and ear fullness symptoms was correlated with the duration of TMD, sug-gesting their association with TMD and not age-related ear problems. Earlier studies hypothesized that such symptoms may be caused by anatomical and functional relationships between the TMJ, the muscles innervated by the trigeminal nerve and the structures of the ear.1,27,33
symptoms, the greater the severity perceived by the patient. And, although several authors suggest that the habits accumulation can lead to worsening or contribute to no remission of the present scenar-io, and deleterious oral habits are among the TMD etiological factors,15,19,30,31,32 the frequency of hab-its was not correlated to the frequency or severity of signs and symptoms, according to data analyzed from ProDTMMulti13 in the current population. In a previous study, it was suggested that, in relation to bruxism, there is an effect of habit in time30. Prob-ably the intensity and duration are more important than the number of habits. However, according to the limits imposed by the instrument used in this study, such measurement was not possible.
There were no significant presence of gum chewing habits and onychophagia in our sample, as well as the correlation between habits and age was negative. Research conducted with student populations pointed that gum chewing and ony-chophagia are the main habits and classified them as juvenile habits.16,29
The nature of this investigation allowed us to know about TMD symptoms in the light of who suf-fers it, revealing the possibility of using the proto-col ProDTMMulti13 as a tool for identification of a
potential framework for TMD. Moreover, the pos-sibility to register information about the awareness and consciousness of the population studied in rela-tion to clenching and/or grinding of teeth facilitates the treatment plan, starting at the point of self con-sciousness to achieve some changes in behavior.11
CONCLUSION
24. Johansson A, Unell L, Carlsson GE, Soderfeldt B, Halling A. Gender differences in symptoms related to temporomandibular disorders in a population of 50-year-old subjects. J Orofac Pain. 2003;17(1):29-35.
25. Leresche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8(3):291-305. 26. Magnusson T, List T, Helkimo M. Self-assessment of pain and discomfort in
patients with temporomandibular disorders: a comparison of five different scales with respect to their precision and sensitivity as well as their capacity to register memory of pain and discomfort. J Oral Rehabil. 1995;22(8):549-56.
27. Malkin DP. The role of TMJ dysfunction in the etiology of middle ear disease. Int J Orthod. 1987;25(1-2):20-1.
28. Manfredi APS, Silva AA, Vendite LL. The sensibility appreciation of the questionnaire for selection of orofacial pain and temporomandibular disorders recommended by the American Academy of Orofacial Pain. Rev Bras Otorrinolaringol. 2001;67(6):763-8.
29. Miyake R, Ohkubo R, Takehara J, Morita M. Oral parafunctions and associations with symptoms of temporomandibular disorders in Japanese university students. J Oral Rehabil. 2004;31(6):518-23.
30. Molina OF, Santos J Jr, Mazzetto MO, Nelson SJ, Nowlin TA, Maineri ET. Oral jaw behaviors in TMD and bruxism: a comparison study by severity of bruxism. Cranio. 2001;19(2):114-22.
31. Molina OF, Santos J Jr, Nelson SJ, Grossman E. Prevalence of modalities of headaches and bruxism among patients with craniomandibular disorders. Cranio. 1997;15(4):14-25.
32. Molina OF, Santos J Jr, Nelson SJ, Nowlin T. A clinical study of specific signs and symptoms of CMD in bruxers classified by the degree of severity. Cranio. 1999;17(4):268-79.
33. Morgan DH, Goode RL, Christiansen RL, Tiner LW. The TMJ-ear connection. Cranio. 1995;13(1):42-3.
34. Mundt T, Mack F, Schwahn C, Benhardt O, Kocher T, John U, Biffar R. Gender differences in associations between occlusal support and signs of temporomandibular disorders: results of the population-based study of health in Pomerania (SHIP). Int J Prosthodont. 2005;18(3):232-9.
35. Nilsson IM. Reliability, validity, incidence and impact of temporomandibular pain disorders in adolescents. Swed Dent J Suppl. 2007;(183):7-86.
36. Okeson JP, Hayes DK. Long-term results of treatment for temporomandibular disorders: an evaluation by patients. J Am Dent Assoc. 1986;112(4):473-8. 37. Oliveira MF, Speciali JG. Cefaléia crônica diária: conceitos e tratamentos. Medicina.
2002;35(4):455-63.
38. Peroz I. Dysfunctions of the stomatognathic system in tinnitus patients compared to controls. HNO. 2003;51(7):544-9.
39. Rocha APF, Nardelli MR, Rodrigues MF. Epidemiologia das desordens
temporomandibulares: estudo da prevalência da sintomatologia e sua interrelação com a idade e o sexo dos pacientes. Rev Serviço ATM. 2002;2(1):5-10. 40. Rosseti LM, Araújo CRP, Rosseti PH, Conti PC. Association between rhythmic
masticatory muscles activity during sleep and masticatory myofascial pain: a polysomnographic study. J Orofac Pain. 2008;22(3):190-200.
41. Sato F, Kino K, Sugisaki M, Haketa T, Amemori Y, Ishikawa T, et al. Teeth contacting habit as a contributing factor to chronic pain in patients with temporomandibular disorders. J Med Dent Sci. 2006;53(2):103-9.
42. Schimitter M, Rammelsberg P, Hassel A. The prevalence of signs and symptoms of temporomandibular disorders in very old subjects. J Oral Rehabil. 2005;32(7):467-73. 43. Shintaku W, Enciso R, Broussard J, Clark GT. Diagnostic imaging for
chronic orofacial pain, maxillofacial osseous and soft tissue pathology and temporomandibular disorders. J Calif Dent Assoc. 2006;34(8):633-44. 44. Solberg WK, Woo MW, Houston JB. Prevalence of mandibular dysfunction in young
adults. J Am Dent Assoc. 1979;98(1):25-34.
45. Tartaglia GM, Silva MAM, Bottini S, Sforza C, Ferrario VF. Masticatory muscle activity during maximum voluntary clench in different research diagnostic criteria for temporomandibular disorders (RDC/TMD) groups. Manual Therapy. 2008;13(5):434-40.
46. Wassell RW, Adams N, Kelly PJ. Treatment of temporomandibular disorders by stabilizing splints in general dental practice: results after initial treatment. Br Dent J. 2004;197(1):35-41.
47. Willianson EH, Hall JT, Zwemer JD. Swallowing patterns in human subjects with and without temporomandibular dysfunction. Am J Orthod Dentofacial Orthop. 1990;98(6):507-11.
1. Arlen H. The otomandibular syndrome. In: Gelb H. Clinical management of head, neck and TMJ pain and dysfunction: a multi-disciplinary approach to diagnostic and treatment. Philadelphia: Saunders; 1985. p. 181-95.
2. Bianchini EMG. Articulação temporomandibular: implicações, limitações e possibilidades fonoaudiológicas. Carapicuíba: Pró-Fono; 2000.
3. Bove SRK, Guimarães AS, Smith RL. Caracterização dos pacientes de um ambulatório de disfunção temporomandibular e dor orofacial. Rev Latino-Am Enfermagem. 2005;13(5):686-91.
4. Camparis CM, Formigoni G, Teixeira MJ, Siqueira JT. Clinical evaluation of tinnitus in patients with sleep bruxism: prevalence and characteristics. J Oral Rehabil. 2005;32(11) 808-14.
5. Cauás M, Alves IF, Tenório K, HC Filho JB, Guerra CMF. Incidences of parafunctional habits and posture in with patients craniomandibular dysfunction. Rev Cir Traumatol Buco-maxilo-fac. 2004;4(2):117-24.
6. Choi YS, Choung PH, Moon HS, Kim SG. Temporomandibular disorders in 19-year-old Korean men. J Oral Maxillofac Surg. 2002;60(7):797-803. 7. Dworkin SF, Huggins KH, Leresche L, Van Korff M, Howard J, Truelove E,
Sommers E. Epidemiology of signs and symptoms in temporomandibular disorders: clinical signs in cases and controls. J Am Dent Assoc. 1990;120(3):273-81.
8. Dworkin SF, Huggins KH, Wilson L, Mancl L, Turner J, Massoth D, et al. A Randomized clinical trial using Research Diagnostic Criteria for temporomandibular disorders-Axis II to target clinic cases for tailored self-care TMD treatment program. J Orofac Pain. 2002;16(1):48-63.
9. Dworkin SF, Leresche L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J Craniomandib Disord Facial Oral Pain. 1992;6(4):301-55.
10. Esposito CJ, Panucci PJ, Farman AG. Associations in 425 patients having temporomandibular disorders. J Ky Med Assoc. 2000;98(5):213-5. 11. Felício CM. Fonoaudiologia nas desordens temporomandibulares: uma ação
educativa-terapêutica. São Paulo: Pancast; 1994. 179 p.
12. Felício CM, Faria TG, Silva MAMR, Aquino AMCM, Junqueira CA. Desordem temporomandibular: relações entre sintomas otológicos e orofaciais. Rev Bras Otorrinolaringol. 2004;70(6):786-93.
13. Felício CM, Mazzetto MO, Silva MAMR, Bataglion C, Hotta THA. Preliminary protocol for multi-professional centers for determination of signs and symptoms of temporomandibular disorders. Cranio. 2006;24(4):258-64.
14. Fonseca DM, Bonfante G, Valle AL, Freitas SFT. Diagnóstico pela anamnese da disfunção temporomandibular. RGO: Rev Gaúcha Odontol. 1994;42(1):23-8. 15. Fujita Y, Motegi E, Nomura M, Kawamura S, Yamaguchi D, Yamaguchi H. Oral
habits of temporomandibular disorder patient with malocclusion. Bull Tokyo Dent Coll. 2003;44(4):201-7.
16. Gavish A, Halachmi M, Winocur E, Gazit E. Oral habits and their association with signs and symptoms of temporomandibular disorders in adolescent girls. J Oral Rehabil. 2000;27(1):22-32.
17. Gesch D, Benhardt O, Alte D, Schwahn C, Kocher I, John U, et al. Prevalence of signs and symptoms of temporomandibular disorders in an urban and rural German population-based study of health in Pomerania. Quintessence Int. 2004;35(2):143-50.
18. Glaros AG, Burton E. Parafunctional clenching, pain, and effort in temporomandibular disorders. J Behav Med. 2000;27(1):91-100.
19. Gremillion HA. The prevalence and etiology of temporomandibular disorders and orofacial pain. Tex Dent J. 2000;117(7):30-9.
20. Headache Classification Committee of The International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia. 1988;8 Suppl 7:10-73.
21. Henderson DH, Cooper JCJR, Brayan GW, Van Sickels JE. Otologic complaints in temporomandibular joint syndrome. Arch Otolaryngol Head Neck Surg. 1992;118(11):1208-13.
22. Huang GJ, Leresche L, Critchlow CW, Martin MD, Drangsholt MT. Risk factors for diagnostic subgroups of painful temporomandibular disorders (TMD). J Dent Res. 2002;84(4):284-8.
23. International Association for the Study of Pain. Classification of chronic pain: descriptors of chronic pain syndromes and definitions of pain terms. 2nd ed. Seattle: IASP Press; 1994.