RevBrasAnestesiol.2015;65(5):384---394
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
REVIEW
ARTICLE
Perioperative
morbidity
and
mortality
in
the
first
year
of
life:
a
systematic
review
(1997---2012)
Dora
Catré
a,b,∗,
Maria
Francelina
Lopes
b,c,
Joaquim
Silva
Viana
d,
António
Silvério
Cabrita
baCentroHospitalarTondela-Viseu,Viseu,Portugal
bFaculdadedeMedicina,UniversidadedeCoimbra,Coimbra,Portugal
cHospitalPediátrico,CentroHospitalareUniversitáriodeCoimbra,Coimbra,Portugal
dFaculdadedeCiênciasdaSaúde,UniversidadedaBeiraInterior,Covilhã,Portugal
Received20November2012;accepted20March2013 Availableonline27July2015
KEYWORDS
Earlymortality; Morbidity:cardiac arrest;
Perioperativecritical events/adverse events;
1-Yearold/1-month oldchildren
Abstract
Backgroundandobjectives: Althoughmanyrecognizethatthefirstyearoflifeandspecifically
theneonatalperiodareassociatedwithincreasedriskofanestheticmorbidityandmortality, therearenostudiesdirectedtothesepediatricsubpopulations.Thissystematicreviewofthe scientificliteratureincludingthelast15yearsaimedtoanalyzetheepidemiologyof morbid-ityandmortalityassociatedwithgeneralanesthesiaandsurgeryinthefirstyearoflifeand particularlyintheneonatal(firstmonth)period.
Content: ThereviewwasconductedbysearchingpublicationsinMedline/PubMeddatabases,
andthefollowingoutcomeswereevaluated:earlymortalityinthefirstyearoflife(<1year) andinsubgroupsofdifferentvulnerabilityinthisagegroup(0---30daysand1---12months)and theprevalenceofcardiacarrestandperioperativecritical/adverseeventsofvarioustypesin thesamesubgroups.
Conclusions:Thecurrentliteratureindicatesgreatvariabilityinmortalityandmorbidityinthe
agegroupunderconsiderationandinitssubgroups.However,despitetheobvious methodo-logicalheterogeneityandabsenceofspecificstudies,epidemiologicalprofilesofmorbidityand mortalityrelatedtoanesthesiainchildren inthefirst yearoflifeshow higherfrequencyof morbidityandmortalityinthisagegroup,withthehighestpeaksofincidenceintheneonates’ anesthesia.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](D.Catré). http://dx.doi.org/10.1016/j.bjane.2013.03.025
Perioperativemorbidityandmortalityinthefirstyearoflife 385
PALAVRAS-CHAVE
Mortalidadeprecoce; Morbidade:parada cardíaca;
Eventoscríticose adversos
perioperatórios; Crianc¸asdeum ano/ummêsdeidade
Morbimortalidadeperioperatórianoprimeiroanodeidade:revisãosistemática (1997-2012)
Resumo
Justificativaeobjetivos: Emboramuitosreconhec¸amqueaidadeinferioraumanoe
especifi-camenteoperíodoneonatalestejamassociadosamaiorriscodemorbimortalidadeanestésica, nãoexistemestudosdirigidosaessassubpopulac¸õespediátricas.Estarevisãosistemáticadas publicac¸õescientíficasdosúltimos15anostevecomoobjetivoanalisaroperfilepidemiológico damorbimortalidaderelacionadacomaanestesiageralecirurgianoprimeiroanodeidadee emparticularnoperíodoneonatal(primeiromêsdeidade).
Conteúdo: A revisão foi conduzida por pesquisa de publicac¸ões nas bases de dados
Med-line/PubMed.Foramavaliadososseguintesdesfechos:mortalidadeprecoce noprimeiro ano de idade(<1A) eem subgrupos dediferente vulnerabilidadenestafaixa etária(0-30 diase 1-12meses)eprevalênciadeparadacardíacaeeventoscríticos/adversosperioperatóriosde diversostiposnosmesmossubgrupos.
Conclusões: Aliteraturacorrenteindicagrandevariabilidadenosíndicesdemortalidadee
mor-bidadenafaixaetáriaemanálise,bemcomonosseussubgrupos.Noentanto,apesardaóbvia heterogeneidade metodológicaedaausênciadeestudos específicos,osperfis epidemiológi-cos demorbimortalidaderelacionadacomaanestesiadecrianc¸asnoprimeiro anodeidade mostramfrequênciamaisaltademorbimortalidadenessafaixaetária,comosmaiorespicosde incidêncianaanestesiadeneonatos.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Information onmorbidity and mortality inpediatric anes-thesiaisabundant,butscattered.Althoughmanyrecognize that age <1 year and specificallythe neonatal periodare associatedwithhigher risk ofanesthetic complications,1,2
therearenostudiesaimedatthisagegroup.Availabledata
arescatteredin studiesthatcovera widerrangeofages,
with reports differing from the results in these pediatric
groups.
Theimprovedsurvivalincongenitalpathologies,aswell
asthedevelopmentofnewsurgicaltechniquesinpediatrics,
ledtoanincreaseinthenumberofsurgeriesperformedin
childrenunderoneyearofage,manyofwhichinextremely
vulnerable infants.3 The anesthesia of pediatric patients
youngerthan 1 yearhas veryspecific characteristics, and
the results of pediatric studies in older children are not
necessarilyapplicabletothem.
Althoughtheriskofanestheticcomplicationsis
presum-ably associatedwith population characteristics, thestudy
of morbidity and mortality related to anesthesia care in
the pediatric population younger than one year has
spe-cialrelevanceforitsfrequencyandconsiderableimpacton
patients’health.Thecharacterizationofthe
epidemiologi-calprofileofmorbidityandmortalityinthisagegroup,asan
instrumentofhealth carequalityevaluation,can improve
anesthesia in this group of very particular characteristics
and provide a starting point for reducing morbidity and
mortality.1,4---6
This systematicreviewofscientificstudiespublishedin
thelast15yearsaimedtoanalyzetheepidemiological
pro-fileofmorbidityandmortalityrelatedtogeneralanesthesia
in the first year of age, and particularly in the
differ-entvulnerablesubgroups:firstmonth and fromoneto12
months.
Methods
Weperformedasystematicsearchofthestudiespublishedin
Medline/Pubmed(http://www.ncbi.nlm.nih.gov/pubmed/)
from 1 January 1997 to 31 October 2012 to find
orig-inal articles on mortality or morbidity associated with
the perioperative period of children under one year of
age. The following keywords were used in the search:
anesthesia-related and mortality and anesthesia-related
andmorbidity.Fromthetitleorabstractofthepotentially relevantarticles,weusedthePubMedfunctionrelated arti-cles.Additionalreferencesfromthisresearchandrelevant
studiescitedwereincluded.
Thesearchwaslimitedtohumanstudiesandthelast15
years.
Alltitles,abstracts,andfulltextsofpotentiallyrelevant studieswereevaluatedforeligibilitybasedontheinclusion
orexclusioncriteriapreviouslydetermined.
Inclusioncriteriawerestudies evaluatingtheincidence
ofearly mortalityor perioperativecardiac arrestor criti-cal/adverseeventsofvarioustypes,asdefinedbydifferent authors,withinformationregardingthespecificsubgroupof childrenunderoneyearofage(group<1Y).Whenages0---30
daysand1---12monthswerespecified,thesedatawerealso
collected.
Exclusioncriteriawerestudieslimitedtoasingleregional
386 D.Catréetal.
Datawerecollectedindependentlybytwoauthorsofthis
study(DCandMFL).
Of each selected article, data on the type of study,
geographicarea,number of cases,number of anesthesia,
typeofsurgery,andperioperativemortalityandmorbidity
werecollected.Regardingmortality,dataonthemortality
rateper10,000anesthesiaswerecollectedandtheperiods
in which death occurred: in the operating
room/post-anesthesiacare unitorin thepostoperativeperiodatany
timewithin30days.Regardingmorbidity,dataontherate
ofperioperativecardiacarrestwerecollected.Inaddition
tothiscriticalevent, weharvested informationregarding
critical/adverse events of various types (defined by the
respectiveauthors)whenevermentionedintherevised
pub-lication.
Results
Theinitialsearchforpublications,limitedtohumansandthe
mentionedperiod,originated 104 and144articlesfor the
anesthesia-related and mortality and anesthesia-related
andmorbiditycombinations,respectively.Afterreadingthe
titleor abstractof these articles and other relevant
sur-veyedbytherelatedarticlesfunctionandcitedreferences,
the selection included 20 articles reporting perioperative
mortality or morbidity related to anesthesia in children
underoneyearofage.Fullanalysisofthesearticlesledto theexclusionofonesystematicreview.1Thus,ourstudydata
representacompilationofinformationfrom19articles.2,7---24
In16articlesofincidence,2,7---21tworeportedseriesinwhich
patientswerealsoincludedinpreviousarticles:thestudyby Braz200617includeddatafromBraz200418andthestudyby
Kawashima200215 includeddatafromMorita2001.7These
data analysis was made to complement the information,
butnottoduplicate.Theremainingthreepublications22---24
refertomulticenterdatabase ofreportedcases.All
stud-iesarelevelBof scientific evidence,according toOxford
classification.25
DataonmortalityarepresentedinTables1and2anddata
onmorbidityinTables3and4.Table5compilesmortality
profilesandcardiacarrests inthedifferentagesubgroups
withinthefirstyearofage.
Mortalityinchildreninthefirstyearofage
Mortality rates reportedin the literature included in the
studyarepresentedintablesoneandfive.Five10---14ofthe
eightstudies in Table 1 have informationon overall
mor-tality per 10 thousandanesthesia in the first year of age
(<1Yor0---12M).There isagreatvariability, from11.4 to
38.9per10,000anesthesiasduringsurgeryandimmediate
postoperativeperiod(an average of30 deaths per10,000
anesthesias,calculatedonthebasis oftwoseries10,12 that
totaled13,634anesthesia)and35.1to59.7per10,000 anes-thesiasuptothefirst24hafteranesthesia(an averageof
53deaths per10,000 anesthesias,calculatedon thebasis
oftwolargeseries[1,141]thattotaled20,661anesthesia).
Themortalityratewithinthefirsttwodaysofanesthesia,
assessedin astudy13 involving pediatricpatients upto18
yearsofage andwith4863anesthesiasinthefirstyearof
age, was 18.5 per 10,000 anesthesias. In another study14
involvingpediatricpatientsupto18yearsandwith15,255
anesthesiasinthefirstyearofage,themortalityraterelated
toanesthesiaat30dayswas135per10,000anesthesias.
Theanalysisoftheseresultsallowshighlightingthe
fol-lowingfeatures:
1. The definition of death during the intraoperative and
earlypostoperativeperiodsorrelatedtoanesthesiahas
noconsensusintheliterature,butregardlessofthe crite-riaused,thestudiesinvolvingmultipleagegroupsfound
highermortalityrateinchildrenunderoneyear ofage
whencomparedtoolderchildren.
2. DatapresentedinTable1indicatingveryhighmortality
ratesinthestudybyChanetal.,9VanderGriendetal.,14
andFlicketal.10shouldbereadinthiscontextofcriteria
variability, asit refer to the totalanesthetized cases, includingcardiacsurgery,and,inthecaseofChanetal.,9
transplants.VanderGriendetal.14andFlicketal.10also
report in their publications the mortality rate in
non-cardiacsurgery, which drops from59.7to 39.7/10,000
anesthesiasinthefirst24hoursinthestudybyVander Griendetal.14andfrom38.9to5/10,000anesthesiasin
thestudybyFlicketal.10
Mortalityinsubgroupsofchildrenundertheageof 1year(0---30daysand1---12months)
Tables1and5haverelevantdataonmortalityrateduring
thefirstmonthofageandfrom1to12months,andTable2
showsthestudieswhichindicatethecauseofdeath.
Five7---14 of the eight selected studies to evaluate the
mortalityratecontaindatafor analysisof thisoutcome in
subgroupsfirstmonth(0---30days)and12monthsofage.
Thedeathratesduringsurgeryandpostoperativeperiod
of anesthesias in neonates and children aged one to 12
monthsanalyzedinastudy10thatinvolvingchildrenupto18
years,with1451anesthesiasinneonatesand7807
anesthe-siasinchildrenagedoneto12monthswere,respectively,
144.7and19.2per10,000anesthesias.Inthefirst24hours, themortalityratespresentedintwostudies9,14rangedfrom
180.1to288per 10,000anesthesiasin neonatesandfrom
32.2to129per10,000anesthesiasinchildrenagedoneto
12months.Mortalityratesinthefirstsevendaysanalyzed
intwostudies7,8rangedfrom26.94to74.10andfrom5.91
to 6.63 per 10,000 anesthesias, respectively, in neonates
andchildrenaged1---12months.Inanotherstudy14involving
pediatricpatientsupto18yearsofageandwith2831
anes-thesiasinneonatesand12,424anesthesiasinchildrenaged
1---12months,the30daysmortalityrateswere,respectively,
367.4and82.1per10,000anesthesias.
Thefollowingaspectsarehighlighted:
1. As in theanalysis ofmortality ratein thefirst year of
age,theanalysisofmortalityratesinthetwosubgroups
ofthis agegrouprevealsthe samemethodological
dif-ferencesandthe need for criticalevaluation fromthe
standpointthisvariability.Theanalysisoftheseprofiles showsthatthepeakriskofmortalityisconsistentinthe
anesthesiagroupofneonates,comparedwiththegroup
P
erioperative
morbidity
and
mortality
in
the
first
year
of
life
387
Table1 Incidenceofintraoperativeandearlypostoperativemortalityinchildrenunder1yearofage.
Author/s(year);typeof publication;periodof investigationand location
Deaths includedin datacollection
Numberofprocedures, maximumage
Overall mortalityinthe study/10,000 anesthesias
Subgroupsunder1yearofage
Age Numberof
anesthesias
Incidence/10,000 anesthesias
Moritaetal.(2001)7; R-M;1999;Japan
First7days 732,788anesthesias atallages
ND 0---30d 3509 74.10
1---12M 13580 6.63
Moritaetal.(2002)8; R-M;2000;Japan
First7days 910,757anesthesias atallages
ND 0---30d ND 26.94
1---12M ND 5.91
ChaneAuler(2002)9; R-1C;1998---1999;Brazil
First24hours 82,641anesthesiasat allages
51 0---30d ND 288
1---12M ND 129
Flicketal.(2007)10; R-1C;1988---2005;USA
ORandPACU 92,881anesthesiasin childrenunder18
6.8 0---30d 1451 144.7
1---12M 7807 19.2
Geral<1Y 9258 38.9
Bunchungmongkoletal. (2007)11;P-M; 2003---2004;Thailand
First24h 25,098anesthesiasin childrenupto15years
15.9 0---12M 5406 35.1
Ahmedetal.(2009)12; R-1C;1992---2006; Pakistan
ORandPACU 20,216anesthesiasin childrenunder18
3.46 0---12M 4376 11.4
Bhartietal.(2009)13; R-1C;2003---2008; India
First2days 12,158anesthesiasin childrenunder18
10.7 0---12M 4863 18.5
VanderGriendetal. (2011)14;R-1C; 2003---2008;Australia
First24hours 10.1855anesthesiasin childrenunder18
24h:13.4 24h
0---30d 2831 180.1
1---12M 12,424 32.2
Geral<1Y 15,255 59.7
30d:34.5 30d:0---30d 2831 367.4
1---12M 12,424 82.1
Geral<1Y 15,255 135.0
388 D.Catréetal.
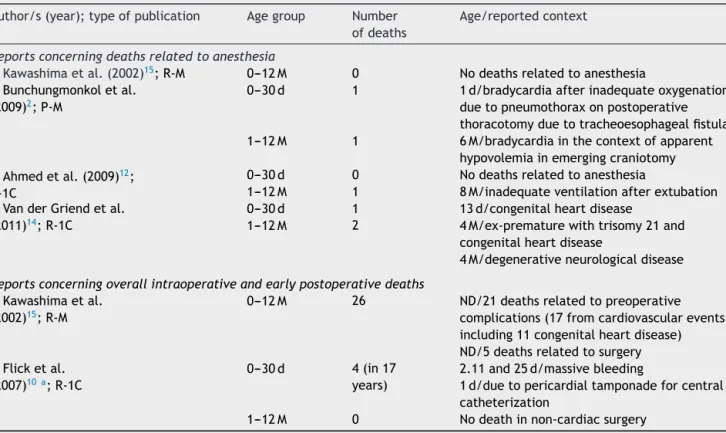
Table2 Mortalitycontextinchildrenunder1yearofagereportedintheliteratureoverthelast15years.
Author/s(year);typeofpublication Agegroup Number ofdeaths
Age/reportedcontext
Reportsconcerningdeathsrelatedtoanesthesia
Kawashimaetal.(2002)15;R-M 0---12M 0 Nodeathsrelatedtoanesthesia Bunchungmonkoletal.
(2009)2;P-M
0---30d 1 1d/bradycardiaafterinadequateoxygenation duetopneumothoraxonpostoperative thoracotomyduetotracheoesophagealfistula 1---12M 1 6M/bradycardiainthecontextofapparent
hypovolemiainemergingcraniotomy Ahmedetal.(2009)12;
R-1C
0---30d 0 Nodeathsrelatedtoanesthesia
1---12M 1 8M/inadequateventilationafterextubation VanderGriendetal.
(2011)14;R-1C
0---30d 1 13d/congenitalheartdisease
1---12M 2 4M/ex-prematurewithtrisomy21and
congenitalheartdisease
4M/degenerativeneurologicaldisease
Reportsconcerningoverallintraoperativeandearlypostoperativedeaths
Kawashimaetal. (2002)15;R-M
0---12M 26 ND/21deathsrelatedtopreoperative complications(17fromcardiovascularevents, including11congenitalheartdisease) ND/5deathsrelatedtosurgery Flicketal.
(2007)10a;R-1C
0---30d 4(in17 years)
2.11and25d/massivebleeding
1d/duetopericardialtamponadeforcentral catheterization
1---12M 0 Nodeathinnon-cardiacsurgery
R-M,retrospectivemulticenter;P-M,prospectivemulticenter;R-1C,retrospective1center;M,month;d,day;ND,unavailable informa-tion.
aInformationregardingnon-cardiacsurgery.
2. InthedataanalysisofKawashimaetal.,15regardingthe
compilation and analysis of data presented by Morita
etal.7 forthe annualstudy ofmortalityandmorbidity
inJapanin1999,mortalitywashigherinchildrenunder
onemonth ofage.However,mortalityinchildren aged
between one and12 months,even though higherthan
that ofolder children,hasbeen supersededby thatof
individualsagedbetween66and85yearsormore.
3. Although several studies refers to the most frequent
causesofdeathandriskfactors,mostofthemdoesnot
contain or analyzes this data in different age groups;
therefore, specific datafor childrenunderoneyear of
agearerareandtheexistingdatagenerallyreferonlyto
theanesthesia-relateddeaths.Thisinformationis
com-piledinTable2.
Perioperativemorbidity
Regardingperioperativemorbidity,studiesshow great
dis-parity between the available data. Some authors have
chosentoanalyzethecardiacarrestsin theperioperative
period(Table3), whileothers evaluatedawider rangeof
critical/adverseevents(Table4).
Perioperativemorbidityinthefirstyearofage
InTable 3, six10---13,16,17 of theeight listed articlescontain
informationontherateofcardiacarrestper10,000 anesthe-siasinthefirstyearofage.Ofthesesixarticles,fivereferto
theoperatingroomandpost-anesthesiacareunitandoneto
thefirst24h.Table5presentstheprofileofcardiacarrests inthedifferentsubgroupsoffirstyearofage.
Itwasnotedthat therateofcardiac arrestper 10,000
anesthesiasintheoperatingroomandpost-anesthesiacare
unit ranged from8.916 to 87.117 (average of 38.6 cardiac
arrests per 10,000 anesthesias, calculated based on five
majorseries10,12,13,16,17 totaling25,392anesthesias);andin
onestudy11 ofthefirst24h, theratewas48.1per 10,000
anesthesiasinauniverseof5406anesthesias.
Therateofperioperativecritical/adverseeventsof
dif-ferenttypesassociatedwithanestheticprocedures(Table4)
rangedfrom4.6%to30.8%.
Wehighlightthefollowingaspectsofthecriticalanalysis ofTables3and4andtherelatedliteraturedata:
1. Aswithmortality,thecriteriausedtocalculatethe inci-denceofcardiacarrestorcritical/adverseeventsvaried.
Thereisthereforeadiscrepancyinthevaluespresented
thatmustbeinterpretedinitscontext.Forexample,the incidenceofcardiacarrestreportedbyFlick etal.10 is
total,includingcardiacsurgery.Inthisstudy,inchildren
underoneyear ofage, theincidenceof cardiacarrest
consideringonlynon-cardiacsurgerywas8.7per10,000
anesthesias,one-fifthofthetotalincidence.
2. In all studies found, the incidence of cardiac arrest
andcritical/adverseeventsofvarioustypeswashigher
in children aged less than one year than in older
P
erioperative
morbidity
and
mortality
in
the
first
year
of
life
389
Table3 Incidenceofperioperativecardiacarrestinchildrenunder1yearofage.
Author/s(year);typeof publication;periodof investigationand location
Cardiacarrest Numberofprocedures, maximumage
Overallincidencein thestudy/10,000 anesthesias
Subgroupsunder1yearofage
Age Numberof anesthesias
Incidence/10,000 anesthesias
Moritaetal.(2001)7; R-M;1999;Japan
ND 732,788anesthesiasat
allages
ND 0---30d 3509 54.1
1---12M 13,580 8.8
Moritaetal.(2002)8; R-M;2000;Japan
ND 910,757anesthesiasat
allages
ND 0---30d ND 28.3
1---12M ND 8.54
Muratetal.(2004)16; P-1C;2000---2002; France
ORandPACU 24,165anesthesiasin childrenupto15years
3.3 <1Y 3681 10.9
Brazetal.(2006)17; P-1C;1996---2005;Brazil
ORandPACU 53,718anesthesiasatall ages
34.6 0---30d 846 177.3
1---12M 2368 55.1
Geral<1Y 3214 87.1
Flicketal.(2007)10; R-1C;1988---2005;USA
ORandPACU 92,881anesthesiasin childrenupto18years
8.6 0---30d 1451 158.5
1---12M 7807 23.1
Geral<1Y 9258 44.3
Bunchungmongkoletal. (2007)11;P-M; 2003---2004;Thailand
First24hours 25,098anesthesiasin childrenupto15years
19.9 <1Y 5406 48.1
Ahmedetal.(2009)12; R-1C;1992---2006; Pakistan
ORandPACU 20,216anesthesiasin childrenupto18yearsa
4.95 <1Y 4376 18.3
Bhartietal.(2009)13; R-1C;2003---2008; India
ORandPACU 12,158anesthesiasin childrenupto18years
22.2 <1Y 4863 35
R-M,Aretrospectivemulticenter;P-1C,Aprospective1center;R-1C,retrospective1center;P-M,Aprospectivemulticenter;ND,unavailableinformation;OR,operatingroom;PACU, post-anesthesiacareunit;d,days;M,months.
390
D.
Catré
et
al.
Table4 Incidenceofperioperativecritical/adverseeventsinchildrenunder1yearofage.
Author/s(year);typeof publication;periodof investigationandlocation
Occurrence period
Numberofprocedures, maximumage
Overall incidencein thestudy
Subgroupsunder1yearofage
Age Numberof anesthesias
Incidência
Tayetal.(2001)19;P-1C; 1997---1999;Singapore
ND 10,000pediatriccases 2.78% <1Y 1022 8.6%
Moritaetal.(2001)7;R-M;1999; Japan
ND 732,788anesthesiasat
allages
ND 0---30d ND 1.68%
1---12M ND 0.48%
Moritaetal.(2002)8;R-M;2000; Japan
ND 910,757anesthesiasat
allages
ND 0---30d ND 0.7%
1---12M ND 0.42%
Muratetal.(2004)16;P-1C; 2000---2002;France
ORandPACU 24,165anesthesiasin childrenupto15years
3.1%atOR 4.8%atPACU
<1Y 3681 3.6%atOR
1.47%atPACU Edomwonyietal.(2006)20;P-1C;12
months,yearunspecified;Nigeria
ORandPACU 270anesthesiasin childrenunder16years
24% 0---30d 15 26.7%
1---12M 69 6%---8.7%
Bunchungmongkoletal. (2007)11;P-M;2003---2004; Thailand
First24h 25,098anesthesiasin childrenupto15years
1.9% <1Y 5406 4.6%
Samakéetal.(2010)21;P-1C; Marc¸o-setembro2004;Mali
ND 107anesthesiasin
childrenupto12years
39% <1Y 107 30.8%
P-1C,prospective1center;R-M,retrospectivemulticenter;P-M,prospectivemulticenter;ND,unavailableinformation;OR,operatingroom;PACU,post-anesthesiacareunit;Definition ofcriticaleventoradverseevent,Ref.19 ---respiratory,cardiovascular,andrelatedtotheequipment,drugs,regionalanesthesia,andothers,includingseizures,deaths,and dental
injuries;Ref.7,8---cardiacarrest,severehypotension,severehypoxemia;Ref.16---cardiovascular,neurological,relatedtoregionalanesthesiaandothers,includinganaphylaxis,malignant
hyperthermia,doseerror,prolongedneuromuscularblockade,hypoorhyperthermia,vomiting,postoperativehemorrhage,andequipmentfailure;Ref.20 ---cardiovascular,respiratory,
neurologicalandgastrointestinal(postoperativenauseaandvomiting);Ref.11 ---pulmonaryaspiration,symptomaticesophagealintubation,desaturationformorethan3minutes,
Perioperativemorbidityandmortalityinthefirstyearoflife 391
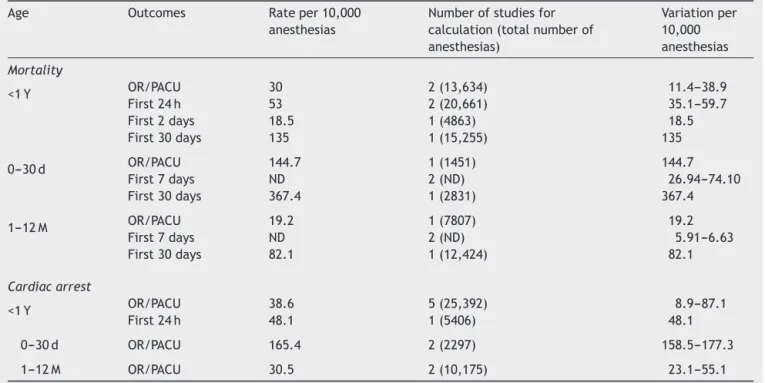
Table5 Epidemiologicalprofilesofmorbidityandmortalityinsubgroupsunder1yearofage.
Age Outcomes Rateper10,000 anesthesias
Numberofstudiesfor calculation(totalnumberof anesthesias)
Variationper 10,000 anesthesias
Mortality
<1Y OR/PACU 30 2(13,634) 11.4---38.9
First24h 53 2(20,661) 35.1---59.7
First2days 18.5 1(4863) 18.5
First30days 135 1(15,255) 135
0---30d OR/PACU 144.7 1(1451) 144.7
First7days ND 2(ND) 26.94---74.10
First30days 367.4 1(2831) 367.4
1---12M OR/PACU 19.2 1(7807) 19.2
First7days ND 2(ND) 5.91---6.63
First30days 82.1 1(12,424) 82.1
Cardiacarrest
<1Y OR/PACU 38.6 5(25,392) 8.9---87.1
First24h 48.1 1(5406) 48.1
0---30d OR/PACU 165.4 2(2297) 158.5---177.3
1---12M OR/PACU 30.5 2(10,175) 23.1---55.1
OR,operatingroom;PACU,post-anesthesiacareunit;d,day;M,month;ND,unavailableinformation.
3. Thefrequencyofcardiacarrestattheagegroupreferred to in our study is also relevant compared to older children. In the studies available, 50%---80% of cardiac arrestsinchildren occurredinpatientsunderoneyear ofage.10---13,16---18 Similarly,Morrayetal.22 intheirstudy
basedonregistrationdatafromPOCA(Pediatric
Periop-erativeCardiac Arrest Registry)stated that more than
halfofcardiacarrestsreportedbetween1994and1997
athospitalsintheUnitedStatesandCanadaoccurredin
childrenunderoneyearofage(169per289children).In thisstudy,ageasanindependentfactoroftheassociated
pathologywasnotpredictiveofmortalityaftercardiac
arrest.
4. Bhanankeretal.23showedin2007anupdateofthePOCA
Registryinwhichitisnoticeabletherelativepercentage
decreaseof cardiac arrests reportedin children under
oneyearofagecomparedtodataofpreviousyears
pre-sentedbyMorrayetal.22 However,withoutinformation
onthenumber ofanesthesiaperformed in hospitalsin
question, it is not possible to calculate and compare
incidences.
5. MacLennanetal.24identified606criticaleventsreported
inchildrenbetween 2006and2008 intheUnited
King-dom,ofwhich102(16.8%)inchildrenunderoneyearof
age.Asit isacompilationof reportedcasesof several
hospitals,itisalsonotpossibletocalculatetheincidence inthispopulation.
Perioperativemorbidityinsubgroupsofchildren under1yearofage
InTable3,four7,8,10,17ofeightarticlescontaininformation
regardingtherateofcardiacarrestper10,000anesthesias
duringthefirstmonthofage(0---30days)andbetweenone
and12months.Table5shows theepidemiologicalprofiles
ofcardiacarrestinsubgroups0---30daysand1---12months. Inthefirstmonthofage,therateofcardiacarrestranged
from 28.3 to 177.3 per 10,000 anesthesias and in 1---12
monthsitvariedfrom8.54to55.1per10,000anesthesias.
Inbothstudies10,17withcompletedataforthecalculationof
thenumberofcasesofperioperativecardiacarrest,amean
of165.4cases ofcardiacarrestoccurred inthe operating
roomand post-anesthesia care unity per 10,000
anesthe-siasinthefirstmonthofage,foraglobaluniverseof2297
anesthesias,andameanof30.5casesper10,000
anesthe-siasinchildren1---12months,foraglobaluniverseof10,175 anesthesias.
Forthefirstmonth ofage,therate ofcritical/adverse
eventsofvarioustypes(Table4)rangedfrom0.7to26.7%
ofanesthesiasandfor1---12months,itrangedfrom0.42to
8.7%ofanesthesias.
The highlights of the critical analysis for data of
Tables3and4andrelatedliteraturearethefollowing:
1. As for the group of children in the first year of age,
the criteriausedtocalculate the incidenceof cardiac
arrest or critical/adverse events in subgroups of 0---30
daysand1---12monthsvaried.Itwasnoticeddiscrepancy
inthevalues,whichmustbeinterpretedinitscontext.
Forexample,theincidenceofcardiacarrestpresented
by Flick et al.10 is total, including cardiac surgery. In
this study,in children underone year of age, its
inci-denceincardiacsurgerywasmuchhigher(434.8/10,000
anesthesias) than in non-cardiac surgery (39.4/10,000
anesthesias).
2. Bhanankeretal.23found93cardiacarrestsreported
392 D.Catréetal.
upto18years,ofwhich21inneonatesand53inchildren
aged1---12months,inPOCARegistrybetween1998and
2004.
Etiologyandcontextofperioperativemorbidityin childrenunder1yearofage
Theetiologyandcontextofcardiacarrestsinchildrenunder oneyearofagearemostlyspecifiedonlyincasesrelatedto anesthesia.
Thus,in thestudy of Ahmed etal.,12 of theeight
car-diacarrestsinchildren underoneyearofage,threewere
attributed toanesthetic causes, notably by hypovolemia,
inadequateventilation(citedintheanalysisof mortality),
and bradycardia after succinylcholine administration. All
wereconsideredpreventable.
In his study of 9 years, Braz etal.17 reported that all
cardiacarrestsrelatedtoanesthesiainchildrenunderone
yearofagewereduetoinefficientventilationandoccurred
inpatientsASAIIIorIV.Nodeathinthestudywasrelated
toanesthesiaandallcasesofcardiacarrestdueto
respira-toryeventoccurred inpatientswithsignificantassociated
pathology.
ThesevencardiacarrestsidentifiedbyFlicketal.10were
due to hypoxemia (n=1), massive bleeding (n=3),
possi-ble air embolism (n=1), complications related tocentral
catheterization(n=2),ofteninaggravatingcontextsas illus-tratedbythephysicalstatusASAIVorVinfivecases.
In the study by Bunchungmongkol et al.,2 in addition
tothe two cases resulting in death previously described,
caused by insufficient oxygenation and hypovolemia, the
remainingfivecardiacarrestsrelatedtoanesthesiain
chil-drenunderoneyearofageweremotivatedbymedication
errors(n=3)andinadequateoxygenation(n=2).
InJapaneseannualstudies,7,8,15theincidenceofcardiac
arrestinchildrenunderoneyearofage(andmoreexpressive
inneonates)wasmainlyattributedtocoexistingpathology.
Nocardiacarrestinneonateswasassociatedwith
anesthe-sia.Itis worthnotingthatin casesof1999, followingthe
occurrenceofcardiacarrest,80.8%ofneonatesdied.This
showsthatcardiovascularresuscitationinthisagegroupis exceptionallydifficult.15
Regardingthevariouscritical/adverseeventsinthe
pop-ulationunderoneyearofage,theliteraturedataareonce
againwidelydispersed,duetothewiderangeofdata
col-lectedandbecausethepopulationinstudiesisnorestricted
tothatagegroup.
In the assessment of 1000 pediatric anesthesias, Tay
etal.19foundanincidenceof2.8%oflaryngospasmin
chil-drenunderoneyearofage,significantlyhigherthaninolder children.
Murat etal.16 andEdomwonyietal.20 reportedintheir
studiesahigherfrequencyofcardiacandrespiratoryevents
inchildren under oneyear of age either in the operating
roomor post-anesthesiacareunit. Thesecond study adds
thatadverseeventsoccurredmorefrequentlyduring
anes-theticinduction.
Ontheotherhand,Bunchungmongkoletal.11reportthat
inthisagegroup criticalevents occurredmorefrequently
during anesthesia. Desaturation was the most common
event. In this study, children under one year of age had
significantly higher incidence of delayed esophageal
intu-bationdetection(0.17%),desaturation(2.2%),reintubation
(0.42%),cardiacarrest(0.65%),death(0.65%),and
medica-tionerror(0.07%).
Discussion
Inthissystematicreview,weemphasizethemainfindings:
(1)thehigherincidencesofmortalityandmorbidityin
chil-dren underoneyearof ageundergoinggeneralanesthesia
comparedwitholderchildren;(2)theincreasedriskinthose
incidences in children undergoing surgeryin the neonatal
period;(3)thehighfrequencyofcardiacarrestsinpatients underoneyearofageamongthetotalcardiacarrestsin chil-dren;(4)thelackofstudiescenteredintheneonatalperiod andfirstyearofage;(5)thegreatvariabilityof
methodolo-giesforthestudyofthesameconcepts.
Althoughthereareseveralstudiesofmorbidityand
mor-tality in anesthetic-surgical setting with incidence data
on pediatric population under one year of age and even
neonatal, this systematic review allowed the compilation
of several existing information that would allow both its
joint analysis and comparison with pre-existing empirical
knowledgeandtheidentificationofunansweredquestions.
Although the included studies were level B of scientific
evidence,mostofthemincludedtensofthousandsof
anes-thesiasintheirseries.
Regarding the various studies methodology, a
signifi-cant difference in the data collected definition is linked
to the period in which the incident occurred:
intraop-erative, operating room and post-anesthesia care unit,
the first 24h, the first two days, the first postoperative
week or month. On the other hand, there is no
consen-sus in the literature regarding the definition of death
and morbidity in the anesthetic/surgical context.
Sev-eral authors report death related to anesthesia, but it
is also determined in several ways: related to the
anes-thesiologist role or anesthetic technique, factors under
the anesthesiologist control, and factors such as surgical
and anesthetics, among others. Given its multifactorial
nature, dataanalysis may bemore informative ifall
fac-tors are considered rather than just trying to emphasize
the ones potentially relatedto anesthesia. Also,risk
pre-vention is more likelyif more importanceis givento the
occurrenceofdeathandmorbiditythroughoutthe
periop-erative process, and not just tothe risk of anesthesia in
particular.14
Also,the discussion of causes and risk factorsis often
limited toa wide range of ages.Of data reported in the
literature specifically related to children less than one
yearold,mortalityandmorbidityintheanestheticcontext
seemtobemorerelatedtocardiovascularandrespiratory
complications, which is consistent with the physiology of
thisage group.This trendseemstoreplacethedeaths of
olderstudies,mostlyrelatedtotheanestheticdrug,often
attributedtohalothane,myocardialdepressantdrug
espe-cially in younger children with congenital heart disease,
which,however,fellintodisuse.22,23,26Withtheuseofnew
andsaferdrugs,deathsbegantobeevidencedbybleeding,
inadequatefluidtherapy,andrespiratoryproblems.Lossof
Perioperativemorbidityandmortalityinthefirstyearoflife 393
Because the circulating volumeis smaller, these patients
aremoresensitivetoinadequatehydration,bothexcessive
and insufficient. That age is a risk factor for respiratory
complications for twomain reasons: increasedperipheral
collapsetrendduetoincreasedchestwallcomplianceand
increased vagal tone with quick response of apnea and
laryngospasmtoirritation of receptorspresent in the
air-waysbysecretions,trachealintubation,andaspiration.The
resultinghypoxia is at that ageclosely relatedto cardiac
arrest.
In general,thepediatricseriesshowan increased
inci-dence of cardiacarrests, 1.4---4.6 per 10,000 anesthesias,
comparedwithonecaseper10,000inadultseries.27Within
thefirstyear,ourstudyshowsamuchhigherincidence,with
aparticularlyhighproportionofcasesintheneonatalage
(165.4per10,000anesthesias).
The technical complications found related to central
lines placement, although of unknown incidence in the
perioperative setting, are well known in other settings,
notablyin pediatric intensivecare studies,which are
jus-tifiedbytheheartanatomyinthefirstmonthsoflife,with
thinnerwalls moresusceptibletotrauma.28 Some authors
recommendtheuseofultrasoundtoincreasethetechnique
safety.28
A common clinical implication to several studies in
the literature, whether directed to pediatric
anesthe-sia mortality or morbidity, is the guidance that pediatric
anesthesia,especiallyforyoungerchildren,shouldbe
per-formed by anesthesiologists with experience in this age
group.1,4---6,12,14,22,29
The global data analysis of pediatric cases of broader
agegroupsisnotnecessarilyapplicabletoanesthesiainthe
neonatalperiodandbeforethefirstyearofage.Therefore,
largemulticenterrandomizedstudiesspecificfortheseages
areneeded,inordertominimizeconfoundingfactorsand
biases,andthusadjusttheclinicalpracticemorecorrectly toincreasesecurity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GonzalezLP,PignatonW,KusanoPS.Anesthesia-related mor-talityin pediatricpatients:a systematicreview. Clinics(São Paulo).2012;67:381---7.
2.Bunchungmongkol N, Punjasawadwong Y, Chumpathong S, etal.Anesthesia-relatedcardiacarrestinchildren:theThai Anesthesia Incidents Study (Thai Study). J Med Assoc Thai. 2009;92:523---30.
3.KinouchiK.Anaestheticconsiderationsforthemanagementof verylowandextremelylowbirthweightinfants.BestPractRes ClinAnaesthesiol.2004;18:273---90.
4.PatersonN,WaterhouseP.Riskinpediatricanesthesia.Paediatr Anaesth.2011;21:848---57.
5.SomriM,CoranAG,HadjittofiC,etal.Improvedoutcomesin paediatricanaesthesia:contributingfactors.PediatrSurgInt. 2012;28:553---61.
6.Morray JP. Cardiac arrest in anesthetized children: recent advances and challenges for the future. Paediatr Anaesth. 2011;21:722---9.
7.Morita K, Kawashima Y, Irita K, et al. Perioperative mortal-ity and morbidity in 1999 with a special reference to age in 466 certified training hospitals of Japanese Society of Anesthesiologists ---Report ofCommittee on OperatingRoom SafetyofJapaneseSocietyofAnesthesiologists.Masui.2001;50: 909---21.
8.MoritaK,KawashimaY,IritaK,etal.Perioperativemortality and morbidityintheyear2000 in520certifiedtraining hos-pitalsofJapaneseSocietyofAnesthesiologists:withaspecial referencetoage--- ReportofJapaneseSocietyof Anesthesiol-ogistsCommittee onOperatingRoomSafety.Masui.2002;51: 1285---96.
9.Chan RP, Auler Junior JO. Retrospective studyof anesthetic deathsinthefirst24hours:reviewof82,641anesthesias.Rev BrasAnestesiol.2002;52:719---27.
10.Flick RP, Sprung J, Harrison TE, et al. Perioperative car-diacarrestsinchildrenbetween1988and 2005atatertiary referral center: a study of 92,881 patients. Anesthesiology. 2007;106:226---37.
11.Bunchungmongkol N, Somboonviboon W, Suraseranivongse S, etal.Pediatricanesthesiaadverseevents:theThaiAnesthesia IncidentsStudy(ThaiStudy)databaseof25,098cases.JMed AssocThai.2007;90:2072---9.
12.AhmedA,AliM,KhanM,et al.Perioperativecardiacarrests in children at a university teaching hospital of a devel-oping country over 15 years. Paediatr Anaesth. 2009;19: 581---6.
13.Bharti N, Batra YK, Kaur H. Paediatric perioperative car-diacarrestand itsmortality:databaseofa 60-monthperiod from a tertiary care paediatric centre. Eur J Anaesthesiol. 2009;26:490---5.
14.VanderGriendBF, ListerNA,McKenzieIM,et al. Postopera-tivemortalityinchildrenafter101,885anestheticsatatertiary pediatrichospital.AnesthAnalg.2011;112:1440---7.
15.KawashimaY,SeoN,MoritaK,etal.Anesthesia-related mor-tality and morbidity in Japan (1999). J Anesth. 2002;16: 319---31.
16.MuratI,ConstantI,Maud’huyH.Perioperativeanaesthetic mor-bidityin children: a databaseof 24,165anaesthetics over a 30-monthperiod.PaediatrAnaesth.2004;14:158---66.
17.Braz LG, Módolo NS, do Nascimento P Jr, et al. Perioper-ative cardiac arrest: a study of 53,718 anaesthetics over 9 yrfromaBrazilianteachinghospital.BrJAnaesth.2006;96: 569---75.
18.BrazLG,BrazJR,MódoloNS,etal.Cardiacarrestduring anes-thesiaatatertiaryteachinghospital:prospectivesurveyfrom 1996to2002.RevBrasAnestesiol.2004;54:755---68.
19.TayCL,TanGM,NgSB.Criticalincidentsinpaediatric anaes-thesia:anauditof10000anaestheticsinSingapore.Paediatr Anaesth.2001;11:711---8.
20.Edomwonyi NP, Ekwere IT, Egbekun R, et al. Anesthesia-relatedcomplications inchildren. MiddleEast JAnesthesiol. 2006;18:915---27.
21.SamakéB,KeitaM,MagalieIM,etal.Adverseeventsof anes-thesiainpediatricsurgeryscheduledatGabrielTourehospital. MaliMed.2010;25:1---4.
22.MorrayJP,GeiduschekJM,RamamoorthyC,etal. Anesthesia-relatedcardiacarrestinchildren:initialfindingsofthePediatric Perioperative Cardiac Arrest (Poca) Registry. Anesthesiology. 2000;93:6---14.
23.Bhananker SM, Ramamoorthy C, Geiduschek JM, et al. Anesthesia-relatedcardiacarrestinchildren:updatefromthe PediatricPerioperativeCardiac ArrestRegistry.AnesthAnalg. 2007;105:344---50.
394 D.Catréetal.
25.Oxford Centre for evidence-based medicine --- levels of evi-dence;2009,March.http://www.cebm.net/index.aspx?o=1025 [accessed17.11.12].
26.Mason LJ. An update on the etiology and prevention of anesthesia-relatedcardiacarrestinchildren.PaediatrAnaesth. 2004;14:412---6.
27.ZuercherM,UmmenhoferW.Cardiacarrestduringanesthesia. CurrOpinCritCare.2008;14:269---74.
28.LeeC,MasonL.Complicationsinpaediatricanaesthesia.Curr OpinAnaesthesiol.2006;19:262---7.