296
Rev Bras Cir Cardiovasc | Braz J Cardiovasc Surg
Rev Bras Cir Cardiovasc 2013;28(2):296-8 Disli OM, et al. - Use of autologous pericardium for mitral leaflet
reconstruction in a child with endocarditis
RBCCV 44205-1471 DOI: 10.5935/1678-9741.20130042
Use of autologous pericardium for mitral lealet
reconstruction in a child with endocarditis
Uso de pericárdio autólogo para reconstrução de folheto mitral em criança com endocardite
Olcay Murat Disli
1, Cemsit Karakurt
2, Nevzat Erdil
3, Bektas Battaloglu
31. Associate professor at Inonu University, School of Medicine, Malatya, Turkey. Had primary responsibility for protocol development, outcome assessment, preliminary data analysis and writing the paper.
2. Associate professor at Inonu University, School of Medicine, Malatya, Turkey. Participated in the development of the protocol and cardiologic assessment. 3. Professor at Inonu University, School of Medicine, Malatya, Turkey.
Participated in the development of the protocol.
Work carried out at Inonu University, School of Medicine, Department of Cardiovascular Surgery, Malatya, Turkey.
Correspondence address: Olcay Murat Disli
Inonu University, School of Medicine, Turgut Ozal Medical Center, Department of Cardiovascular Surgery, 44280 Malatya, Turkey.
E-mail: [email protected]
Article received on September 4th, 2012 Article accepted on November 8th, 2012
CASE REPORT
Abstract
We present a case of successful repair of the mitral valve for active infective endocarditis. Mitral valve repair was performed through debridement of vegetation and abscess, resection and
repair of the posterior mitral lealet and posterior repair with
autologous pericardium. Postoperative period was uneventful-ly, with no evidence of recurrent infection, and echocardiogram showed mitral valve competence with mild mitral regurgitation. We demonstrate that valve repair is a feasible choice in cases of active endocarditis in children.
Descriptors: Endocarditis, subacute bacterial. Child. Mitral valve/surgery. Pericardium.
Resumo
Apresentamos um caso de reparo bem-sucedido da valva mi-tral decorrente de endocardite infecciosa ativa. Reparo da valva mitral foi acompanhado de desbridamento da vegetação e do abscesso, ressecção e plastia do folheto mitral posterior, e anu-loplastia posterior com pericárdio autólogo. Pós-operatório sem evidências de infecção recorrente, e ecocardiograma demonstrou competência da valva mitral com regurgitação mitral trivial. Concluímos que o reparo valvar é uma escolha viável em caso de endocardite ativa nas crianças.
Descritores: Endocardite bacteriana subaguda. Criança. Valva mitral/cirurgia. Pericárdio.
INTRODUCTION
Infective endocarditis (IE) is a condition that is rarely observed among children. It is associated with a postoperative mortality rate of less than 5%. In general, mitral valve replacement is performed for the treatment of mitral valve regurgitation that develops as a result of infective endocarditis. However, recently performed clinical studies have shown that
patients with isolated mitral valve IE may also beneit from
mitral valve repair [1].
There are considerable technical dificulties associated
with the surgical procedures involved when the mitral valve is affected by endocarditis. In the article, we describe a case
of successful mitral endocarditis treatment by describing how valve repair was performed in this particular case.
CASE REPORT
Signs of infection accompanied by weakness and high fever were observed in a 9 year old boy, despite antibiotic administration for the previous 2 weeks. Severe mitral regurgitation 3x2 cm was observed during transesophageal echocardiography (TEE) (Figure 1A), and a perforation was
identiied on the posterior lealet together with a considerably
297
Rev Bras Cir Cardiovasc | Braz J Cardiovasc Surg
Rev Bras Cir Cardiovasc 2013;28(2):296-8 Disli OM, et al. - Use of autologous pericardium for mitral leaflet
reconstruction in a child with endocarditis
Abbreviations, acronyms & simbols
IE TEE
Infective endocarditis
Transesophageal echocardiography
Staphylococcus aureus, and abscesses were visible beyond the
posterior lealet on the adjacent wall. Standard cardiopulmonary
bypass, with blood cardioplegia maintained at mild hypothermia, was used for surgery. During the procedure, the abscess was debrided and the mitral valve was reconstructed. Mitral repair was performed on the posterior mitral valve leaflet using quadrangular resection, and the body of the posterior valve and the locations of abscess resection were reconstructed
with fresh autologous pericardium (Figure 2). Recovery from cardiopulmonary bypass was without any adverse events. Intraoperative TEE demonstrated competence for the valve. Following surgery, antibiotic treatment was administered for the ensuing 6 weeks, and recurrence of infection was not observed. No adverse events occurred during the postoperative period, and the mitral valve displayed minimal regurgitation. Mitral valve competence was measured 6 months after the surgery, and cardiac performance was eventually observed to be normal. (Figure 1B) Patient was discharged 14 days after the surgery, with perioral antibiotic therapy being continued following discharge. The bacterial mass was mostly composed of Gram
positive bacteria within the vegetation, but no speciic pathogen
developed from the culture of the excised vegetation.
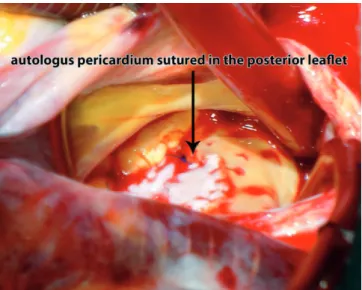
Fig. 2 – Following aggressive debridement of the posterior lealet
and the left atrial wall, the infected zone was resected and replaced with autologous pericardium
Fig. 1 – Transthoracic echocardiogram showing large mitral vegetation (31x 22 mm)
DISCUSSION
According to the American College of Cardiology/ American Heart Association 2006 Guidelines, mitral valve repair is strongly recommended in active infective endocarditis against the risk of infection with prosthetic materials [2]. Endocarditis surgery involves full excision of the infective and necrotic areas, which serves to restore the structure of the operated regions. For infective valve diseases, Carpentier [3] and Dreyfus et al. [4] have recommended the thorough debriding of the infected valve by means of direct surgical intervention at an early stage. Hence, the surgery is to be performed while infection is only limited to the area of the heart valve tissue, and before ventricular function is impaired in the patient. Tenório et al. [5] suggested that pericardial patch must comprise the body of the posterior
lealet to which the anterior lealet will coopt during the
systole. It is important that the coopting area between the
298
Rev Bras Cir Cardiovasc | Braz J Cardiovasc Surg
Rev Bras Cir Cardiovasc 2013;28(2):296-8 Disli OM, et al. - Use of autologous pericardium for mitral leaflet
reconstruction in a child with endocarditis
An independent risk factor associated with surgeries for mitral valve repair is annular abscesses. It is possible for pericardial patch or bovine pericardium to be employed for
annular reconstruction. For coaptation between the two lealets,
annuloplasty can be performed while the mitral annulus is dilated. However, we chose not to follow this approach for this patient. By conserving subvalvular apparatus, it is possible to preserve left ventricular function and to increase the long-term survival of the patient. In patients with infective
endocarditis there is a deinite advantage of TEE to provide
better visualization of the shape and size of a vegetation, as well as the surrounding tissues, severity of valvar regurgitation, and associated hemodynamics. Therefore, in this case,
intraoperatively saline injection through the valves and TEE
were performed to assess the adequacy and success of repair. We infer from the abovementioned case that further emphasis should be placed on preserving the patient’s native valve, regardless of the unfavorable clinical and pathological picture that the patient may display. This is especially important in child patients, since mitral repair reduces the risk of thromboembolism, and thereby removes the need for
using anticoagulants that are dificult to manage in a pediatric
population. Furthermore, an advantage of mitral repair is that it that removes the risk of prosthetic valve endocarditis. On
the other hand, dificulties concerning its mechanical use are
the potential patient-prosthesis mismatch and the eventual necessity of reoperation due to the child outgrowing the
prosthetic valve. Mihaljevic et al. [6] have described patients
with advanced endocarditis and annular destruction need to have their prosthesis replaced.
We consider that the percentage of repair can be increased by an active annulus. However, we also consider that the unstable preoperative hemodynamics nevertheless leads immediate valve replacement to be preferred over complicated valve repair for many surgeries, as this approach may have
the beneit of shortening the surgery period and increasing the
chances for survival. CONCLUSION
Mitral valve repair with autologous tissue is an approach that is likely to yield better surgery and results. Improved
late survival, elimination of the necessity for re-operation, and functional outcomes can be achieved by preserving the valve tissue. As such, the case described above demonstrates that valve repair is an alternative approach for the treatment of active infective endocarditis that affects the mitral valve in children.
REFERENCES
1. Iung B, Rousseau-Paziaud J, Cormier B, Garbarz E, Fondard O, Brochet E, et al. Contemporary results of mitral valve repair for infective endocarditis. J Am Coll Cardiol. 2004;43(3):386-92.
2. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons, Bonow RO, Carabello BA, Kanu C, de Leon AC Jr, Faxon DP, Freed MD, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006;114(5):e84-231.
3. Carpentier A. Cardiac valve surgery: the “French correction”. J Thorac Cardiovasc Surg. 1983;86(3):323-37.
4. Dreyfus G, Serraf A, Jebara VA, Deloche A, Chauvaud S, Couetil JP, et al. Valve repair in acute endocarditis. Ann Thorac Surg. 1990;49(5):706-11.
5. Tenório EM, Moraes Neto F, Chauvaud S, Moraes CR. Experience
with the posterior lealet extension technique for correction of rheumatic mitral insuficiency in children. Rev Bras Cir
Cardiovasc. 2009;24(4):567-9.
6. Mihaljevic T, Paul S, Leacche M, Rawn JD, Aranki S, O'Gara