DOI: 10.18410/jebmh/2015/646
ORIGINAL ARTICLE
J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 31/Aug. 03, 2015 Page 4597
A PROSPECTIVE STUDY OF CUTANEOUS ADVERSE DRUG REACTION
IN COASTAL DISTRICT OF ANDHRA PRADESH
J. Vijayashree1, Anand Acharya2
HOW TO CITE THIS ARTICLE:
J. Vijayashree, Anand Acharya.“A Prospective Study of Cutaneous Adverse Drug Reaction in Coastal District of Andhra Pradesh”. Journal of Evidence based Medicine and Healthcare; Volume 2, Issue 31, August 03, 2015; Page: 4597-4600, DOI: 10.18410/jebmh/2015/646
ABSTRACT: An adverse drug reaction can be defined as “an appreciably harmful or unpleasant reaction, resulting from an intervention related to the use of a medicinal product, which predicts hazard from future administration and warrants prevention or specific treatment, or alteration of the dosage regimen, or withdrawal of the product”. This is a prospective study conducted at two tertiary centers in coastal Andhra Pradesh during April 2013 to June 2015. Out of 164 cases of coetaneous ADR, 63% were male and 36.58%were female, Maculo popular rashes were most common cutaneous drug reaction. Out of all drugs antimicrobial agent were the most common drugs which is responsible for cutaneous ADR.
KEYWORDS: Cutaneous drug reaction, Coastal Andhra Pradesh.
INTRODUCTION: An adverse drug reaction can be defined as “an appreciably harmful or unpleasant reaction, resulting from an intervention related to the use of a medicinal product, which predicts hazard from future administration and warrants prevention or specific treatment, or alteration of the dosage regimen, or withdrawal of the product.(1)
The frequency and clinical patterns of cutaneous reactions are influenced by drug use, prevalence of specific conditions (e.g. HIV Infection) and pharmacogenetic traits of a population and that may vary greatly among the different population around the world.(2) Spectrum of
cutaneous reaction may vary from simple urticaria to Steven Johnson syndrome, Toxic epidermal hydrolysis and DRESS. Monitoring and reporting ADR is the important part of pharmacovigilance program of India (PPI) present study is designed. To examine various type of cutaneous drug reaction and its causative agent in coastal district of Andhra Pradesh.
MATERIAL AND METHODS: This is a prospective study conducted at two tertiary centers in coastal Andhra Pradesh during April 2013 to June 2015. All the suspected adverse drug reaction of all age groups and boat the sex where included in the study.
Information regarding adverse drug reaction was collected on suspected ADR reporting form of PVPI. Written informed consent was taken from each individual before enrollment in to the study. Diagnosis was made by proper history taking and medication document.
Exclusion documents criteria: 1. In appropriate mediation history.
2. Clinical diagnosis is not matching the drug reaction.
DOI: 10.18410/jebmh/2015/646
ORIGINAL ARTICLE
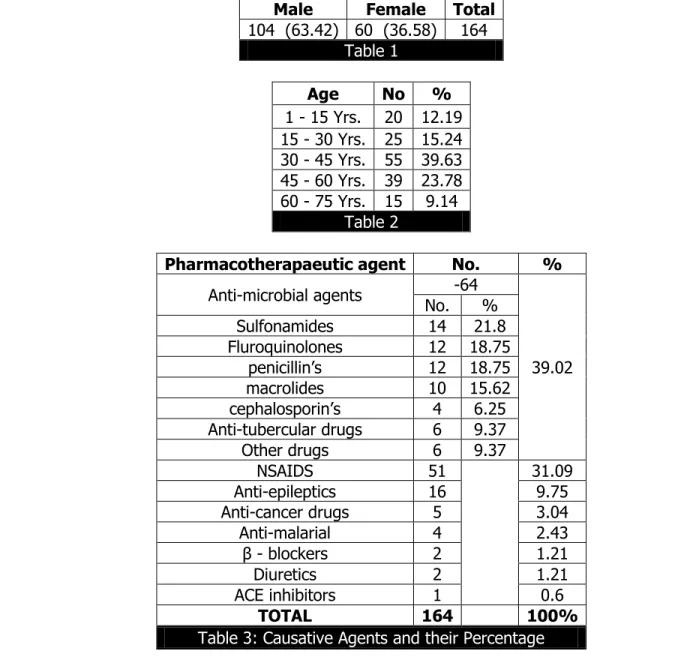
J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 31/Aug. 03, 2015 Page 4598 RESULT: During two year of study around 164 patients were enrolled for study, out of that 104 male and 60 female, between the age group 1yr. to 70yr., out of 164 pt. most of the pt. were in the age between 20 to 50yr.
Among all pharmacotherapecetic agent anti-microbial agents were most common drug which is responsible for cutaneous reaction, that is 39.02%, among then sulfonamide (21.8%) was most common followed by fluroquionolones (18.75%) penicillin, (18.75) and macrolides (15.62%).
NSAIDS accounted for 39.0%.
Anti-epileptic drugs accounted for 9.75%.
Maculo popular rashes are most common type of reaction which was 36.50%, cutaneous drug reaction that is 21.95%, fixed drug emption angioedema and erythema multiforme were 6.09% and 1.2% respectively. Stephen Johnson syndrome and TEN was rare that is 2.43% and 1.2% respectively.
Male Female Total 104 (63.42) 60 (36.58) 164
Table 1
Age No % 1 - 15 Yrs. 20 12.19 15 - 30 Yrs. 25 15.24 30 - 45 Yrs. 55 39.63 45 - 60 Yrs. 39 23.78 60 - 75 Yrs. 15 9.14
Table 2
Pharmacotherapaeutic agent No. %
Anti-microbial agents -64
39.02 No. %
Sulfonamides 14 21.8
Fluroquinolones 12 18.75
penicillin’s 12 18.75
macrolides 10 15.62
cephalosporin’s 4 6.25
Anti-tubercular drugs 6 9.37
Other drugs 6 9.37
NSAIDS 51 31.09
Anti-epileptics 16 9.75
Anti-cancer drugs 5 3.04
Anti-malarial 4 2.43
β - blockers 2 1.21
Diuretics 2 1.21
ACE inhibitors 1 0.6
TOTAL 164 100%
DOI: 10.18410/jebmh/2015/646
ORIGINAL ARTICLE
J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 31/Aug. 03, 2015 Page 4599
Maculopopular rashes 60 36.58%
Urticaria 36 21.95%
Fixed drug eruptions 34 20.73% Erythema multiforme 10 6.09%
Angioedema 2 1.20%
Stephen Johnsonsyndrome 4 2.43% Toxic epidermal necrolysis (TEN) 2 1.20%
Others 16 9.75%
TOTAL 164 100%
Table 4: Types of rashes and their Percentage
DISCUSSION: Out of 164 cases of coetaneous ADR, 63% were male and 36.58%were female, which is similar to the study of Sharma et al.(3) but B nit similar to the study of Faize.(4) out of all
drugs antimicrobial agent were the most common drugs which is responsible for cutaneous ADR, as reported earlier by Sarita.(5) Maculo popular rashes were most common cutaneous drug
reaction, which similar to the study.(6) Among the anti-microbial agent sulphonamide was the
most common drug which caused with ADR and next drug was NSAID, similar to other study.(7,8)
CONCLUSION: Cutaneous drug reaction can occur with many drugs and its severity varies from urticaria to SJS, TEN and DRESS. It is believed that medication error is 50 – 100 times common then ADES. So for prevention of ADR, best practices to be followed are to reduce the error.
BIBLIOGRAPHY:
1. Prof I Ralph Edwards, FRCP Jeffrey K Aronson, FRCP Adverse drug reactions: definitions, diagnosis, and management the lancet Volume 356, No. 9237, p1255–1259, 7 October 2000.
2. Naldi L, CrottiS. Epidemiology of cutaneous drug-induced reactions. G It al Dermatol Venereol. 2014 Apr; 149 (2):207-18.
3. Rohini Sharma, DevrajDogra, NainaDogra A study of cutaneous adverse drug reactions at a tertiary center in Jammu, India Year: 2015 | Volume: 6 | Issue: 3 | Page: 168-171.
4. Faiza Al-Raaie* and D.D. Banodkar Epidemiological Study of Cutaneous Adverse Drug
Reactions in Oman Med J. 2008 Jan; 23 (1): 21–27.
5. Sarita Sasidharanpillai, NajeebaRiyaz, Anza Khader, Uma Rajan, Manikoth P Binitha, and Deepthi N SureshanSevere Cutaneous Adverse Drug Reactions: A Clinicoepidemiological Study Indian J Dermatol. 2015 Jan-Feb; 60 (1): 102.
DOI: 10.18410/jebmh/2015/646
ORIGINAL ARTICLE
J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 31/Aug. 03, 2015 Page 4600
7. Amparo Hernandez-Salazar, Samuel Ponce de Leon-Rosales, Sigfrido Rangel-Frausto, EliaCriollo, Carla Archer-Dubon, Epidemiology of Adverse Cutaneous Drug Reactions. A Prospective Study in Hospitalized Patients.
8. Tejas K Patel, Sejal H Thakkar, DC Sharma. Cutaneous adverse drug reactions in Indian population: A systematic review. Indian dermatology online journal Year: 2014;5(6):76-86. 9. Bates Dw, Boyle DL, Vander Bliet MB, et al. relationship between medication errors and
adverse drug event j. Gen inter med 1995 to 199-205.
NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR:
Dr. Anand Acharya, Professor,
Department of Pharmacology, KIMS, Amalapuram.
E-mail: [email protected]
Date of Submission: 27/07/2015. Date of Peer Review: 28/07/2015. Date of Acceptance: 30/07/2015. Date of Publishing: 31/07/2015.
AUTHORS:
1. J. Vijayashree 2. Anand Acharya
PARTICULARS OF CONTRIBUTORS:
1. Associate Professor, Department of DVL, Great Eastern Medical School and Hospital, Srikakulam.