Revista Gaúcha
de Enfermagem
How to cite this article:
Moura LM, Shimizu HE. Social representa-tions of health councilors regarding the right to health and citizenship. Rev Gaúcha Enferm. 2016;37(spe):e70826. doi: http://dx.doi.org/10.1590/1983-1447.2016.esp.70826.
doi: http://dx.doi.org/10.1590/1983-1447.2016.esp.70826
Social representations of health councilors
regarding the right to health and citizenship
Representações sociais de conselheiros de saúde acerca do direito à saúde e da cidadania
Representaciones sociales de concejales de salud sobre el derecho a la salud y a la ciudadanía
a Escola Superior de Ciências da Saúde (ESCS), Curso
de Gradução em Enfermagem. Brasília, Distrito Fede-ral, Brasil.
b Universidade de Brasília (UnB), Faculdade de
Ciências da Saúde, Departamento de Saúde Coletiva. Brasília, Distrito Federal, Brasil.
Luciana Melo de Mouraa
Helena Eri Shimizub
ABSTRACT
Objective: To know the structure of the social representations of right to health and citizenship of health municipal councilors. Method: This is a qualitative study, based on the central nucleus theory of social representations, carried out in eight municipalities of the Integrated Region for the Development of the Surroundings of the Federal District, Brazil. The intentional sample consisted of municipal health councilors. Between June and December 2012, free recall questionnaires were used, of which 68 were answered with the inducing term health, and 64 with the inducing term citizenship. Data were analyzed using EVOC software and Bardin’s content analysis.
Results: The representational field of the right to health is associated with the idea of universal law guaranteed by the Constitution and the Unified Health System (SUS), and of citizenship linked to rights and duties.
Conclusions: The conceptions of right to health are understood as a condition for reaching citizenship, and citizenship as social protection.
Keywords: Right to health. Citizen participation. Health councils.
RESUMO
Objetivo: Conhecer a estrutura das representações sociais de direito à saúde e cidadania de conselheiros municipais de saúde. Método: Estudo qualitativo, fundamentado nas Teorias das Representações Sociais e do Núcleo Central, realizado em oito municípios da Região Integrada de Desenvolvimento do Entorno do Distrito Federal, Brasil. A amostra intencional foi composta por conselheiros municipais de saúde. Entre junho e dezembro de 2012 aplicaram-se questionários de evocação livre, dos quais foram respondidos 68 com o termo indutor Direito à Saúde e 64 com o termo indutor Cidadania. Os dados foram analisados por meio do software EVOC e
da análise de conteúdo de Bardin.
Resultados: O campo representacional de direito à saúde está associado à ideia de direito universal garantido pela Constituição e pelo SUS e de cidadania vinculado aos direitos e deveres.
Conclusões: As concepções de direito à saúde são entendidas enquanto condição para alcance da cidadania e cidadania como proteção social.
Palavras-chave: Direito à saúde. Participação cidadã. Conselhos de saúde.
RESUMEN
Objetivo: Conocer la estructura de las representaciones sociales de la salud y el derecho a la ciudadanía de la salud de concejales. Método: Estudio cualitativo basado en la teoría de las representaciones sociales y el núcleo central, realizado en los municipios de la región que rodea el Desarrollo Integrado del Distrito Federal, Brasil. Una muestra intencional fue compuesta por consejeros munici-pales de salud. Entre junio y diciembre de 2012 aplicaron cuestionarios de recuerdo libre, de los cuales fueron contestados 68 con el inductor del término derecho a la salud y 64 con el término ciudadanía inductor. Los datos fueron analizados utilizando el software EVOC y el análisis de contenido de Bardin.
Resultados: El campo representacional derecho a la salud se asocia con la idea del derecho universal garantizado por la Constitución y el SUS y la ciudadanía vinculada a los derechos y deberes.
Conclusiones: El derecho de los conceptos de salud se entiende como condición para el logro de la ciudadanía y ciudadanía como protección social.
INTRODUCTION
The right to health is part of social rights, being one of the most difficult to achieve, especially when considering civil and political rights, which require effective State actions through effective policies and programs(1). In this perspec-tive, besides the universal right to health, intersectoriality of health actions, the regulatory role of the State in relation to the health market, decentralization, regionalization and hierarchization of the system were included in the Unified Health System (SUS, as per its acronym in Portuguese).
Popular participation in health services was ensured through collegial bodies called conferences and health councils(3). These forums premise is the democratization of public management, and improvement of efficiency and effectiveness of social policies. However, the panorama shows that there is a low incorporation of the proposals of the conferences and that the councils have limited au-tonomy in the definition of public health policies, besides having a bureaucratic function(3-4).
The participation of the population and its organized groups in the management of health services represents a major step forward in representative democracy, because the right to health should be defined as a priority by the local community(5). The community, by expressing health needs, becomes able to define the extension of the con-cept of health and delimit the scope of freedom (individual right) and equality (collective right), which are the base of the right to health.
In this context, the struggle to guarantee the right to health ended up being the figures of citizen subjects, that is, political activists who seek to guarantee better living conditions for the population(6). This is, therefore, the exer-cise of citizenship, which takes place primarily as a practice of identification with public issues, that is, with issues of public interest. In other words, the exercise of citizenship is a daily practice(7).
Nonetheless, it should be noted that the search for guarantees of the rights to health, and the political activ-ism of the organized civil society has been incorporated into the coordination of neoliberalism, with the modes of subjectivation of the political claims themselves(6). As a re-sult, there is the risk of losing this right, which was hardly achieved in the health reform process, the universal cover-age of health services for all the population.
Based on this, it is important to understand how sub-jects behave and justify or position themselves in relation to their actions to defend the right to health and citizen-ship, since a citizen action is related to the guarantee of rights and to the exercise of democracy.
Accordingly, social representations of the right to health and citizenship of municipal health councilors can contribute to the design of restricted or comprehensive health care models, and also greatly influence municipal public health policies that are reverted into services ren-dered to the community.
Therefore, a question emerges: Which social represen-tations of right to health and citizenship permeate daily practices within municipal health councils? For this rea-son, this study had as objective to know the structure of social representations of right to health and citizenship of health councilors of municipalities of the Integrated Region for the Development of the Surroundings of the Federal District (RIDE-DF).
METHOD
This study is part of a thesis(8) that analyzed the organi-zation and dynamics of municipal health conferences and councils in order to reach users’ satisfaction.
The methodological design chosen was the qualitative research, based on the Social Representations Theory(9), along with the complementary proposal of the Central Nucleus Theory(10). This theory proposes that a social rep-resentation is organized around a central nucleus, which is formed by one or more elements that give meaning to the representation, and that, for this reason, are stable and define the homogeneity of a group. Around this central el-ement, or these central elements, the peripheral elements, considered the moving and evolutionary aspect of a rep-resentation, would be organized, with the function to reify, regulate and defend the central nucleus(10).
Using the structural approach of social representations, it is possible to access and identify the terms and expres-sions that better define and organize the representations of the right to health and citizenship, assisting in the anal-ysis of the common field, which corresponds to the beliefs shared by the municipal health councilors.
It is important to note that these municipalities are con-sidered as dormitory cities, and have a significant popula-tion contingent that, due to speculative home purchase in the territory of the Federal District, had to migrate to adja-cent cities. In these municipalities, there is a strong depen-dence on the Federal District for public health services; in addition, there is low average income among the majority of the population, and a high rate of informality in the labor market, where more than 80% of the population does not have private health insurance(12).
Thus, the municipalities were selected if they were rep-resentative of the RIDE-DF regions; had a population of more than 50,000 inhabitants, and held municipal health conferences every two years. Hence, the sample consist-ed of Municipal Health Councils of the South Surrounding regions (Cidade Ocidental, Novo Gama, Santo Antônio do Descoberto and Valparaíso, all in the state of Goiás); of the North Surroundings (Formosa and Planaltina, municipali-ties of Goiás); Region of Pirineus (Pirenópolis, Goiás); and the region of Unaí (Buritis of the state of Minas Gerais).
The intentional sample consisted of health councilors from the municipalities described above, with at least six months of office, present at the ordinary and extraordinary meetings of the councils from June to December 2012, and who volunteered to participate, totaling 68 subjects who answered the questionnaire on the inducing term
right to health, and 64 who responded as to the inducing term citizenship. Twenty-one meetings were followed for the application of the questionnaire. Councilors with less than six months in office, or who were absent from meet-ings or who refused to participate in the survey were ex-cluded from the sample.
The data collection instrument was a semi-structured and self-administered questionnaire, divided into three parts. The first part was intended for evocation, where the free evocation technique was used so that the council-ors could cite six words or expressions that occurred to them immediately in relation to the inducing terms right to health and citizenship. The second part used the tech-nique of hierarchy of items so that the councilors enu-merated, in order of importance, three words or expres-sions considered more important. The third part of the questionnaire was intended to justify in writing the three words or expressions considered of greater relevance for each inducing term. This free evocation questionnaire makes it possible to know mental elements quickly and objectively, by apprehending the elements of the cen-tral and peripheral nucleus of a representation, avoiding masking of elements through consciousness, as it hap-pens in the interview (13).
In order to identify the structure of the social represen-tations, the answers collected in the first part of the ques-tionnaire were submitted to the evocation analysis, through the software EVOC (Ensemble of Programmes Permettant l’Analyze des Évocations), version 2000, for the analysis of free evocations. This allows to identify not only the con-tent of the representations, but their internal organization based on a double criterion: frequency (freq.) versus av-erage evocation order (AEO). The closer the avav-erage is to one, the greater the importance of the indicated words. According to the assumption of the structural perspective of social representations, the association of these two crite-ria distributed in four quadrants reveals the probable cen-tral and peripheral elements of a social representation(10). Words with a high frequency, and to which the subjects attribute an importance in the definition of the object, and express a central and organizing sense of social represen-tation; therefore, they are more important in the cognitive arrangement. The words in the peripheral system have less frequency and distant evocation, and are important for pro-viding support to the central nucleus, as well as being more fluctuating to changes. The intermediate elements, located in the contrast zone, are expressed with low frequency, but with the next evocation by the subjects, or high frequency and distant evocation, and signal the existence of relevant differences in the representation when they deviate from the central elements, indicating the existence of a represen-tational subgroup(13). The analyses with the software of the words/expressions evoked from the inducing terms, right to health and citizenship, were carried out separately.
The organization of the data from the second part of the questionnaire was submitted to the centrality test. In this step, the words or expressions evoked after the enu-meration in order of importance in the EVOC software were analyzed, and their internal organization took place in frequency versus average order of importance (AOI) in order to proceed with the comparison with the free evo-cation order.
refers to the treatment of the results obtained and inter-pretation for proposition of inferences.
The present study was submitted to the Ethics Com-mittee of the Foundation for Teaching and Research of the Federal District, and approved under number 001/2012. All research subjects had voluntary participation and signed a free and informed consent form.
RESULTS AND DISCUSSION
The analysis performed with the EVOC software al-lowed the identification of the probable central elements,
that is, those that give meaning and organize the represen-tation, as well as the probable elements of the periphery of the social representation of right to health (Table 1).
The data obtained from the analysis of free associations of the inducing term right to health (Table 1) revealed two important elements in the central nucleus: Constitution and SUS. These elements characterize the legal instruments for the materialization of this right, as well as the idea of accessibility and everyone’s right. In the second quadrant, there are the terms that are probably part of the peripher-al system closest to the centrperipher-al nucleus, where the right to health and the right to receive medicines appeared as the
Central Nucleus Peripheral System – First Periphery
1st Quadrant Frequency >= 8
Average Order of Evocation <3
2nd Quadrant Frequency >= 8
Average Order of Evocation >=3 Evoked Term accessibility constitution everyone’s rights SUS Freq. 8 11 16 10 AEO 2.625 2.000 2.000 2.300 Evoked Term medication responsibility Freq. 11 9 AEO 3.182 3.556
Peripheral System – Contrast Zone Peripheral System – Second Periphery
3rd Quadrant Frequency < 8
Average Evocation Order <3
4th Quadrant Frequency <8
Average Evocation Order >=3 Evoked Term care citizenship citizen commitment health council state obligation rights exams fundamental hospital equality taxes comprehensiveness legislation physician denied Freq. 6 7 5 6 4 7 3 3 3 6 6 4 3 7 5 4 AEO 2.333 2.571 2.200 2.833 2.500 2.714 2.333 2.000 1.333 2.333 2.500 2.500 2.333 2.429 2.800 1.000 Evoked Term basic care communication knowledge education humanization elderly financial resources respect treatment universality Freq. 3 3 7 3 5 4 3 4 3 7 AEO 3.333 5.000 3.714 4.667 4.200 4.250 4.333 4.250 3.000 4.429 Table 1 – Quadrants with the structure of social representation of the municipal health councilors of the eight municipal-ities of the RIDE-DF on the term Right to Health – 2012
responsibility of the managers. In the third quadrant or con-trast zone emerged a representational subgroup formed by the idea of citizenship, where the citizen has the right to care, and it is the duty of the State to provide it, as well as the right to social participation, objectified in the health council. The issue of tax collection reinforces the idea of cit-izenship and right to health. In the more distant peripher-al system, right to heperipher-alth referred to the elements of basic care, communication, knowledge, education, the elderly, financial resources, respect, treatment and universality.
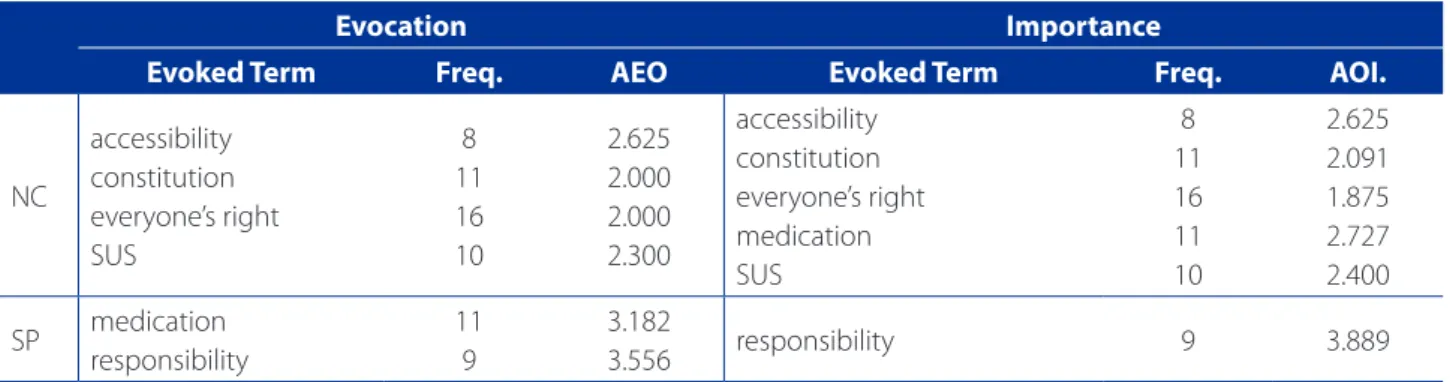
Table 2 presents the results of the centrality test of the term right to health for comparison of the elements of the central nucleus in average evocation order and in average order of importance.
When performing the centrality test, it was verified that the central elements of right to health (Table 2) remained in order of evocation, as well as in order of importance, re-inforcing the evidence that these elements make up the central nucleus.
It was found that the social representations of right to health of health councilors are anchored in the ideas of the Sanitary Reform that were approved by the VIII Na-tional Conference of Health in 1986, to strengthen the public health sector, to expand coverage to all citizens, aiming at establishing a unified health system(2). Another element evidenced was the Constitution, which is char-acterized as a legal instrument for materializing the uni-versal right to health.
Using the content analysis of the justifications of the three words or expressions of greater relevance for the inducing term right to health two thematic categories emerged.
The category named Right to Health revealed that the right to health is universal; however, a speech pointed
out that SUS is for the underprivileged. The councilors also revealed that the governors should ensure compliance with health laws regarding health, and convert taxes col-lected into the health system, since there is a need for in-vestment in the SUS. In addition, they showed the right to health as a conquest, the result of the collective struggle and that to guarantee it, the society should know the laws that support the SUS to demand their compliance by the public power, even through judicialization. Another idea that emerged on the subject was the supervision of the fulfillment of the right to health by health councils, public ministries, and courts of accounts. The collective discourse also highlighted that accessibility to appointments, diag-nostic exams, treatments, humanized and quality care reify this right.
The universal health system has allowed the accessibil-ity mentioned by the councilors of this study to appoint-ments, diagnostic exams, treatappoint-ments, and humanized and quality care. The right to health includes access to the re-sources needed to achieve health, the ability to withstand conditions that endanger health, health information and transparency, informed consent, and even the right to make a decision(15).
UNESCO, in 2005, through the Universal Declaration on Bioethics and Human Rights reaffirmed health as a funda-mental human right and that the population’s access to health care is essential to quality health, and should there-fore be the central objective of governments(16).
In the category called Full Health, other factors that influence health conditions, such as basic sanitation, hous-ing, employment, education, food, water quality, access to sports and leisure were pointed out. On the other hand, some councilors cited private health plans for access to dif-ferential treatment and better health, albeit at high costs.
Evocation Importance
Evoked Term Freq. AEO Evoked Term Freq. AOI.
NC
accessibility constitution everyone’s right SUS
8 11 16 10
2.625 2.000 2.000 2.300
accessibility constitution everyone’s right medication SUS
8 11 16 11 10
2.625 2.091 1.875 2.727 2.400
SP medication responsibility
11 9
3.182
3.556 responsibility 9 3.889
Source: Research data, 2012. Freq.= Frequency AEO= Average Evocation Order AOI= Average Order of Importance
It was verified that the councilors, when referring to the
right to health, went beyond the field of health, since they pointed to other factors that influence health conditions, such as basic sanitation, housing, employment, education, food, water quality, access to sport and leisure, as demon-strated in the theme category Full Health. Accordingly, health systems and their governments, in order to guaran-tee the right to health, should work on the social and en-vironmental determinants of health, derived from the form of organization of production in society, and the inequal-ities that exist in it, emphasizing that the action on these factors should be the responsibility of all State sectors(2), considering the complexity of this right, as it achieves sev-eral spheres, including health, law, financial, educational, technological, housing, sanitation and management
pol-icies(17). Thus, the right to health has been closely related to other human rights such as human dignity, life, non-discrimination, equity, prohibition against torture, privacy, access to information, and freedom for organizing associa-tions, meetings, and movements(18).
Nonetheless, in the Full Health thematic category, the complementary health network was considered of better quality when compared to public services, showing strong indications of a progressive penetration of private interest in the public health system. This contrasts with the perspective of the Sanitary Reform, which defended the creation of a public and universal health system, where private initiative would be established in a complementa-ry manner, with the perspective of its gradual reduction in the context of the SUS(6).
Central Nucleus Peripheral System – First Periphery
1st Quadrant Frequency >= 13
Average Evocation Order <3
2nd Quadrant Frequency >= 13
Average Evocation Order >=3 Evoked Term
obligations rights respect
Freq. 20 27 19
AEO 2.600 1.556 2.526
Evoked Term Freq. AEO
Peripheral System – Contrast Zone Peripheral System – Second Periphery
3rd Quadrant Frequency < 13
Average Evocation Order <3
4th Quadrant Frequency <13
Average Evocation Order >=3 Evoked Term
action constitution right to health equality
social participation health
empathy union vote
Freq. 3 3 3 4 10
6 7 3 6
AEO 1,667 2,000 1.000 2.500 2.400 2.833 2.714 2.000 2.500
Evoked Term citizen collectivity commitment knowledge dignity education job ethics humanization mobilization housing responsibility sanitation society
Freq. 5 3 3 6 5 6 5 3 3 4 3 6 4 8
AEO 3.200 4.000 3.333 4.167 3.800 3.833 3.600 3.667 6.000 4.500 4.667 3.500 4.750 4.250 Table 3 – Quadrants with a structure of social representation of municipal councilors of eight municipalities of the RIDE-DF on the term Citizenship – 2012
In this direction, health councils are extremely relevant, especially to vocalize the defense of health as a public good. Community-based participation is also be important to ensure access to a wide range of health promotion, pre-vention, curative and rehabilitation health services(19).
The analysis with the software EVOC revealed the rep-resentational structure of the term citizenship (Table 3) from the arrangement of the elements in the upper left quadrant or central nucleus, upper right quadrant or first periphery, lower right quadrant or second periphery and lower left quadrant called contrast zone.
Regarding the free evocation of the inducing term citi-zenship (Table 3), the analysis showed, in the central nucle-us, the elements of exercise of rights, fulfillment of obliga-tions, and respect. The second quadrant that corresponds to the peripheral system that is closest to the central nu-cleus appeared empty. In the third quadrant or contrast zone a representational subgroup appeared, formed by the idea of citizenship associated with action, based on the constitution, which guarantees the right to health, equali-ty, social participation and voting, and that there is a need for solidarity and union among people. In the most distant peripheral system, citizenship referred to the conditions for a person to be recognized as a citizen.
Table 4 presents the result of the centrality test of the term citizenship for comparison of the elements of the cen-tral nucleus in average evocation order and in average or-der of importance.
When performing the centrality test, it was seen that the central elements of the term citizenship (Table 4) re-mained in order of evocation and in order of importance, indicating that these elements probably form the central nucleus because they resist to the test.
The social representations of citizenship of the council-ors are anchored in theoretical and philosophical frame-works that were the basis for the citizen’s constitution, by presenting in the central nucleus the right elements,
obli-gations, and respect. In the Brazilian constitution, citizen-ship is guaranteed in three areas: civil, social and political rights. Hence, the civil rights of individual freedom preser-vation, such as contract, property, expression, conscience; political rights of representation and participation; and so-cial rights, which are aimed at avoiding the worst effects of capitalism, with the right to health, education, food, labor, housing, leisure, safety, social security, maternity and child protection, and assistance to the disadvantaged were relat-ed to the citizen’s condition(18). In short, the term citizenship has contemplated the rights, obligations, as well as respect to the laws that the citizen has in relation to the country where he/she was born or chose to live in.
Two thematic categories emerged from the content analysis of the justifications of the three words or expres-sions of greater relevance for the inducing term citizen.
The category called Social Activism revealed that the rights, respect for the laws and neighbors, and the fulfill-ment of obligations were considered the basic principles of citizenship. In addition, the set of rights allowed social activism and participation in public life. In this sense, an individual is considered a citizen when he/she is aware of his/her rights and obligations. Among their obligations, they mentioned voting, here put as the greatest expression of citizenship.
These findings revealed that citizenship encompasses a set of rights that allow the active participation of individ-uals in public affairs. Participation would take place, con-cretely, from the choice of governors, through the electoral process, with representative democracy guaranteed in the constitution, as demonstrated in the thematic category Social Activism.
However, this has proved to be insufficient to address the problems presented by most of the population. Thus, participatory democracy mechanisms are adopted as a po-litical, social and cultural strategy capable of guaranteeing the expansion of the public sphere, and greater
participa-Evocation Importance
Evoked Term Freq. AEO Evoked Term Freq. AOI.
NC
obligations rights respect
20 27 19
2.600 1.556 2.526
obligations rights respect
20 26 19
2.550 1.692 2.789 SP
Table 4 – Centrality test of the term Citizenship, RIDE-DF – 2012
tion of citizens in the public discussion of the communi-ty(4). Participation is anticipated in the Brazilian constitution through the institutional channels of social participation, among them, councils and conferences.
The historical conjuncture of the citizenship constitution took place during the formation of the national States, and the establishment of capitalism, due to the decline of feu-dalism and bourgeois rise. Therefore, citizenship developed as a principle of justice and with the normative function of organizing the political system and legitimizing political au-thority through citizens who hold rights and obligations(20).
In addition, social movements have played a key role in the consolidation of citizenship, because through strug-gles they overcame the development of social protection systems, aiming at reducing the deleterious effects of the capitalist system, based on the economic inequality of the social classes(20). Accordingly, social protection has devel-oped legally, in the form of rights guaranteeing the status of citizenship, and institutionalized in the systems of pro-vision of health, education and care goods and services, seeking to increase the population well-being(20).
Another category that emerged, called Full Citizen-ship, revealed that for citizenship to be complete it is nec-essary that the city be clean and organized, as a means of avoiding the spread of diseases, denoting a concern with the sanitary condition.
In this category it was understood that the councilors anchored their representations of citizenship in the reform-ist ideology that postulated the improvement of sanitary conditions as a pathway for access to the extension of the right to citizenship, more precisely to the democratization of society.(2)
CONCLUSIONS
The content of the social representations of the sub-jects of the study signaled that the right to health is un-derstood as a condition for reaching citizenship, and this as a form of social protection. These representations were shared by the group and possibly guided attitudes and behaviors within the councils, with a significant potential to influence the proposals and the decision making of the municipal health policies.
The structure of the social representations of citizen-ship was limited to the fulfillment of obligations, and the exercise of rights; however, the elements in the peripheral systems brought the conditions to have citizenship and the mechanisms of social protection, signaling a tenden-cy to amplify its meaning. It must be recognized that the process of changing social representations is a slow
move-ment, because first the peripheral elements of social repre-sentations are transformed, and then the central elements are modified.
Based on the SUS scenario, it was verified that the foun-dations of the health reform were built, but they require efforts to keep health as a public good, requiring a pro-found political change, which extends to an awareness of the right to health and citizenship. Therefore, to become a reality one must consider that modifying actions implies changing the representations that guide them.
Limitations of this study include the need for expand-ing the investigation on the influence of social representa-tions of right to health and citizenship of municipal coun-cilors on health policies, municipal health plans, and on the provision of community health services. In academic terms, the study may contribute to discussions and prompt new investigations about social representations in the field of health.
REFERENCES
1. Silva BK, Bezerra AFB, Tanaka OY. Direito à saúde e integralidade: uma discussão sobre os desafios e caminhos para a sua efetivação. Interface Comun Saúde Educ. 2012;16(40):249-59.
2. Paiva CHA, Teixeira LA. Reforma sanitária e a criação do Sistema Único de Saúde: notas sobre contextos e autores. Hist Cienc Saúde-Manguinhos. 2014;21(1):15-35.
3. Krüger TR, Lemke AP, Nardino D, Finger SJ, Meggiato JR, Nunes MLA. et al. As proposições das conferências de saúde e os planos municipais de saúde: um estudo em municípios de Santa Catarina. Saúde Debate. 2011;35(91):508-21. 4. Paiva FS, Van Stralen CJ, Costa PHA. Participação social e saúde no Brasil: revisão
sistemática sobre o tema. Cienc Saúde Coletiva. 2014;19(2):487-98. 5. Dallari SG. O direito à saúde. Rev Saúde Públ.1988;22(1):57-63.
6. Lara L, Guareschi NMF, Bernardes AG. Reforma sanitária e a privatização da saúde em um contexto biopolítico de garantia de direito. Psicol Soc. 2016;28(2):360-8. 7. Maia AAM, Pereira MZC. Cidadania, educação e cotidiano. Educ Real.
2014;39(2):617-31.
8. Moura LM. Capacidade das instâncias institucionalizadas de participação social em saúde da RIDE-DF: potencialidades e fragilidades para influenciar a melhoria da atenção básica [tese]. Brasília (DF): Universidade de Brasília, Programa de Pós-Graduação em Ciências da Saúde; 2015.
9. Moscovici S. Representações sociais: investigações em psicologia social. Petró-polis: Vozes; 2010.
10. Abric JC. A abordagem estrutural das representações sociais. In: Moreira ASP, Oliveira DC, organizadores. Estudos interdisciplinares de representação social. Goiânia: AB Editora; 1998. p. 27-38.
11. Pires MRGM, Göttems LBD, Martins CMF, Guilhem D, Alves ED. Oferta e demanda por média complexidade/SUS: relação com atenção básica. Cienc Saúde Cole-tiva. 2010;15(Supl. 1):1009-19.
df.gov.br/images/CODEPLAN/PDF/pesquisa_socioeconomica/PMAD/PMAD_ Perfil_socioeconomico_dos_moradores_dos_municipios_da_AMB.pdf. 13. Oliveira DC, Marques SC, Gomes AMT, Teixeira MATV. Análise das evocações
li-vres: uma técnica de análise estrutural das representações sociais. In: Moreira ASP, organizador. Perspectivas teórico-metodológicas em representações so-ciais. João Pessoa: EDUFPB; 2005. p. 573-602.
14. Bardin L. Análise de conteúdo. 1. ed. Lisboa: Edições 70; 2011.
15. Brysk A. Human rights and private wrongs: constructing global civil society. New York: Routledge; 2005.
16. United Nations Educational Scientific and Cultural Organization [Internet]. Paris: UNESCO, c2005- 2017 [cited 2014 Sep 1]. Universal Declaration on Bioethics and Human Rights; [about 12 screens]. Avaiable from: http://portal.unesco.org/ en/ev.php-URL_ID=31058&URL_DO=DO_TOPIC&URL_SECTION=201.html.
17. Mitano F, Ventura CAA, Lima MCRAA, Balegamire JB, Palha PF. Right to health: (in)congruence between the legal framework and the health system. Rev Lati-no-Am Enfermagem. 2016;24:e2679.
18. Kingston LN, Cohen EF, Morley CP. Debate: limitations on universality: the “right to health” and the necessity of legal nationality. BMC Int Health Hum Rights. 2010;10:11.
19. Andrade LOM, Pellegrini Filho A, Salar O, Rígoli F, Salazar LM, Serrate PCF, et al. Social determinants of health, universal health coverage and sustain-able development: case studies from Latin American Countries. Lancet. 2015;385(9975):1343-51.
20. Fleury S, Ouverney AM. Política de saúde: uma política social. In: Giovanella L, Escorel S, Lobato LVC, Noronha JC, Carvalho AI, organizadores. Políticas e sistema de saúde no Brasil. Rio de Janeiro: Editora Fiocruz; 2012. p. 23-64.
Corresponding author:
Luciana Melo de Moura
E-mail: [email protected]