https://doi.org/10.1007/s00592-017-1090-y ORIGINAL ARTICLE
Maternal educational level and the risk of persistent post‑partum
glucose metabolism disorders in women with gestational diabetes
mellitus
Inês Gante1 · Ana Carina Ferreira2 · Gonçalo Pestana3 · Daniela Pires4,5 · Njila Amaral6 · Jorge Dores7 · Maria do Céu Almeida1 · José Luis Sandoval8
Received: 20 August 2017 / Accepted: 11 December 2017 / Published online: 29 December 2017 © Springer-Verlag Italia S.r.l., part of Springer Nature 2017
Abstract
Aims Gestational diabetes mellitus (GDM) occurs in 5–15% of pregnancies, and lower maternal educational attainment has been associated with higher risk of GDM. We aimed to determine if maternal education level is associated with persistent post-partum glucose metabolism disorders in women with GDM.
Methods Retrospective cohort study of women with GDM followed in 25 Portuguese health institutions between 2008 and 2012. Educational attainment was categorised into four levels. Prevalence of post-partum glucose metabolism disorders (type 2 diabetes mellitus, increased fasting plasma glucose or impaired glucose tolerance) was compared and adjusted odds ratios calculated controlling for confounders using logistic regression.
Results We included 4490 women diagnosed with GDM. Educational level ranged as follows: 6.8% (n = 307) were at level 1 (≤ 6th grade), 34.6% (n = 1554) at level 2 (6–9th grade), 30.4% (n = 1364) at level 3 (10–12th grade) and 28.2% (n = 1265) at level 4 (≥ university degree). At 6 weeks post-partum re-evaluation, 10.9% (n = 491) had persistent glucose metabolism disorders. Educational levels 1 and 2 had a higher probability of persistent post-partum glucose metabolism disorders when compared to level 4 (OR = 2.37 [1.69;3.32], p < 0.001 and OR = 1.39 [1.09;1.76], p = 0.008, for level 1 and 2, respectively), an association that persisted in multivariable logistic regression adjusting for confounders (level 1 OR = 2.25 [1.53;3.33],
p < 0.001; level 2 OR = 1.43 [1.09;1.89], p = 0.01).
Conclusions Persistent post-partum glucose metabolism disorders are frequent in women with GDM and associated with lower maternal educational level. Interventions aimed at this risk group may contribute towards a decrease in prevalence of post-partum glucose metabolism disorders.
Keywords Diabetes · Gestational · Education · Women · Post-partum
Introduction
Gestational diabetes mellitus (GDM), defined as decreased glucose tolerance diagnosed during pregnancy, is estimated to occur in 5–15% of pregnancies [1, 2]. Insulin resistance, caused partly by placental hormones and maternal adiposity, is recognised as the most important aetiological factor [3].
GDM was associated with adverse foetal, labour and maternal outcomes [2, 4–6]. As for maternal complications, a higher rate of hypertensive disorders (gestational hyperten-sion, preeclampsia and eclampsia) [7] and increased risk of developing glucose metabolism disorders after pregnancy such as type 2 diabetes mellitus (type 2 DM), impaired fasting glucose or impaired glucose tolerance have been described [8]. GDM increases the risk of developing type Managed by Massimo Federici.
Electronic supplementary material The online version of this article (http s://doi.org/10.1007 /s005 92-017-1090 -y) contains supplementary material, which is available to authorized users. * Inês Gante
[email protected] * José Luis Sandoval [email protected]
2 DM up to seven times. Therefore, screening for type 2 DM and other glucose metabolism disorders at 6–12 weeks after delivery is mandatory according to current guidelines [9]. Moreover, studies have shown that all types of glucose metabolism disorders are associated with increased risk of cardiovascular disease, which is higher in participants meet-ing the criteria for type 2 DM [10, 11].
Identified risk factors for GDM include Asian and black ethnicity, increased maternal age, obesity, polycystic ovary syndrome, personal history of GDM and family history of diabetes [2]. Known predictive factors for persisting glucose metabolism disorders after pregnancy are obesity, GDM diagnosed before the 24th week of gestation and require-ment of insulin treatrequire-ment to achieve glycemic control during pregnancy [8, 12].
Maternal education is an additional risk factor for glu-cose metabolism disorders in the general population [13] as well as for GDM, as recently shown by Bouthoorn et al. [14]. However, its role as a predictive factor for persistence of glucose metabolism disorders after a pregnancy with a GDM diagnosis has not, to the best of our knowledge, been explored.
The aim of this study was to determine if maternal educa-tional level was associated with increased risk of persisting post-partum glucose metabolism disorders in women with GDM.
Methods
We performed a retrospective cohort study of pregnant women diagnosed with GDM, who delivered in Portugal between 2008 and 2012.
Study population
Data were obtained from the Portuguese National Registry of GDM with permission from the database coordinator— the Study Group of the Portuguese Society of Diabetology (SGPSD).
GDM diagnosis was established using the criteria recom-mended by the Portuguese Directorate-General of Health (PDGH). Until February 2011, diagnosis was based on the Carpenter and Coustan’s criteria, with a 100-g 3-h oral glucose tolerance test (OGTT), after a selective screening strategy in the 1st trimester and between 24 and 28 ges-tational weeks [15]. After February 2011, diagnosis was established using a universal screening strategy based on the International Association of Diabetes and Pregnancy Study Groups’ criteria, American Diabetes Association (ADA) and the World Health Organisation—fasting plasma glucose in the 1st trimester and 75-g 2-h OGTT between 24 and 28 gestational weeks [1, 16, 17]. To determine if
different diagnostic criteria could be an effect modifier of the relationship between maternal education and the outcome, an interaction term between maternal education and diag-nostic criteria was added to the logistic regression analysis (see below). This was not significant (p = 0.33), and, con-sequently, we present our results without stratification by this variable.
Women with history of diabetes and those with twin preg-nancies were not included in the database.
Data were collected from clinical records of women with GDM followed in 25 Portuguese public sector health institutions, from a total of 44 institutions invited to partici-pate in the study and comprising all Portuguese continen-tal districts. Datasets were aggregated and validated by the SGPSD, according to the data provided by the PDGH. Data were blinded with respect to patient and health institution’s identification, ensuring anonymity of the collected data. This study complies with the Declaration of Helsinki on medi-cal protocol and ethics. Each participating hospital’s insti-tutional review board approved data collection. Given the retrospective nature of this study and the use of anonymised data, participants’ written consent was not required. Outcome variable
The primary outcome was defined by the presence or absence of any glucose metabolism disorder at 6 weeks post-partum [9], defined as a composite of either type 2 DM or increased fasting plasma glucose or impaired glucose toler-ance in a 2-h 75-g OGTT. Type 2 DM was diagnosed in the presence of a plasma glucose ≥ 7 mmol/L after a 8 h fast or a 2 h plasma glucose ≥ 11 mmol/L during an OGTT; increased fasting plasma glucose as fasting plasma glucose of 5.5–6.9 mmol/L and impaired glucose tolerance as plasma glucose 7.7–10.9 mmol/L 2 h after an OGTT [9, 12, 15]. No differences in how the outcome was measured were expected to have occurred between the groups defined by maternal educational level.
Covariates
The predictor variable, maternal educational level, was divided into four categories: level 1 (6th grade or less), level 2 (from 6th to 9th grade), level 3 (from 10th to 12th grade) and level 4 (university degree or higher).
Potential confounders were included as covariates in the statistical analysis. These include demographic (maternal age and district) and biometric characteristics (pre-pregnancy body mass index (BMI)—categorised into normal < 25 kg/m2, overweight ≥ 25 and < 30 kg/
m2 and obese ≥ 30 kg/m2; and gestational weight gain—
classified as a weight increase below, within or above the limits established by the 2009 Institute of Medicine
recommendations [18]) and obstetric history (nulliparous, previous pregnancy with or without GDM).
Women received education on diet, exercise and appro-priate glycemic targets. According to the guidelines of the Portuguese General-Directorate of Health [19], the goal of therapy was to reduce fasting glucose to 3.3–5.0 mmol/L and the 1 h postprandial level to 5.5–6.6 mmol/L in more than 90% of the glucose measurements. Insulin was started if the glycemic targets were not achieved within 1–2 weeks with non-pharmacological therapy. Gestational age at GDM diagnosis (determined using obstetric ultrasound), the delay between diagnosis and first GDM obstetric appointment and the need of insulin therapy were also included in the analysis.
The mean value of HbA1c in the third trimester was obtained, but not included in the multivariable model, as it would not be a predictor but a consequence of glucose metabolism disorders.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) and categorical variables as number and frequency.
In order to identify an association between educational level and the persistence of glucose metabolism disor-ders after delivery, we performed a univariable logistic regression analysis with glucose metabolism disorders as the outcome and educational level as a predictor. Multi-variable logistic regression analysis was used to adjust for confounding variables (age, district, pre-pregnancy BMI, gestational weight gain, obstetric history, week of diagno-sis, delay to specialist appointment and insulin-requiring GDM).
To assess if an effect modification of educational level on the outcome could be observed for maternal age, year of diagnosis, geographical location or number of previous deliveries (using only multiparous women), we performed a logistic regression including interaction terms for each of the variables individually. For this analysis, educational level was dichotomised into two groups: levels 1–2 and 3–4. Due to chance alone, we would expect 0.20 of the four interaction tests to be statistically significant at the
p < 0.05 level.
The need for insulin therapy during pregnancy was used as a surrogate for lack of glycemic control. We performed logistic regression using this variable as an outcome and educational level and the previously mentioned confound-ers as predictors.
All data were analysed using STATA 13.1 and R 3.2.2. A two-sided p < 0.05 was considered significant and 95% confidence intervals are presented.
Missing data
Missing data for the explanatory variable (educational level) were assumed to be missing completely at random, and par-ticipants with missing data for this variable were excluded from the analysis. We assumed missing values for the out-come (persistent post-partum glucose metabolism disorders) were missing at random (MAR). By MAR we mean that the missingness of the outcome may be determined by other variables, such as education, with previous studies having reported that more educated women have a higher probabil-ity of returning for the re-evaluation appointment 6 weeks after delivery than least educated ones [20–22]. To address this limitation, multiple imputation was performed for the outcome variable. We used the mi package of STATA to create 40 imputed datasets using chained equations which were then combined and analysed. All potential confound-ers used in the multivariable logistic models were included in the imputation model. Results from imputed data did not differ from the ones obtained by complete case analysis, what is consistent with previous reports on outcome impu-tation [23]. As such, complete case analysis (only including participants with data for the outcome) was reported. The descriptives of participants with missing data can be found in Table S1, and we could observe that those with missing data for maternal education did not considerably differ from those included in the complete case analysis.
Results
The cohort used in this study comprises 4490 women diag-nosed with gestational diabetes mellitus. The original dataset was composed of 8266 women. Women with missing data for the outcome (n = 2944) and/or the predictor (n = 1636) were excluded from the analysis (n = 3776).
Mean age ± SD of participants was 33.2 ± 5.1 years. While 44.2% (n = 1923) had a normal pre-pregnancy BMI, 30.5% (n = 1329) were overweight, and 25.3% (n = 1100) were obese. Concerning educational level, 6.8% (n = 307) of the participants belonged to level 1, 34.6% (n = 1554) to level 2, 30.4% (n = 1364) to level 3 and 28.2% (n = 1265) to level 4. Baseline characteristics of the participants stratified by educational level are shown in Table 1.
The mean ± SD for the week of GDM diagnosis was 26.0 ± 7.9 and 2.8 ± 3.5 weeks for the delay between diag-nosis and first GDM obstetric appointment.
A total of 11.9% (n = 532) of the women had a previous pregnancy with a diagnosis of GDM, 41.1% (n = 1835) had a pregnancy without this diagnosis, and 46.9% (n = 2093) were nulliparous. The mean ± SD for third trimester HbA1c measurement was 5.3 ± 0.5% (34 ± 6 mmol/mol). Twenty-seven per cent (n = 1142) experienced an excessive weight
gain according to the IOM guidelines and 34.8% (n = 1561) needed insulin therapy during pregnancy.
At the 6 weeks post-partum re-evaluation, 10.9% (n = 491) were diagnosed with persistent glucose metabo-lism disorders. Impaired glucose tolerance was the most prevalent type of glucose metabolism disorder, occurring in 8.0% (n = 357). Post-partum diabetes and impaired fasting glucose were present in 1.6% (n = 73) and 1.4% (n = 61), respectively.
When stratified by educational level, significant differ-ences were observed between groups. Notably, less edu-cated women were older (36.1 ± 4.7 level 1 vs. 33.8 ± 4.2 level 4), had a higher pre-pregnancy BMI (30.6% level 1
vs. 54.2% level 4, had normal pre-pregnancy BMI), were more frequently multiparous (23.3% were nulliparous in level 1 vs. 61.6% in level 4) and had a higher percentage of excessive weight gain during pregnancy (29.6% level 1 vs. 22.9% level 4). Moreover, less educated women had a higher percentage of post-partum glucose metabolism disorders (19.9% level 1 vs. 9.5% level 4) and higher need of insulin to achieve glycemic control during pregnancy (41.0% level 1 vs. 30.3% level 4). The remaining baseline clinical, laboratory and demographic data, as well as miss-ing data details, can be found summarised in Table 1 and Table S2.
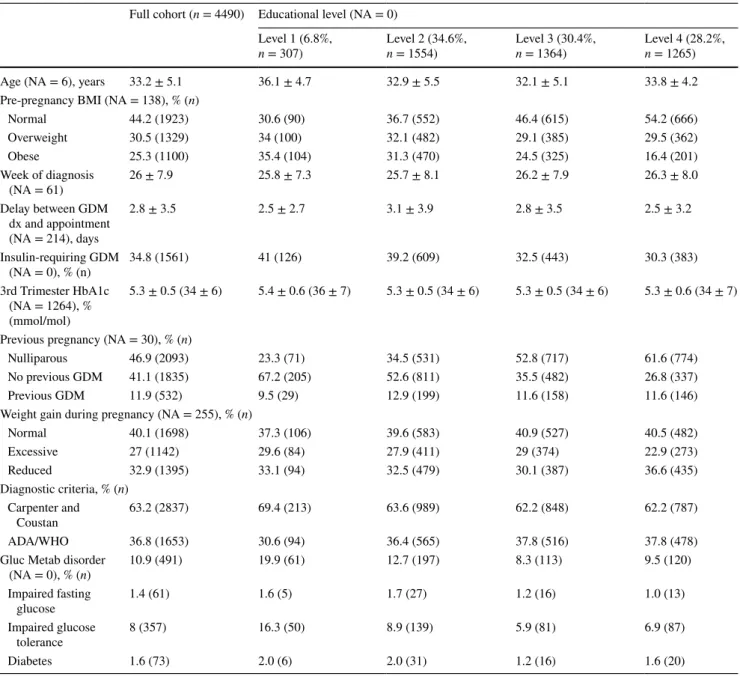
Table 1 Baseline characteristics of participants, overall and according to their educational level
NA indicates missing data. Data are mean ± SD, unless otherwise specified Full cohort (n = 4490) Educational level (NA = 0)
Level 1 (6.8%,
n = 307) Level 2 (34.6%, n = 1554) Level 3 (30.4%, n = 1364) Level 4 (28.2%, n = 1265)
Age (NA = 6), years 33.2 ± 5.1 36.1 ± 4.7 32.9 ± 5.5 32.1 ± 5.1 33.8 ± 4.2
Pre-pregnancy BMI (NA = 138), % (n)
Normal 44.2 (1923) 30.6 (90) 36.7 (552) 46.4 (615) 54.2 (666) Overweight 30.5 (1329) 34 (100) 32.1 (482) 29.1 (385) 29.5 (362) Obese 25.3 (1100) 35.4 (104) 31.3 (470) 24.5 (325) 16.4 (201) Week of diagnosis (NA = 61) 26 ± 7.9 25.8 ± 7.3 25.7 ± 8.1 26.2 ± 7.9 26.3 ± 8.0 Delay between GDM dx and appointment (NA = 214), days 2.8 ± 3.5 2.5 ± 2.7 3.1 ± 3.9 2.8 ± 3.5 2.5 ± 3.2 Insulin-requiring GDM (NA = 0), % (n) 34.8 (1561) 41 (126) 39.2 (609) 32.5 (443) 30.3 (383) 3rd Trimester HbA1c (NA = 1264), % (mmol/mol) 5.3 ± 0.5 (34 ± 6) 5.4 ± 0.6 (36 ± 7) 5.3 ± 0.5 (34 ± 6) 5.3 ± 0.5 (34 ± 6) 5.3 ± 0.6 (34 ± 7) Previous pregnancy (NA = 30), % (n)
Nulliparous 46.9 (2093) 23.3 (71) 34.5 (531) 52.8 (717) 61.6 (774)
No previous GDM 41.1 (1835) 67.2 (205) 52.6 (811) 35.5 (482) 26.8 (337)
Previous GDM 11.9 (532) 9.5 (29) 12.9 (199) 11.6 (158) 11.6 (146)
Weight gain during pregnancy (NA = 255), % (n)
Normal 40.1 (1698) 37.3 (106) 39.6 (583) 40.9 (527) 40.5 (482) Excessive 27 (1142) 29.6 (84) 27.9 (411) 29 (374) 22.9 (273) Reduced 32.9 (1395) 33.1 (94) 32.5 (479) 30.1 (387) 36.6 (435) Diagnostic criteria, % (n) Carpenter and Coustan 63.2 (2837) 69.4 (213) 63.6 (989) 62.2 (848) 62.2 (787) ADA/WHO 36.8 (1653) 30.6 (94) 36.4 (565) 37.8 (516) 37.8 (478)
Gluc Metab disorder
(NA = 0), % (n) 10.9 (491) 19.9 (61) 12.7 (197) 8.3 (113) 9.5 (120) Impaired fasting glucose 1.4 (61) 1.6 (5) 1.7 (27) 1.2 (16) 1.0 (13) Impaired glucose tolerance 8 (357) 16.3 (50) 8.9 (139) 5.9 (81) 6.9 (87) Diabetes 1.6 (73) 2.0 (6) 2.0 (31) 1.2 (16) 1.6 (20)
Lower educational level correlates with a higher probability of persistent post‑partum glucose metabolism disorders
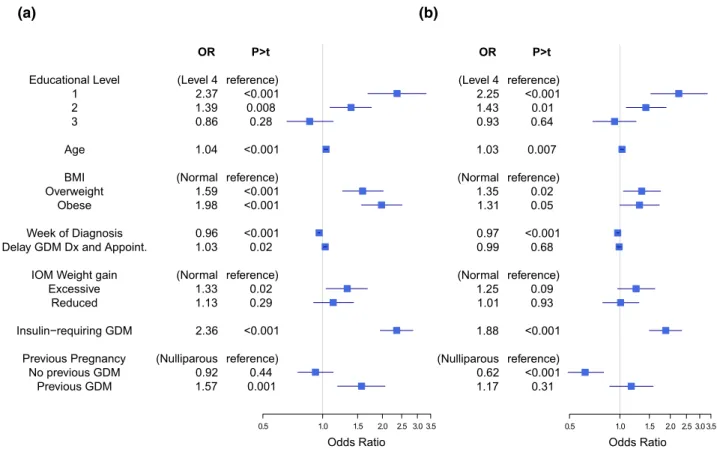
We performed a univariable analysis (Fig. 1a) to correlate educational levels (as well as other predictors, namely age, pre-pregnancy BMI, week of diagnosis, delay between diagnosis and specialist appointment, weight gain, insulin-requiring GDM and previous pregnancy information) with post-partum glucose metabolism disorders. Educational lev-els 1 and 2 had a statistically significant higher probability of having persistent post-partum glucose metabolism disorders when compared to level 4 (OR = 2.37 [1.69;3.32], p < 0.001 and OR = 1.39 [1.09;1.76], p = 0.008, for level 1 and 2, respectively). Noticeably, insulin-requiring participants or those with a previous diagnosis of GDM also had a signifi-cantly higher probability of persistent post-partum glucose metabolism disorders in this univariable analysis (OR = 2.36 [1.95;2.85], p < 0.001 and OR = 1.57 [1.19;2.06], p = 0.001, respectively).
After adjustment for the previously described confound-ers using multivariable logistic regression (Fig. 1b), lower educational levels 1 and 2 were associated with a signifi-cantly higher probability of persistent post-partum glucose
metabolism disorders (level 1 OR = 2.25 [1.53;3.33],
p < 0.001; level 2 OR = 1.43 [1.09;1.89], p = 0.01). In
addition, participants requiring insulin to achieve glycemic control were also associated with this outcome (OR = 1.88 [1.50;2.34], p < 0.001). Significance could also be observed for age (OR = 1.03 [1.01;1.05], p = 0.007), week of diagno-sis (OR = 0.97 [0.96;0.99], p < 0.001) and overweight par-ticipants (OR = 1.35 [1.05;1.75], p = 0.02). Previous preg-nancy with GDM was not predictive of the outcome when compared to nulliparous women (OR = 1.17 [0.87;1.58],
p = 0.31). However, having a pregnancy without
previ-ous diagnosis of GDM was related to a lower probability of persistent post-partum glucose metabolism disorders (OR = 0.62 [0.49;0.80], p < 0.001).
Maternal age modifies the effect of educational level on persistent post‑partum glucose metabolism disorders
While no effect modification could be observed by district of origin, year of diagnosis or number of previous deliveries (in multiparous women) (Fig. S2a, Fig. S2b and Table S3), a significant interaction was detected for maternal age (coeffi-cient = − 0.04 [− 0.08;− 0.01], p = 0.02). The probability of
Educational Level 1 2 3 Age BMI Overweight Obese Week of Diagnosis Delay GDM Dx and Appoint.
IOM Weight gain Excessive Reduced Insulin−requiring GDM Previous Pregnancy No previous GDM Previous GDM OR (Level 4 2.37 1.39 0.86 1.04 (Normal 1.59 1.98 0.96 1.03 (Normal 1.33 1.13 2.36 (Nulliparous 0.92 1.57 P>t reference) <0.001 0.008 0.28 <0.001 reference) <0.001 <0.001 <0.001 0.02 reference) 0.02 0.29 <0.001 reference) 0.44 0.001 0.5 1.0 1.5 2.0 2.5 3.0 3.5 Odds Ratio (b) (a) OR (Level 4 2.25 1.43 0.93 1.03 (Normal 1.35 1.31 0.97 0.99 (Normal 1.25 1.01 1.88 (Nulliparous 0.62 1.17 P>t reference) <0.001 0.01 0.64 0.007 reference) 0.02 0.05 <0.001 0.68 reference) 0.09 0.93 <0.001 reference) <0.001 0.31 0.5 1.0 1.5 2.0 2.5 3.03.5 Odds Ratio
Fig. 1 Forest plots for a univariable and b multivariable logistic regression (n = 3978) indicating the association, effect size and direc-tion between confounder variables and educadirec-tional level and higher
probability of persistent post-partum glucose metabolism disorders. Odds ratios (OR) with 95% confidence intervals. Age in years, delay between GDM diagnosis (dx) and appointment in days
having persistent post-partum glucose metabolism disorders increased with age to a lower degree in educational levels 1–2 than in levels 3–4 (Fig. 2a). Moreover, the difference between the groups was only significant before the maternal age of 37 years, encompassing the majority of the partici-pants (Fig. 2b).
Educational level influences glycemic control resulting in higher probability of requiring insulin during pregnancy
Participants with educational levels 1 and 2 had a higher probability of needing insulin during pregnancy (OR = 1.39 [1.03;1.87], p = 0.03 and OR = 1.39 [1.16;1.68], p = 0.001 for level 1 and 2, respectively, and when compared to level 4) (Fig. 3). It is also worth noticing that excessive weight gain (OR = 1.21 [1.01;1.45], p = 0.04), previous pregnancy with GDM (OR = 1.48 [1.18;1.85], p = 0.001 compared to nul-liparous), age (OR = 1.02 [1.01;1.04], p = 0.006) and higher pre-pregnancy BMI (OR = 1.53 [1.29;1.82], p < 0.001 for overweight and OR = 2.20 [1.84;2.63], p < 0.001 for obese participants) were also associated with increased probability of insulin-requiring GDM. 0 .1 .2 .3 .4 Pr(GlucMetD) 10 20 30 40 50 Maternal Age 0 .02 .04 .06 .08 Density 10 20 30 40 50 Maternal Age
1-2Educational Level3-4 All (a)
(b)
Fig. 2 a Margins plot with 95% confidence intervals for effect
modi-fication by age of the educational level influence on the probability of persistent post-partum glucose metabolism disorders, b density plot for maternal age. Maternal age in years. Predicted probability of glu-cose metabolism disorders [Pr(GlucMetD)]
Fig. 3 Forest plot for multi-variable logistic regression indicating the association, effect size and direction between confounder variables and educational level and higher probability of insulin-requiring GDM pregnancy. Odds ratios (OR) with 95% confidence intervals. Age in years, delay between GDM diagnosis (dx) and appointment in days
Educational Level 1 2 3 Age BMI Overweight Obese Week of Diagnosis Delay GDM Dx and Appoint.
IOM Weight gain Excessive Reduced Previous Pregnancy No previous GDM Previous GDM OR (Level 4 1.39 1.39 1.14 1.02 (Normal 1.53 2.20 0.91 0.94 (Normal 1.21 0.93 (Nulliparous 1.01 1.48 P>t reference) 0.03 0.001 0.18 0.006 reference) <0.001 <0.001 <0.001 <0.001 reference) 0.04 0.38 reference) 0.89 0.001 0.5 1.0 1.5 2.0 2.5 3.0 Odds Ratio Multivariable logistic regression (n=3978)
Discussion
We characterised a cohort of women with GDM, followed in more than half of all public sector health institutions in Portugal between the years 2008 and 2012, and we observed that persistent glucose metabolism disorders at 6 weeks post-partum are frequent (10.9%) and asso-ciated with lower educational levels. While Bouthoorn et al. showed an association between this socio-economic indicator and GDM risk [14], an unequal persistence of post-partum glucose metabolism disorders in women with GDM has not, to the best of our knowledge, been previ-ously described in such a large cohort and has potential public health implications.
We must acknowledge the limitations of our study. First, the observational nature of a cohort study design prevents us from inferring causality and the retrospective analysis, despite the large dataset, limits the study’s con-clusions. Second, different and evolving diagnostic criteria for GDM, as well as pre-diabetes stages are a concern, although a difficult one to overcome as they lack a uni-versal definition. Third, the absence of baseline glycemic measures does not allow us to determine if lower educated women already had undiagnosed glucose metabolism dis-orders, other than type 2 DM, before pregnancy. Fourth, only 25 of the 44 public sector healthcare institutions man-aging gestational diabetes mellitus agreed to participate in this study, what may limit the generalisability of the study results. Fifth, missing data for outcome and explanatory variables were high, with missing data for the outcome (36.5%) being in line with previous reports of non-adher-ence to gestational diabetes mellitus post-partum screen-ing [20, 22]. While we tried to address missing data by describing it and using multiple imputation, it is possible that our assumptions concerning their nature might not be accurate. Finally, during the years included in our study insulin was the mainstay of pharmacological treatment of GDM, as it preceded the widespread acceptance and gen-eralisation of the use of metformin during pregnancy. It would be of interest to assess if our findings persist after the implementation of this new approach.
The results from our cohort agree with what has been described for this patient population [24–26]: older age, higher pre-pregnancy BMI, earlier week of diagnosis and requirement for pharmacological treatment were asso-ciated with persistent glucose metabolism disorders. Inversely, a previous pregnancy without GDM was asso-ciated with normal post-partum glucose metabolism.
The association between lower educational level and glucose metabolism disorders at 6 weeks post-partum was consistent throughout the years encompassed in this study and across different geographical areas. Lower educated
women were older, had higher pre-pregnancy BMI at the first pregnancy visit, gained more weight during pregnancy and had a higher probability of insulin-requiring GDM during pregnancy compared to other educational strata. The association we identified could be partly due to these confounding factors, widely known to be potential causes for both type 2 DM and GDM. However, the fact that the association between educational level and the outcome was independent of said confounders suggests that other mechanisms concur towards this deleterious outcome. Lower educational levels may be associated with specific lifestyle habits, mainly lack of exercise and/or unhealthy diet, which are important risks factors for type 2 DM and not measured in our cohort. It is plausible that women with lower educational level may be exposed to other socio-economic factors, such as worse employment conditions, less free time to perform leisure activities and physical exercise.
Other potential unmeasured confounders could influence this association. A possible contributing factor could be worse glycemic control during pregnancy, but the lack of association between third trimester HbA1c and educational level seems to contradict this hypothesis (data available in Table S4). However, the role of HbA1c as a marker of glycemic control during pregnancy has recently been chal-lenged, as physiological changes (such as anaemia) and the short duration of altered glycemic control during pregnancy might preclude the use of this marker [27]. We also showed that lower maternal educational level was related to higher probability of insulin-requiring GDM, suggesting worse gly-cemic control in low educated participants that could result in the observed persistent post-partum glucose metabolism disorders. Nevertheless, the inclusion of this variable in the logistic regression model did not remove the significance of educational level in predicting the outcome, suggesting that worse glycemic control was not sufficient to explain the observed effect.
Type 2 DM increasing prevalence is a major concern, making it a key target for public health interventions [28]. Impaired fasting glucose and impaired glucose tolerance are known to be pre-diabetic conditions associated with a higher risk of developing type 2 DM later in life [11, 29]. As such, it is important to know which women with GDM are at the highest risk for persistent glucose metabolism disorders. This group could benefit from targeted interventions aimed at preventing persistent glucose metabolism disorders and/or effectively reducing the risk of progression to overt diabetes, as underscored in the 2015 ADA Diabetes Guidelines [30].
In conclusion, we believe information originating from this large cohort is valuable in both adding to current knowl-edge and suggesting future research paths. While this study was performed using a Portuguese population, educational level heterogeneity occurs universally and understanding
how widespread the association with persistent post-partum glucose metabolism disorders actually is, would be of great importance. Future studies may enable the development of targeted public health interventions focused on reducing the observed inequities in post-partum glucose metabolism disorders in this population and, consequently, contrib-ute to a reduction in the global burden of diabetes and its complications.
Acknowledgements We thank the multidisciplinary teams of obste-tricians and diabetologists of Portuguese health institutions who col-lected patient data for the National Registry of Gestational Diabetes. In addition, we would like to acknowledge the alumni and faculty of the Harvard Medical School—Portugal Clinical Scholars Research Train-ing Programme for useful scientific discussions. DP was partially sup-ported by Fundação para a Ciência e Tecnologia under the Program for doctoral training in clinical research for medical interns (SFRH/ SINT/95317/2013).
Funding This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Compliance with ethical standards
Conflict of interest All authors declare that they have no conflict of interest.
Ethical approval All procedures in this study were in accordance with the ethical standards of the institutional and national research commit-tee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent For this type of study using retrospective and anonymised data, participants’ written consent was not required.
References
1. Kampmann U, Madsen LR, Skajaa GO, Iversen DS, Moeller N, Ovesen P (2015) Gestational diabetes: a clinical update. World J Diabetes 6(8):1065–1072. http s://doi.org/10.4239 /wjd.v6.i8.1065
2. Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR et al (2008) Hyperglycemia and adverse preg-nancy outcomes. N Engl J Med 358(19):1991–2002. http s://doi. org/10.1056 /NEJM oa07 0794 3
3. Di Cianni G, Miccoli R, Volpe L, Lencioni C, Del Prato S (2003) Intermediate metabolism in normal pregnancy and in gestational diabetes. Diabetes Metab Res Rev 19(4):259–270. http s://doi. org/10.1002 /dmrr .390
4. Gorgal R, Goncalves E, Barros M, Namora G, Magalhaes A, Rodrigues T et al (2012) Gestational diabetes mellitus: a risk factor for non-elective cesarean section. J Obstet Gynaecol Res 38(1):154–159. http s://doi.org/10.1111 /j.1447 -0756 .2011 .0165 9.x
5. Mitanchez D, Yzydorczyk C, Simeoni U (2015) What neona-tal complications should the pediatrician be aware of in case of maternal gestational diabetes? World J Diabetes 6(5):734–743.
http s://doi.org/10.4239 /wjd.v6.i5.734
6. Simeoni U, Barker DJ (2009) Offspring of diabetic pregnancy: long-term outcomes. Semin Fetal Neonatal Med 14(2):119–124.
http s://doi.org/10.1016 /j.siny .2009 .01.002
7. Yogev C, Hod C, Oats M et al (2010) Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: preeclampsia. Am J Obstet Gynecol 202(3):255 e1–255 e7. http s://doi.org/10.1016 / j.ajog .2010 .01.024
8. Kim C, Newton KM, Knopp RH (2002) Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 25(10):1862–1868
9. Expert Committee on the Diagnosis and Classification of Dia-betes Mellitus (2003) Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 26(Suppl 1):S5–S20. http s://doi.org/10.2337 /diac are.26.2007 . S5
10. Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV et al (1999) Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation 100(10):1134–1146
11. Nathan DM, Davidson MB, DeFronzo RA, Heine RJ, Henry RR, Pratley R et al (2007) Impaired fasting glucose and impaired glu-cose tolerance: implications for care. Diabetes Care 30(3):753– 759. http s://doi.org/10.2337 /dc07 -9920
12. Lee AJ, Hiscock RJ, Wein P, Walker SP, Permezel M (2007) Gestational diabetes mellitus: clinical predictors and long-term risk of developing type 2 diabetes: a retrospective cohort study using survival analysis. Diabetes Care 30(4):878–883. http s://doi. org/10.2337 /dc06 -1816
13. Magliano DJ, Barr EL, Zimmet PZ, Cameron AJ, Dunstan DW, Colagiuri S et al (2008) Glucose indices, health behaviors, and incidence of diabetes in Australia: the Australian Diabetes, Obe-sity and Lifestyle Study. Diabetes Care 31(2):267–272. http s://doi. org/10.2337 /dc07 -0912
14. Bouthoorn SH, Silva LM, Murray SE, Steegers EA, Jaddoe VW, Moll H et al (2015) Low-educated women have an increased risk of gestational diabetes mellitus: the Generation R Study. Acta Dia-betol 52(3):445–452. http s://doi.org/10.1007 /s005 92-014-0668 -x
15. Carpenter MW, Coustan DR (1982) Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol 144(7):768–773 16. World Health Organization (2014) Diagnostic criteria and
classification of hyperglycaemia first detected in pregnancy: a World Health Organization Guideline. Diabetes Res Clin Pract 103(3):341–363. http s://doi.org/10.1016 /j.diab res.2013 .10.012
17. Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P et al (2010) International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33(3):676–682. http s://doi.org/10.2337 /dc09 -1848
18. Rasmussen KM, Yaktine AL (eds) (2009) Weight gain during pregnancy—reexamining the guidelines. Washington (DC): National Academies Press (US)
19. Dores JM, Magalhães A, Carvalheiro M (2017) Relatório de Con-senso sobre a Diabetes e Gravidez. Portuguese General-Directo-rate of Health. 2011. http ://www.saud erep rodu tiva .dgs.pt/fich eiro s-de-uplo ad-dive rsos /rela tori o-de-cons enso -pdf.aspx
20. Ferrara A, Peng T, Kim C (2009) Trends in postpartum diabetes screening and subsequent diabetes and impaired fasting glucose among women with histories of gestational diabetes mellitus: a report from the Translating Research Into Action for Diabe-tes (TRIAD) Study. DiabeDiabe-tes Care 32(2):269–274. http s://doi. org/10.2337 /dc08 -1184
21. Bennett WL, Ennen CS, Carrese JA, Hill-Briggs F, Levine DM, Nicholson WK et al (2011) Barriers to and facilitators of post-partum follow-up care in women with recent gestational diabe-tes mellitus: a qualitative study. J Womens Health (Larchmt) 20(2):239–245. http s://doi.org/10.1089 /jwh.2010 .2233
22. Pastore I, Chiefari E, Vero R, Brunetti A (2017) Postpartum glu-cose intolerance: an updated overview. Endocrine. http s://doi. org/10.1007 /s120 20-017-1388 -0
23. White IR, Royston P, Wood AM (2011) Multiple imputation using chained equations: issues and guidance for practice. Stat Med 30(4):377–399. http s://doi.org/10.1002 /sim.4067
24. Coustan DR, Carpenter MW, O’Sullivan PS, Carr SR (1993) Gestational diabetes: predictors of subsequent disordered glucose metabolism. Am J Obstet Gynecol 168(4):1139–1144 (discussion
44–5)
25. Kjos SL, Buchanan TA, Greenspoon JS, Montoro M, Bernstein GS, Mestman JH (1990) Gestational diabetes mellitus: the preva-lence of glucose intolerance and diabetes mellitus in the first two months post partum. Am J Obstet Gynecol 163(1 Pt 1):93–98 26. Schaefer-Graf UM, Buchanan TA, Xiang AH, Peters RK, Kjos
SL (2002) Clinical predictors for a high risk for the develop-ment of diabetes mellitus in the early puerperium in women with recent gestational diabetes mellitus. Am J Obstet Gynecol 186(4):751–756
27. Nielsen LR, Ekbom P, Damm P, Glumer C, Frandsen MM, Jensen DM et al (2004) HbA1c levels are significantly lower in early and late pregnancy. Diabetes Care 27(5):1200–1201
28. Wild S, Roglic G, Green A, Sicree R, King H (2004) Global preva-lence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27(5):1047–1053
29. Karve A, Hayward RA (2010) Prevalence, diagnosis, and treat-ment of impaired fasting glucose and impaired glucose tolerance in nondiabetic U.S. adults. Diabetes Care 33(11):2355–2359.
http s://doi.org/10.2337 /dc09 -1957
30. American Diabetes Association (2015) 5. Prevention or delay of type 2 diabetes. Diabetes Care 38(Suppl 1):S31–S32. http s://doi. org/10.2337 /dc15 -S008
Affiliations
Inês Gante1 · Ana Carina Ferreira2 · Gonçalo Pestana3 · Daniela Pires4,5 · Njila Amaral6 · Jorge Dores7 · Maria do Céu Almeida1 · José Luis Sandoval8
1 Department of Obstetrics, Maternidade Bissaya Barreto - Centro Hospitalar e Universitário de Coimbra, Rua Augusta, 3000-061 Coimbra, Portugal
2 Department of Nephrology, Hospital Curry Cabral - Centro Hospitalar Lisboa Central, Rua Beneficência 8, 1069-166 Lisbon, Portugal
3 Department of Cardiology, Centro Hospitalar de São João, Alameda Prof. Hernâni Monteiro, 4200–319 Porto, Portugal 4 Department of Infectious Diseases, Centro Hospitalar de
Lisboa Norte and Faculdade de Medicina de Lisboa, Av. Egas Moniz, 1649-035 Lisbon, Portugal
5 Infection Control Program, Geneva University Hospitals, Rue Gabrielle Perret-Gentil, 1205 Geneva, Switzerland
6 Department of Obstetrics and Gynecology, Hospital Beatriz Angelo, Avenida Carlos Teixeira 3, 2674-514 Loures, Portugal
7 Department of Endocrinology, Centro Hospitalar do Porto, Largo Prof. Abel Salazar, 4099-001 Porto, Portugal
8 Unit of Population Epidemiology, Department of Community Medicine, Primary Care, and Emergency Medicine,
Geneva University Hospitals, Rue Gabrielle Perret-Gentil, 1205 Geneva, Switzerland