Cardoso and Paulos. Int Arch Cardiovasc Dis 2017, 1:003 Volume 1 | Issue 1 Open Access
International Archives of
Cardiovascular Diseases
Citation: Cardoso IL, Paulos AT (2017) C Reactive Protein and Cardiovascular Disease. Int Arch Cardio-vasc Dis 1:003
Received: November 01, 2017; Accepted: December 09, 2017; Published: December 11, 2017 Copyright: © 2017 Cardoso IL, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
C Reactive Protein and Cardiovascular Disease
Inês Lopes Cardoso* and Ana Teresa Paulos
Health Sciences Faculty, Fernando Pessoa University, Portugal
*Corresponding author: Inês Lopes Cardoso, Health Sciences Faculty, Fernando Pessoa University, Rua Carlos da Maia n. °296 4200-150 Porto, Portugal, E-mail: [email protected]
underlying CVD, frequently starts in childhood with the development of inflammatory processes [2].
Inflammation seems to be crucial in the development and progression of atherosclerosis from the formation of the atheriosclerotic lesion caused by lipid deposition, till rupture of fat plaques [3]. During an inflammatory reaction, there is the development of an interaction be-tween the vascular wall, inflammatory cells and plasma lipoproteins, with the release of several adhesion mol-ecules and cytokines. Together with this, acute phase markers like fibrinogen, C Reactive Protein (CRP), sial-ic acid, ceruloplasmin, among others are produced [1]. These biomarkers were mentioned in several studies as predictors of cardiovascular disease.
Prevention of cardiovascular disorders must be a pri-ority and all efforts must be done to limit disease pro-gression or avoid the development of a new CVD. In this way, the control of risk factors is a strong weapon in CVD prevention.
Cardiovascular risk factors
Most CVDs result from inadequate lifestyle and hence from controllable risk factors like smoking, sed-entarism, excessive weight, bad food diet and stress. However, there are also uncontrollable factors that contribute to the increased risk of CVD like age, fami-ly history and gender. Considering gender, last century women were more protected against CVDs than men due to the cardiovascular protection given by estrogens [4]. Nevertheless, nowadays this difference in incidence has been decreasing due to habits acquired by women like the use of oral contraceptives and tobacco.
Other risk factors that might involve genetic and
en-Abstract
Cardiovascular Diseases (CVD) are the first cause of death in developed countries, therefore it is of interest to reduce this public health problem. The development of atheroscle-rosis is the main cause of CVD. This pathology results from the accumulation of lipids in the arterial wall, that leads to a complex inflammatory process. Inflammatory biomarkers are a valuable tool in the detection and monitorization of the evolution of this process, as well as in the choice of thera-py to implement. C-Reactive Protein (CRP), determined by high sensitivity methods (hs-CRP), is the most studied bio-marker and stands out among the others, being considered an important marker of inflammation. Its importance comes from the fact that its plasma level is not affected by large di-urnal or seasonal variations, and for this reason is indicated as an important mediator of the atherosclerotic process. The goal of this work is to deepen knowledge concerning the importance of C reactive protein as a risk factor for the development of cardiovascular diseases and discuss how it can be used in primary as well as secondary prevention of CVD. The use of C reactive protein as a biomarker allows detection, monitorization and prevention of cardiovascular disease.
Keywords
Cardiovascular disease, Atherosclerosis, Inflammatory pro-cess, Inflammatory biomarkers, High sensitive C reactive protein
RevIew ARTICLe
Introduction
Nowadays, Cardiovascular Disorder (CVD) is a health problem with big relevance and concern, being associ-ated with numerous risk factors [1]. For this reason, it is considered one of the most common causes of mortal-ity and morbidmortal-ity in developed countries. Usually, indi-viduals with CVD only become symptomatic when they reach adult age, however atherosclerosis, the process
Check for updates
to endothelium is activated by adhesion molecules like Selectins (selectin-E, selectin-P), cellular adhesion mol-ecules (Inter-Cellular Adhesion Molecule-1 (ICAM-1), Vascular Adhesion Molecule-1 (VCAM-1)) and integrins. Chemotaxis and monocytes entrance to the sub-endo-thelial space is promoted by a Protein (protein-1) that potentiates attraction of monocytes, Interleukin-8 (IL-8), and one chemokine, called fractalkine. After that, monocytes and macrophages start to differentiate. Macrophages receive oxidised LDL via scavenger re-ceptor (CD36, scavenger rere-ceptor-A), becoming sponge cells, lesion indicators [1]. Later, smooth muscle cells migrate into the intima, proliferate and forma fibrous matrix, that keeps on growing, narrowing the artery.
It is believed that, during the processes of necrosis and apoptosis, lipid filled macrophages release matrix metalloproteinases, that damage the endothelium. Since LDL filled macrophages are enriched in tissue fac-tor, this one is released from the macrophage and con-tacts circulating platelets, resulting in the formation of thrombi and consequent acute coronary syndromes [1].
C Reactive Protein (CRP)
Characterization and structure
CRP was first described by Tillet and Francis, more than 70 years ago, during a study in patients having infection with Streptococcus pneumoniae. Serum ob-tained from these patients, during the acute phase of symptoms, included a substance capable of precipitat-ing the C polysaccharide of the cell wall of pneumococ-cus. This substance was called C reactive. Several stud-ies showed that this protein is undetectable in healthy patients, however reaches very high levels in patients having infections. After patient’s recovery, levels of this protein become undetectable again [18].
CRP is a member of the family of proteins called pentraxins and has a molecular weight of 115135 Da. This protein is formed by five identical non-glycosylated polypeptide chains (23027 Da) of 206 aminoacids each. The semonomers are linked in a non-covalent fashion, organized in a very stable discoid structure with resis-tance to proteolysis [19]. Each monomer has two dis-tinct faces, the recognition/binding face and the effec-tor face. The binding face, to which two calcium ions are associated, recognises the phosphocholine residues of the C polysaccharide of Streptococcus pneumoniae [20,21], and the effector face has affinity for the com-plement factor 1q and FcγRs [20].
Metabolism/Synthesis of CRP
CRP is an acute phase protein produced in liver due to stimulation by several pro-inflammatory cytokines derived from monocytes/macrophages or adipose tis-sue [11,22]. Its liver production is mainly stimulated by IL-6, being this synthesis synergically increased by IL-1 [18,23]. It is consensus that pro-inflammatory risk vironmental causes are high levels of plasma glucose,
since insulin resistance leads to dyslipidemias [5] and in-creased blood cholesterol levels in the form of LDL (that has higher chance of oxidation and deposition in blood vessels).
Still other CVD risk factors that seem to involve pure genetic causes are high plasma levels of lipoprotein (a) [6], hyperhomocysteinemia [7,8], as well as high levels of C Reactive Protein (CRP) in blood [9].
As mentioned, during the inflammation process there is an increase in acute phase biomarkers like CRP. For this reason, this proteinis of special interest since its plasma concentration is easily quantified, it has the best clinical-epidemiological correlation and, in opposition to other acute phase markers, it shows relatively stable plasma levels, allowing its correct quantification [10]. Besides these findings, this protein shows characteris-tics that make it very attractive [11]. In the first place, it is an acute phase protein, being an unspecific marker of systemic inflammation [12], whose serum levels in-crease as a response to several types of lesion, partic-ularly bacterial infections that constitute inflammatory stimuli. Secondly, its hepatic production is mainly stim-ulated by Interleukin 6 (IL-6) [11]. At the beginning of an inflammatory process, there is an increase in CRP levels in the first eight hours that can reach 300 mg/dL in 48 hours [13]. C reactive protein is an independent risk fac-tor for CVDs [10].
Growing evidences suggest that hs-CRP constitutes an important cardiovascular risk marker and is phys-io-pathologically associated with the atherosclerotic process, having value in primary and secondary preven-tion [11]. However, its serum concentrations can be in-fluenced by other factors like pharmaceutical products, hormones and tobacco [12].
Atherosclerosis
Atherosclerosis starts with systemic mediators that have a key role in its progression, as well as in its stabili-ty and plaque rupture. The association between inflam-matory biomarkers, the atherosclerotic phase and the dynamic of cardiovascular events related to atheroscle-rosis seems to be fundamental for CVD development [14]. Chronic inflammation of blood vessels seems to be the main cause of atherosclerotic plaque formation and its rupture [15]. Plaque formation results from accumu-lation of lipids, inflammatory cells and fibrotic elements, that deposit in the wall of arteries and blood vessels, leading to their obstruction [16].
The inflammatory process initiates with the increase of endothelium permeability to inflammatory cells, giv-ing rise to oxidized LDL deposition [17]. After endotheli-um dysfunction, mononuclear cells like monocytes and T lymphocytes adhere firmly to the endothelium and migrate to involving tissues (sub-endothelial space) by a process called diapedesis. The attachment of leucocytes
Between all existing markers, CRP shows up due to its high sensitivity in evaluating inflammatory states, showing a strong increase as a response to several in-flammatory and infectious stimuli. Measurement of CRP plasma levels helps the clinical evaluation of the pres-ence, extension and activity of the inflammatory pro-cess and the follow-up of the evolution and therapeutic response [28].
CRP detection and development of
atherosclero-sis
In the beginning, CRP plasma levels were determined by serum-agglutination performed in latex particles in a slide. This assay allowed a semi-quantitative determi-nation, with a subjective interpretation. Later, quanti-tative methods for CRP quantification were developed through immunoturbidimetry and nephelometry [32].
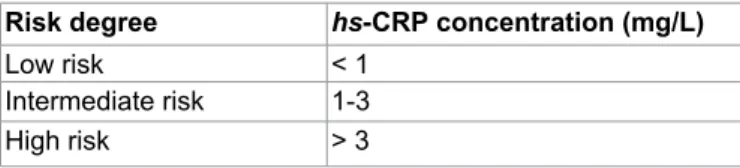
Due to the low sensitivity of these methods on de-tection of low levels of inflammation, in the 90s a high sensitivity nephelometry method for detection of very low levels of serum CRP was developed, called high sen-sitivity CRP (hs-CRP). This is the ideal laboratory meth-od in use to determine cardiovascular risk linked with chronic systemic vascular inflammation of atherosclero-sis, having a detection limit of 0.3 mg/L [11].
Table 1 describes the relationship between hs-CRP plasma concentrations and the risk factor, or capacity of cardiovascular events prediction.
Several studies confirm that hs-CRP predicts cardio-vascular events in healthy women [33] and men [34], in individuals with traditional risk factors [35] or with CVD [23]. The capacity of hs-CRP to predict CVD risk is in-dependent from traditional risk factors [34,36]. hs-CRP is an additional risk factor for coronary artery disease when associated with high plasma levels of cholesterol [22,37].
For many years, CRP was used as a complementary method for diagnosis of inflammatory processes of any nature. Meanwhile, with the discovery of inflammatory components involved in cardiovascular events, mainly atherosclerosis, CRP was assigned as a risk indicator for coronary disease and cerebral vascular accidents [28], being an inflammatory marker considered strong pre-dictor, that is independent of the risk for cardiovascular event or death.
Several prospective clinical studies have shown that CRP is associated with mortality risk in short or long term both in patients having acute or chronic ischemic factors like oxidized LDL and infectious agents such as
Chlamydia pneumoniae trigger a pro-inflammatory
re-sponse [24]. This response leads to the increase in IL-1β and TNF-α secretion, that consequently provokes release of cytokine IL-6. More over, IL-6, after binding to its receptor in liver, leads to secretion and release of CRP and amyloid A serum protein [22].
Besides liver production, data suggests that CRP is also produced in the atherosclerotic lesion (specially in smooth muscle and macrophages), in kidneys, neurons and alveolar macrophages [25,26]. Moreover, there are evidences of stimulation of CRP production by lipid per-oxidation and infection by cytomegalovirus that triggers a cascade of pro-inflammatory cytokines [3].
Work of Chang, et al. [27] showed that CRP does not bind to native LDL. Instead, the increase in reactive ox-ygen production leads to oxidation of LDL that triggers entrance of LDL in macrophages mediated by CRP. CRP binds to oxidized phosphatidylcholine present at the surface of LDL [27].
Healthy individuals have low plasma levels of CRP (< 0.5 mg/dL). However, during inflammatory process-es, serum concentration of this protein can rise one hundred to one thousand times. Its synthesis starts 4-6 hours after stimulation, duplicates every 8 hours and reaches a maximum after 50 hours (around 2 days). Its levels can reach 300 mg/dL in 48 hours. These charac-teristics make CRP a relevant clinical marker due to its stability, high sensitivity, good reproductivity and preci-sion. This protein has a plasma half-life of 19 hours even after stimulus, trauma or surgery. It can take several days until it reaches basal levels [28,29]. In the absence of chronic stimulus, CRP levels normalize in 3-4 days. On the other hand, in chronic inflammatory states, CRP concentrations can remain high forever [28].
It has also been observed a correlation between CRP genetic variants and its plasma levels. Michopoulos, et al. [30] saw increased CRP plasma levels associated with the presence of the rs1130864 CRP polymorphism. Moreover, Markt, et al. [31] detected mean CRP levels significantly elevated in men with one copy of the vari-ant alleles rs3093075 and rs1417938 compared to those with no copies. On the other hand, the same study ob-served that men with one copy of the variant allele rs1800947 had significantly lower mean CRP levels. The rs2808630 polymorphism was not associated with cir-culating CRP [31].
CRP plasma concentration differs between individu-als. Each person has its own basal level that remains sta-ble over the years without big changes during the day or season. Diet does not interfere with CRP levels as well. However, these values tend to increase slightly with age in healthy individuals, probably due to the development of diseases still in the sub-clinical stages [29].
Table 1: Risk degree in the development of cardiovascular
problems related to serum levels of hs-CRP [1].
Risk degree hs-CRP concentration (mg/L)
Low risk < 1 Intermediate risk 1-3 High risk > 3
Nitric oxide produced by endothelial cells has an es-sential role in blood vessels relaxation, being strategical-ly linked to the endothelial cell membrane. Moreover, NO contradicts vascular smooth muscle contraction and inhibits platelet activation. It also acts on integrins, by modifying leucocyte adhesion and neutrophil diape-deses [44]. NO is continuously released from vascular endothelium, being responsible for the maintenance of tissues blood flow and for tissue extravasation control [45].
Therefore, all described processes are limited when CRP plasma levels are high [29]. By inhibiting NO pro-duction, CRP contributes to apoptosis of endothelial cells and consequently to pro-atherogenic and pro-in-flammatory events (Figure 1) [46].
Additionally, CRP not only controls the expression of adhesion molecules, like ICAM-1 and VCAM-1, through chemokine MCP-1, but also facilitates entrance of LDL, by opsonization, in macrophages [29,47]. Moreover, it has the power to induce oxidation of that cholesterol, contributing for the development of atherosclerosis. CRP is also involved in destabilization of atheroma fi-brous layer, by stimulating Matrix Methaloproteinase-1 (MMP-1), released with collagen and proteins degrada-tion. This destabilization occurs equally by the decrease in concentration of Plasminogen Activator (tPA), respon-sible for clot lysis in vascular wall, and for the increase in the level of Plasminogen Activator Inhibitor (PAI-1), that inhibits fibrinolysis. This process facilitates thrombi formation in endothelial wall, increasing the risk of car-diovascular events [48,49] (Figure 2).
Therefore, CRP is not only an inflammatory marker of atherosclerosis and coronary events, but also a CVD cardiac disease, or in individuals with atherosclerosis
risk [38]. In 2003, Ishikawa, et al. [39] concluded that CRP is located inside the atherosclerotic plaque, having an important role in plaque vulnerability. In the same way Inoue, et al. [24] in 2005, showed that CRP is pro-duced in the atherosclerotic plaque responsible for acute coronary syndrome, demonstrating the existence of a CRP gradient in coronary arterial circulation close and far away from the plaque.
CRP as risk factor
Evidences suggest that CRP is not only an inflamma-tory marker, but also participates actively in the ath-erosclerosis process [40]. Its levels correlate directly with several cardiovascular risk factors, like body mass index, smoking, systolic arterial pressure, serum levels of triglycerides and total cholesterol, cardiac frequency, fasting glycaemia and cardiovascular disease or stroke history and in an inverse way with HDL levels, both in children and in adults [41,42].
By its interaction with classic risk factors, CRP can lead to changes in the pro-atherosclerotic profile of pa-tients [43]. This protein has direct influence in athero-sclerotic vessels through the activation of the comple-ment system, closely related with the initial stages of atherosclerotic plaque formation, and with the stimulus of tissue factor synthesis by monocytes (procoagulant effect), and consequently, in promotion of inflamma-tion and thrombosis [10].
CRP favours the development of a pro-inflammatory state, through reduction of endothelial Nitric Oxide Syn-thase Activity (eNOS) [29], as well as reduction of tran-scription of eNOS coding genein endothelial cells [29].
↑ IL-6
↑ CRP
↑Plasminogen activator inhibitor
↓Plasminogen activator
↓eNOS
↑ Adhesion molecules ↓Fibrinolysis
↑ Cardiovascular events
Described data show that the use of statins in prima-ry prevention of CVD leads to a decrease in CVD mortal-ity. It was also seen the decrease of coronary events in groups with different characteristics of the population under study [54].
According with guidelines concerning “Emerging bio-markers for primary prevention of cardiovascular dis-ease” from the National Academy of Clinical
Biochem-istry Laboratory [55], hs-CRP cannot be determined in general population to evaluate cardiovascular risk. However, it can be used to stratify cardiovascular risk in adults with intermediate risk of coronary disease, and can help the decision about statins use in primary pre-vention [11].
CRP in secondary prevention
The objectives of secondary prevention are focused in avoiding a new cardiovascular event and identify the progression of myocardium dysfunction, leading to a reduction of mortality rate due to these diseases. To achieve these goals, secondary prevention includes changes in lifestyle and continuous use of medicines [56].
For hypertensive patients it is essential smoking ces-sation, weight loss, decrease of cholesterol serum levels and practice of physical exercise. Moreover, the con-tinuous use of aspirin, β-blockers, inhibitors of the an-giotensin I conversion enzyme, and in women in meno-pause, hormone replacement are also essential [56].
Several studies have shown the value of CRP in sec-ondary prevention of CVDs. The FRISC study [57] per-formed in 917 patients with acute coronary syndrome showed that hs-CRP has independent capacity of car-diovascular mortality prediction. Another randomized prospective study in 391 patients having non-fatal/fatal acute myocardial infarction (CARE study [36]), proved that the use of pravastatin leads to risk reduction of cor-mediator due to its contribution for the lesion process,
for plaque break and incoronary thrombosis mecha-nisms [29,46]. However, more research is needed to be able to conclude about the effects of CRP as a risk factor of CVD and its clinical relevance [47].
CRP in primary prevention
Due to the relationship between high CRP plasma levels and cardiovascular mortality and morbidity risk [11], it is important to establish a primary care line to decrease CVDs. For this, it is essential the evaluation of cardiovascular risk factors to stop their progression.
Several prospective studies having CRP as central target, have shown the benefits of primary prevention. In 1999, the MONICA-Augsburg study [50] performed in a sample of 936 asymptomatic men, concluded that the increase of hs-CRP leads to a 19% increased risk of fatal and non-fatal coronary events.
In the same way, the PREVEND study in 8139 as-ymptomatic men and women observed a relationship between hs-CRP and angiographic characteristics and consequently clinical instability of the atherosclerotic plaque [51]. The use of lovastatin in the treatment of 5742 individuals (AFCAPS/TexCAPS study) reduced the occurrence of the first coronary event both in individu-als with high cholesterol levels, and in the ones having high hs-CRP levels, even with low lipid profile [52].
The PRINCE study [53] performed with 1702 asymp-tomatic men and women showed that pravastatin re-duces hs-CRP levels in individuals without previous his-tory of CVD, independently of cholesterol levels.
Rosuvastatin was tested in 1802 asymptomatic men and women (having cholesterol LDL < 130 mg/dL and
hs-CRP > 2 mg/L) in the JUPITER study [54]. It was ob-served a reduction of 50% in LDL levels and 37% in hs-CRP levels, consequently reducing cardiovascular events in these apparently healthy individuals.
Inflammatory cellsin vascular wall and pro-inflammatory cytokines CRP Liver Endothelial cell Monocyte/macrophage Smoothmusclecell
Stimulates prolife ration and migration of smooth muscle cells Increase of free radicals
↓ NO release
↑ Expression of ICAM-I and VCAM-1 ↑ PAI-1
↑ Entrance of LDL-cholesterol
↑ Expression of cytokines (IL-6, TNF and IL-1) ↑ Expression of tecidular factor
↑ PAI-1
Figure 2: CRP role in stimulation of endothelial cells, mononuclear cells (monocytes and macrophages) and smooth muscle
and collaborators [34] published the first study that demonstrated the effect on reduction of cardiovascular events, because of therapy with acetylsalicylic acid, to-gether with serum CRP levels reduction [34]. This study showed that a dose of aspirin per day contributes to a 44% decrease in myocardial infarction risk. Patients having higher CRP levels showed higher risk decrease [34]. In the same way, a 75 mg per day dosage during a month led to a meaningful reduction in plasma CRP [61]. On the other hand, other studies demonstrated the ineffectiveness of aspirin relative to CRP levels [62]. Cyclooxygenase-2 Inhibitors (COX-2) (rofecoxib, cele-coxib) were also tested for their ability to reduce CRP levels. Some studies observed a decrease on serum CRP levels, when used alone or in combination with statins or aspirin [63,64].
In the same way, Lincoff, et al. [65] tested the effect of clopidogrel, an antiplatelet agent, on CRP levels and observed a 32% reduction [65].
Besides the anti-inflammatory effects on atheroscle-rotic tissues, statins also lead to reduction in CRP lev-els [53]. Riesen, et al. [66] observed beneficial effects on plasma CRP reduction. In this study, it was observed that therapy with high dosage of statins or its combi-nation with COX-2 inhibitors, given before an invasive coronary procedure in patients with unstable angina, rapidly decreased CRP serum levels [66].
There are, in fact, numerous studies showing the power of statins in reducing hs-CRP levels, that ob-served a reduction of 13 to 50% in its plasma levels [67
-70]. This was observed in patients with obesity [68], di-abetes [70], dyslipidemias [67,68] and coronary artery disease [69]. This statin associated with hs-CRP levels reduction results in a bigger clinical benefit in the treat-ment of patients having atrial fibrillation [71].
Another lipid lowering agent, ezetimibe, an inhibitor of cholesterol absorption, was tested in combination with statins [67]. This study observed a 41% reduction in CRP plasma levels when using the combined treatment onary events, mainly in individuals with inflammation
evidence determined by hs-CRP, not related with lipid levels.
Intensive therapy with a statin applied to 3745 pa-tients with acute coronary syndrome (PROVE-IT study [58]) could reduce hs-CRP levels below 2 mg/L, conse-quently decreasing the risk of acute myocardial infarc-tion or fatal coronary events, independently on the re-duction of LDL levels.
The PEACE study [59] (with 3771 individuals having-stable coronary disease) allowed to associate plasma
hs-CRP levels above 1 mg/L, to higher mortality risk due
to cardiovascular disease, acute myocardial infarction or stroke.
Since the inflammatory process is an integral part of atherosclerosis evolution, the use of a biomarker like CRP, becomes quite useful in combination with the con-trol of classic risk factors like lipid levels, change of eat-ing habits, weight loss associated with regular physical activity, control of glycaemic levels and smoking cessa-tion. The interconnection of these factors are strategies for reduction of cardiovascular events in primary and secondary prevention [29,47].
Therapy for high levels of CRP
Knowing that CRP is involved in CVD pathophysiolo-gy, it is expected that reduction of CRP levels prevents the development of the disorder and its complications. Data suggests that certain drugs can reduce CRP levels, however, the clinical relevance of these interventions is not known [60].
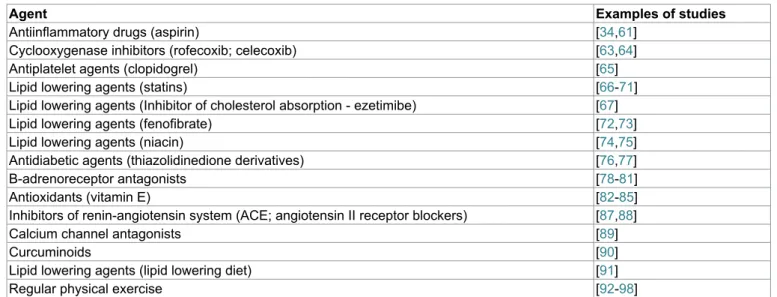
Prevention of cardiovascular events in individuals with high CRP levels can be achieved using CRP lowering agents. Table 2 summarizes the main studied agents/ strategies that contribute to reduction of plasma CRP.
Aspirin has the capacity of reducing the risk offu-ture cardiovascular events due to its antiplatelet and anti-inflammatory properties [47,60]. In 1997, Ridker
Table 2: CRP lowering agents.
Agent Examples of studies
Antiinflammatory drugs (aspirin) [34,61] Cyclooxygenase inhibitors (rofecoxib; celecoxib) [63,64] Antiplatelet agents (clopidogrel) [65] Lipid lowering agents (statins) [66-71] Lipid lowering agents (Inhibitor of cholesterol absorption - ezetimibe) [67] Lipid lowering agents (fenofibrate) [72,73] Lipid lowering agents (niacin) [74,75] Antidiabetic agents (thiazolidinedione derivatives) [76,77] Β-adrenoreceptor antagonists [78-81] Antioxidants (vitamin E) [82-85] Inhibitors of renin-angiotensin system (ACE; angiotensin II receptor blockers) [87,88] Calcium channel antagonists [89]
Curcuminoids [90]
Lipid lowering agents (lipid lowering diet) [91] Regular physical exercise [92-98]
sedentary adults. This studydid not show significative reductions of CRP and IL-6 after aerobic training, how-ever, reductions of CRP plasma levels were observed in response to resistance training [98]. Smith and co-work-ers [99] have shown that long term physical exercise can strongly reduce plasma levels of inflammatory cy-tokines and CRP. This anti-inflammatory effect demon-strates the benefits of physical activity in cardiovascular disease prevention [99].
Shortcomes on the use of CRP
As mentioned previously, CRP has a long half-life (around 19 hours), reaching its basal levels after several days. Indeed, the prognostic value and the evolution of the treatment in an initial phase might not be the most correct, making it a limitation on its use. Moreover, CRP takes 4-6 hours to be produced, after stimulus. So, its detection might not be fast enough to detect a cardio-vascular event [28].
CRP is an unspecific marker of acute phase response and increases of its plasma levels are expected not only in inflammation, but also in other clinical situations like infection and necrosis [100,101]. In this way, it is im-portant to say that CRP like any other marker, cannot be used alone in diagnosis or monitorization of therapeutic response.
Conclusion
CVDs are the main cause of incapacity and prema-ture death in the whole world. In these circulatory dis-eases, atherosclerosis is the basis for their progression. However, CVD development does not depend on one factor alone, but on the association of several risk fac-tors, resulting in a synergetic and multiplicative effect. With the high prevalence of risk factors for CVD in the general population, it becomes essential to give special attention to their prevention, detection and correction.
CVD prevention should start during childhood and adolescence with the adoption of healthy habits, since these will be used in adult life. Risk of CVD development can be detected using biomarkers that have been rele-vant in diagnosis, prognosis and as a therapeutic guide for these disorders. Biomarkers constitute a biologi-cal-qualitative and quantitative parameter of physiolog-ical changes or pathologphysiolog-ical processes.
Among biomarkers, CRP, an inflammatory marker, is considered to have bigger clinical relevanceand higher additional prognostic information, being independent of traditional risk factors. Moreover, CRP is an inflam-matory mediator in cardiovascular events.
CRP production, together with the increase of other pro-inflammatory cytokines starts during the first stage of the inflammatory process. This shows its role as a risk marker in this process. Moreover, CRP leads to instabil-ity of vascular endothelium by reducing NO production, induces LDL oxidation by facilitating LDL entrance in the [67]. Fenofibrate, usually used in the treatment of
hy-pertriglyceridemia also led to CRP reduction, being ob-served a decrease between 74-84% [72,73]. In the same way, treatment of dyslipidemias with a combination of niacin/statin, allowed a 24% reduction of CRP [74,75]. The effect of niacin alone was not tested in these stud-ies.
Some antidiabetic agents can also have beneficial effects on CRP levels. A 40% reduction of CRP levels, after treatment with thiazolidinedione derivatives, was observed in type 2 diabetes mellitus patients [76] and in nondiabetic hypertensive patients [77]. Moreover, β-adrenoreceptor antagonists, normally use in the treatment of hypertension and coronary artery disease, led to reduction of CRP levels ranging between 36-73%, depending on the type of antagonist used [78-81].
The use of antioxidants has also been shown to con-tribute to CRP reduction. Several studies observed de-creased plasma CRP levels when using vitamin E, rang-ing from 49 to 81% [82-85], but no effect was seen by vitamin C [86].
Another group of drugs known to have effect on CRP plasma levels are the inhibitors of Renin-Angiotensin system. Angiotensin converting enzyme inhibitors and angiotensin II receptor blockers were tested and both led to decrease in CRP levels [87,88].
Some calcium channel antagonists can also lead to plasma CRP reduction. This was observed in the study of Hung, et al. [89] where these agents were used in the treatment of patients with vasospastic coronary artery disease.
The use of herbal extracts like curcuminoids, multi-functional natural products with promising cardiopro-tective and anti-inflammatory properties, has also been tested. Sahebkar [90] observed a significant decrease of CRP plasma levels in a group of 172 individuals.
Moreover, obesity, tobacco, and lack of physical activity are factors associated with high levels of CRP, and therefore changes in lifestyle also contribute to the intended reduction [10,47]. One example is the use of lipid lowering diets tested by Jenkins, et al. [91], who observed a 10-28% decrease in serum levels of that pro-tein, depending on the type of diet used.
Lack of physical activity during childhood and ad-olescence is a risk factor with big significance for CVD [92]. Regular physical exercise is associated with poten-tial benefits for health, being considered essenpoten-tial for proper growth and development [93]. Data proved that regular physical activity is inversely associated with high levels of different inflammatory markers [94-96]. It has also been observed that the type, duration and intensity of physical activity are crucial factors for the profile of cytokine response after exercise [97]. A study of Dong-es, et al. [98] evaluated changes of IL-6 and CRP after 10 weeks of resistance and aerobic physical exercise in
7. Durand P, Prost M, Loreau N, Lussier-Cacan S, Blache D (2001) Impaired homocysteine metabolism and athero-thrombotic disease. Lab Invest 81: 645-672.
8. Nygård O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, et al. (1997) Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med 337: 230-236.
9. Lowe GD, Yarnell JW, Rumley A, Bainton D, Sweetnam PM (2001) C-reactive protein, fibrin D-dimer, and incident isch-emic heart disease in the Speedwell study: Are inflamma-tion and fibrin turnover linked in pathogenesis? Arterioscler Thromb Vasc Biol 21: 603-610.
10. Lagrand WK, Visser CA, Hermens WT, Niessen HW, Ver-heugt FW, et al. (1999) C-reactive protein as a cardiovas-cular risk factor: More than an epiphenomenon? Circulation 100: 96-102.
11. Silva D, Lacerda AP (2012) Proteína C reativa de alta sen-sibilidade como biomarcador de risco na doença coronária. Revista Portuguesa de Cardiologia 31: 733-745.
12. Villacorta H, Masetto AC, Mesquita ET (2006) C-reactive protein: inflammatory marker with prognostic value in pa-tients with decompensated heart failure. Archives of Cardi-ology 88: 585-589.
13. Koenig W, Khuseyinova N (2007) Biomarkers of athero-sclerotic plaque instability and rupture. Arterioscler Thromb Vasc Biol 27: 15-26.
14. Berezin AE, Lisovaya OA (2014) C-reactive protein after stroke in arterial hypertension. Asian Cardiovasc Thorac Ann 22: 551-557.
15. Libby P (1995) Molecular bases of the acute coronary syn-dromes. Circulation 91: 2844-2850.
16. Gottlieb MGV, Bonardi G, Moriguchi EH (2005) Fisiopa-tologia e aspetos inflamatórios da aterosclerose. Scientia Medica 15: 203-207.
17. Librandi AP, Pandochi AI (2008) O envolvimento do siste-ma de complemento nos processos de aterogénese. Me-dicina 41: 312-326.
18. Marnell L, Mold C, Du Clos TW (2005) C-reactive protein: Ligands, receptors and role in inflammation. Clin Immunol 117: 104-111.
19. Dongyuan Xia, David Samols (1997) Transgenic mice ex-pressing rabbit C-reactive protein are resistant to endotox-emia. Proc Natl Acad Sci U S A 94: 2575-2580.
20. Thompson D, Pepys MB, Wood SP (1999) The physiolog-ical structure of human C-reactive protein and its complex with phosphocholine. Structure 7: 169-177.
21. Stone PA, Kazil J (2014) The relationships between serum C-reactive protein level and risk and progression of coro-nary and carotid atherosclerosis. Semin Vasc Surg 27: 138-142.
22. Jialal I, Devaraj S (2001) Inflammation and atherosclerosis: The value of the high-sensitivity C-reactive protein assay as a risk marker. Am J Clin Pathol 116: S108-S115.
23. Haverkate F, Thompson SG, Pyke SD, Gallimore JR, Pepys MB (1997) Production of C-reactive protein and risk of coronary events in stable and unstable angina. Europe-an concerted action on thrombosis Europe-and disabilities Europe-angina pectoris study group. Lancet 349: 462-466.
24. Inoue T, Kato T, Uchida T, Sakuma M, Nakajima A, et al. (2005) Local release of C-reactive protein from vulnerable plaque or coronary arterial wall injured by stenting. J Am
macrophage, and is involved in destabilization of the fi-brous layer of the atheroma. This destabilization occurs through the stimulus of matrix methaloproteinase-1, released with collagen and other proteins degradation, inducing thrombus formation in the endothelial wall and consequently increasing the risk of cardiovascular events.
So, CRP measured by high sensitivity methods in in-dividuals having apparent cardiovascular risk, should be seen not only as an inflammation marker but also as a possible risk factor for CVDs.
High CRP levels can be reduced by the use of several strategies that go from changes in daily habits to the use of several drugs that directly interfere with CRP serum concentration.
In conclusion, the prevalence of high risk individuals for the progression of CVD, points out for the need of strategies with coordinate intervention of several health experts. These strategies should involve prevention, de-tection and effective treatment of cardiovascular risk factors, contributing in this way to the risk reduction in the population.
It is important the adoption of measures in the pop-ulation, that potentiate the reduction of the risk of de-veloping this type of disorders, the application of a fast and adequate treatment and the use of secondary pre-vention measures that will reduce their return.
The Authors declare that there is no conflict of in-terest.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
1. DL Cozlea, DM Farcas, A Nagy, AA Keresztesi, Ramona Tifrea, et al. (2013) The impact of C-reactive protein on global cardiovascular risk on patients with coronary artery disease. Curr Health Sci J 39: 225-231.
2. Sobrinho CAA, Moreira CM, Mota JA, Santos RMR (2015) Proteína C reativa, atividade física e aptidão cardiorrespi-ratória em adolescentes portugueses: Um estudo transver-sal. Cadernos de Saúde Pública 31: 1907-1915.
3. Hajsadeghi S, Chitsazan M, Chitsazan M, Salehi N, Amin A, et al. (2015) Changes of high sensitivity C-reactive pro-tein during clopidogrel therapy in patients undergoing per-cutaneous coronary intervention. Res Cardiovasc Med 5: e28997.
4. Nakagami F, Nakagami H, Osako MK, Iwabayashi M, Tani-yama Y, et al. (2010) Estrogen attenuates vascular remod-eling in Lp(a) transgenic mice. Atherosclerosis 211: 41-47. 5. Taskinen MR (2005) Type 2 diabetes as a lipid disorder.
Curr Mol Med 5: 297-308.
6. Baños-González, Peña-Duque, Anglés-Cano E, Marti-nez-Rios, Bahena, et al. (2010) Apo(a) phenotyping and lon-term prognosis for coronary artery disease. Clin Bio-chem 43: 640-644.
41. Cook DG, Mendall MA, Whincup PH, Carey IM, Ballam L, et al. (2000) C-reactive protein concentration in children: Re-lationship to adiposity and other cardiovascular risk factors. Atherosclerosis 149: 139-150.
42. Wu SL, Li JF, Li Y, Jin C, Wang LY, et al. (2010) The distri-bution and influential factors of serum high sensitivity C-re-active protein in general population. Zhonghua Nei Ke Za Zhi 49: 1010-1014.
43. Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, et al. (2006) Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med 355: 2631-2639.
44. Furchgott RF, Cherry PD, Zawadzki JV, Jothianandan D (1984) Endothelial cells as mediators of vasodilation of ar-teries. J Cardiovasc Pharmacol 6: S336-S343.
45. Flora Filho R, Zilberstein B (2000) Óxido nítrico: o simples mensageiro percorrendo a complexidade. Metabolismo, síntese e funções. Revista da Associação Médica Brasile-ira 46: 265-271.
46. Teixeira BC, Lopes AL, Macedo RCO, Cleiton SC, Thiago RR, et al. (2014) Marcadores inflamatórios, função endo-telial e riscos cardiovasculares. J Vasc Bras 13: 108-115. 47. Blake GJ, Ridker PM (2003) C-reactive protein: a surrogate
risk marker or mediator of atherothrombosis? Am J Physiol Regul Integr Comp Physiol 285: 1250-1252.
48. Singh U, Devaraj S, Jialal I (2005) C-reactive protein de-creases tissue plasminogen activator activity in human aortic endothelial cells: Evidence that C-reactive protein is a procoagulant. Arterioscler Thromb Vasc Biol 25: 2216-2221.
49. Volp AC, Alfenas RC, Costa NM, MinimI VPR, Stringue-ta CP, et al. (2008) Capacidade dos biomarcadores in-flamatórios em predizer a síndrome metabólica. Arq Bras Endocrinol Metab 52: 537-549.
50. Koenig W, Sund M, Fröhlich M, Fischer HG, Löwel H, et al. (1999) C-reactive protein, a sensitive marker of inflam-mation, predicts future risk of coronary heart disease in ini-tially healthy middle-aged men: Results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort study, 1984 to 1992. Circulation 99: 237-242.
51. Geluk CA, Post WJ, Hillege HL, Tio RA, Tijssen JG, et al. (2008) C-reactive protein and angiographic characteristics of stable and unstable coronary artery disease: Data from the prospective PREVEND cohort. Atherosclerosis 196: 372-382.
52. Ridker PM, Rifai N, Clearfield M, Downs JR, Weis SE, et al. (2001) Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events. N Engl J Med 344: 1959-1965.
53. Albert MA, Danielson E, Rifai N, Ridker PM, PRINCE In-vestigators (2001) Effect of statin therapy on C-reactive protein levels: The pravastatin inflammation/CRP evalua-tion (PRINCE): A randomized trial and cohort study. JAMA 286: 64-70.
54. Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, et al. (2008) Resuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 359: 2195-2207.
55. Christenson RH, Azzazy HM (2009) Cardiac point of care testing: A focused review of current National Academy of Clinical Biochemistry guidelines and measurement plat-forms. Clin Biochem 42: 150-157.
Coll Cardiol 46: 239-245.
25. Calabro P, Willerson JT, Yeh ET (2003) Inflammatory cy-tokines stimulated C-reactive protein production by human coronary artery smooth muscle cells. Circulation 108: 1930-1932.
26. Dong Q, Wright JR (1996) Expression of C-reactive protein by alveolar macrophages. J Immunol 156: 4815-4820. 27. Mi-Kyung Chang, Christoph J Binder, Michael Torzewski,
Joseph L Witztum (2002) C-reactive protein binds to both oxidized LDL and apoptotic cells through recognition of a common ligand: Phosphorylcholine of oxidized phospholip-ids. Proc Natl Acad Sci U S A 99: 13043-13048.
28. Bezerra CFR, Amaral BA, Camelo FP, Ana RLA, Eduardo GS, et al. (2008) O papel da proteína C-reativa na relação entre as doenças periodontais e cardiovasculares. R Peri-odontia 18: 7-13.
29. Denardi CAS, Filho AC, Chagas ACP (2008) A Proteína C-reativa na atualidade. Rev SOCERJ 2: 329-334.
30. Vasiliki Michopoulos, Alex O Rothbaum, Tanja Jovanovic, Lynn M Almli, Bekh Bradley, et al. (2015) CRP genetic vari-ation and CRP levels are associated with increased PTSD symptoms and physiological responses in a highly trauma-tized civilian population. Am J Psychiatry 172: 353-362. 31. Markt SC, Rider JR, Penney KL, Schumacher FR, Epstein
MM, et al. (2014) Genetic variation across C-reactive pro-tein and risk of prostate cancer. Prostate 74: 1034-1042. 32. Lima JCC, Correia LCL, Silva AM (2000) Proteína C reativa
de alta sensibilidade como biomarcador de risco na doença coronária. Newslab 41: 164-166.
33. Ridker PM, Hennekens CH, Buring JE, Rifai N (2000) C-re-active protein and other markers of inflammation in the pre-diction of cardiovascular disease in women. N Engl J Med 342: 836-843.
34. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennek-ens CH (1997) Inflammation, aspirin, and the risk of cardio-vascular disease in apparently healthy men. N Engl J Med 336: 973-979.
35. Kuller LH, Tracy RP, Shaten J, Meilahn EN (1996) Rela-tion of C-reactive protein and coronary heart disease in the MRFIT nested case-control study. Multiple risk factor intervention trial. American Journal of Epidemiology 144: 537-547.
36. Ridker PM, Glynn RJ, Hennekens CH (1998) C-reactive protein adds to the predictive value of total and HDL cho-lesterol in determining risk of first myocardial infarction. Cir-culation 97: 2007-2011.
37. Hashimoto H, Kitagawa K, Hougaku H, Shimizu Y, Saka-guchi M, et al. (2001) C-reactive protein is an independent predictor of the rate of increase in early carotid atheroscle-rosis. Circulation 104: 63-67.
38. Scirica BM, Morrow DA, Cannon CP, de Lemos JA, Mur-phy S, et al. (2007) Clinical application of C-reactive protein across the spectrum of acute coronary syndromes. Clin Chem 53: 1800-1807.
39. Ishikawa T, Hatakeyama K, Imamura T, Date H, Shibata Y, et al. (2003) Involvement of C-reactive protein obtained by directional coronary atherectomy in plaque instability and developing restenosis in patients with stable or unstable angina pectoris. Am J Cardiol 91: 287-292.
40. Li SH, Szmitko PE, Weisel RD, Wang CH, Fedak PW, et al. (2004) C-reactive protein upregulates complement-inhibito-ry factors in endothelial cells. Circulation 109: 833-836.
71. Abaci O, Kocas C, Oktay V, Yildiz CE, Kilickesmez KO, et al. (2013) Comparison of rosuvastatina versus atorvastatin for preventing postoperative atrial fibrillation. Heart Surg Forum 16: E158-E161.
72. Coban E, Sari R (2004) The effect of fenofibrate on the levels of high sensitivity C-reactive protein in dyslipidemic obese patients. Endocr Res 30: 343-349.
73. Yesilbursa D, Serdar A, Saltan Y, Serdar Z, Heper Y, et al. (2005) The effect of fenofibrate on serum paraoxonase ac-tivity and inflammatory markers in patients with combined hyperlipidemia. Kardiol Pol 62: 526-530.
74. Kashyap ML, McGovern ME, Berra K, Guyton JR, Kwiterovich PO, et al. (2002) Long-term safety and effica-cy of a once-daily niacin/lovastatin formulation for patients with dyslipidemia. Am J Cardiol 89: 672-678.
75. Moon YS, Kashyap ML (2002) Niacin extended-release/ lovastatin: Combination therapy for lipid disorders. Expert Opin Pharmacother 3: 1763-1771.
76. Haffner SM, Greenberg AS, Weston WM, Chen H, Williams K, et al. (2002) Effect of rosiglitazone treatment on nontra-ditional markers of cardiovascular disease in patients with type 2 diabetes mellitus. Circulation 106: 679-684.
77. Raji A, Seely EW, Bekins SA, Williams GH, Simonson DC, et al. (2003) Rosiglitazone improves insulin sensitivity and lowers blood pressure in hypertensive patients. Diabetes Care 26: 172-178.
78. Anzai T, Yoshikawa T, Takahashi T, Maekawa Y, Okabe T, et al. (2003) Early use of beta-blockers is associated with attenuation of serum C-reactive protein elevation and favor-able short-term prognosis after acute myocardial infarction. Cardiology 99: 47-53.
79. Jenkins NP, Keevil BG, Hutchinson IV, Brooks NH (2002) Beta-blockers are associated with lower C-reactive protein concentrations in patients with coronary artery disease. Am J Med 112: 269-274.
80. Joynt KE, Gattis WA, Hasselblad V, Fuzaylov SY, Sere-bruany VL, et al. (2004) Effect of angiotensin-converting enzyme inhibitors, beta-blockers, statins, and aspirin on C-reactive protein levels in outpatients with heart failure. Am J Cardiol 93: 783-785.
81. Yasunari K, Maeda K, Nakamura M, Watanabe T, Yoshika-wa J, et al. (2004) Effects of carvedilol on oxidative stress in polymorphonuclear and mononuclear cells in patients with essential hypertension. Am J Med 116: 460-465.
82. Devaraj S, Jialal I (2000) Alpha-tocopherol supplementa-tion decreases serum C-reactive protein and monocyte in-terleukin-6 levels in normal volunteers and type 2 diabetic patients. Free Radic Biol Med 29: 790-792.
83. Murphy RT, Foley JB, Tome MT, Mulvihill NT, Murphy A, et al. (2004) Vitamin E modulation of C-reactive protein in smokers with acute coronary syndromes. Free Radic Biol Med 36: 959-965.
84. Somogyi A, Herold M, Kocsis I, Nagy G, Somfai G, et al. (2005) Effect of vitamin E supplementation on the vitamin content of lipoprotein in young men and woman. Orv Hetil 146: 1813-1818.
85. Upritchard JE, Sutherland WH, Mann JI (2000) Effect of supplementation with tomato juice, vitamin E and vitamin C on LDL oxidation and products of inflammatory activity in type 2 diabetes. Diabetes Care 23: 733-738.
86. Fumeron C, Nguyen-Khoa T, Saltiel C, Kebede M, Buisson C, et al. (2005) Effects of oral vitamin C supplementation on 56. Jardim CV, Titan SM, Pereira AC, Lotufo PA (1999)
Pre-venção secundária da doença coronária em pacientes hip-ertensos. Hiper Ativo 6: 51-56.
57. Lindahl B, Toss H, Siegbahn A, Venge P, Wallentin L (2000) Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. FRISC Study Group. Fragmin during Instability in Coronary Artery Disease. N Engl J Med 343: 1139-1147.
58. Ridker PM, Morrow DA, Rose LM, Rifai N, Cannon CP, et al. (2005) Relative efficacy of atorvastatin 80 mg and pravastatin 40 mg in achieving the dual goals of low-densi-ty lipoprotein cholesterol < 70 mg/dl and C-reactive protein < 2 mg/l: An analysis of the PROVE-IT TIMI-22 trial. J Am Coll Cardiol 45: 1644-1648.
59. Sabatine MS, Morrow DA, Jablonski KA, Rice MM, Warnica JW, et al. (2007) Prognostic significance of the Centers for Disease Control/American Heart Association high-sensitivi-ty C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation 115: 1528-1536.
60. Prasad K (2006) C-reactive protein (CRP)-lowering agents. Cardiovasc Drug Rev 24: 33-50.
61. Woodward M, Lowe GD, Francis LM, Rumley A, Cobbe SM, et al. (2004) A randomized comparison of the effects of aspirin and clopidogrel on thrombotic risk factors and C-re-active protein following myocardial infarction: The CADET trial. J Thromb Haemost 2: 1934-1940.
62. Takeda T, Hoshida S, Nishino M, Tanouchi J, Otsu K, et al. (2003) Relationship between effects of statins, aspirin and angiotensin II modulators on high-sensitive C-reactive protein levels. Atherosclerosis 169: 155-158.
63. Kim SB, Kim SH, Chang JW, Lee SK, Min WK, et al. (2004) Effects of cebecoxib on high-sensitivity C-reactive protein in chronic peritoneal dialysis patients. Ren Fail 26: 381-384. 64. Chyrchel M, Dudek D, Bartuś S, Legutko J, Heba G, et al.
(2004) High-dose statin and COX-2 inhibitor therapy rapidly decreases C-reactive protein level inpatients with unstable angina. Kardiologia Polska 61: 213-221.
65. Lincoff AM, Kereiakes DJ, Mascelli MA, Deckelbaum LI, Bar-nathan ES, et al. (2001) Abciximab suppresses the rise in levels of circulating inflammatory markers after percutaneous coronary revascularization. Circulation 104: 163-167.
66. Riesen WF, Engler H, Risch M, Korte W, Noseda G (2002) Short-term effects of atorvastatin on C-reactive protein. Eur Heart J 23: 794-799.
67. Ballantyne CM, Houri J, Notarbartolo A, Melani L, Lipka LJ, et al. (2003) Effect of ezetimibe coadministered with ator-vastatin in 628 patients with primary hypercholesterolemia. A prospective, randomized, double-blind trial. Circulation 107: 2409-2415.
68. Harold E Bays, Evan A Stein, Arvind K Shah, Darbie L Mac-cubbin, Yale B Mitchel, et al. (2002) Effects of simvastatin on C-reactive protein in mixed hyperlipidemic and hypertri-glyceridemic patients. The American Journal of Cardiology 90: 942-946.
69. Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, et al. (2005) Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med 352: 29-38.
70. van de Ree MA, Huisman MV, Princen HM, Meinders AE, Kluft C, et al. (2003) Strong decrease of high sensitivity C-reactive protein with high-dose atorvastatin in patients with type 2 diabetes mellitus. Atherosclerosis 166: 129-135.
94. Plaisance EP, Grandjean PW (2006) Physical activity and high-sensitivity C-reactive protein. Sports Med 36: 443-458. 95. Lavie CJ, Church TS, Milani RV, Earnest CP (2011) Impact
of physical activity, cardiorespiratory fitness, and exercise training on markers of inflammation. J Cardiopulm Rehabil Prev 31: 137-145.
96. Hamer M, Sabia S, Batty GD, Shipley MJ, Tabák AG, et al. (2012) Physical activity and inflammatory markers over 10 years: Follow-up in men and women from the Whitehall II cohort study. Circulation 126: 928-933.
97. Ferreira FC, de Medeiros AI, Nicioli C, Nunes JE, Shigue-moto GE, et al. (2009) Circuit resistance training in seden-tary women: Body composition and serum cytokine levels. Appl Physiol Nutr Metab 35: 23-29.
98. Donges CE, Duffield E, Drinkwater EJ (2010) Effects of re-sistance or aerobic exercise training on interleukin-6, C-re-active protein, and body composition. Med Sci Sports Exerc 42: 304-313.
99. Smith JK, Dykes R, Douglas JE, Krishnaswamy G, Berk S (1999) Long-term exercise and atherogenic activity of blood mononuclear cells in persons at risk of developing ischemic heart disease. JAMA 281: 1722-1727.
100. Gabay C, Kushner I (1999) Acute-phase proteins and oth-er systemic responses to inflammation. N Engl J Med 340: 448-454.
101. Young B, Gleeson M, Cripps AW (1991) C-reactive pro-tein: A critical review. Pathology 23: 118-124.
oxidative stress and inflammation status in haemodialysis patients. Nephrol Dial Transplant 20: 1874-1879.
87. Mitrovic V, Klein HH, Krekel N, Kreuzer J, Fichtlscherer S, et al. (2005) Influence of the angiotensin converting en-zyme inhibitor ramipril on high sensitivity C-reactive protein (hs-CRP) in patients with documented atherosclerosis. Z Kardiol 94: 336-342.
88. Yasunari K, Maeda K, Watanabe T, Nakamura M, Yoshikawa J, et al. (2004) Comparative effects of valsartan versus am-lodipine on left ventricular mass and reactive oxygen species formation by monocytes in hypertensive patients with left ven-tricular hypertrophy. J Am Coll Cardiol 43: 2116-2123. 89. Hung MJ, Cherng WJ, Cheng CW, Yang NI (2005) Effect of
antispastic agents (calcium antagonists and_or isosorbide di-nitrate) on high-sensitivity C-reactive protein in patients with coronary vasospastic angina pectoris and no hemodynamical-ly significant coronary artery disease. Am J Cardiol 95: 84-87. 90. Sahebkar A (2014) Are curcuminoids effective C-reactive
protein-lowering agents in clinical practice? Evidence from a meta-analysis. Phytother Res 28: 633-642.
91. Jenkins DJ, Kendall CW, Marchie A, Faulkner DA, Wong JM, et al. (2003) Effects of a dietary portfolio of cholester-ol-lowering foods vs. lovastatin on serum lipids and C-reac-tive protein. JAMA 290: 502-510.
92. Andersen LB, Riddoch C, Kriemler S, Hills AP (2011) Phys-ical activity and cardiovascular risk factors in children. Br J Sports Med 45: 871-876.
93. Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dish-man RK, et al. (2005) Evidence based physical activity for school-age youth. J Pediatr 146: 732-737.
![Figure 1: Cascade of changes induced by CRP that lead to cardiovascular events [46].](https://thumb-eu.123doks.com/thumbv2/123dok_br/18698115.915970/4.892.69.830.763.1167/figure-cascade-changes-induced-crp-lead-cardiovascular-events.webp)
![Figure 2: CRP role in stimulation of endothelial cells, mononuclear cells (monocytes and macrophages) and smooth muscle cells leading to the production of inflammatory mediators [49].](https://thumb-eu.123doks.com/thumbv2/123dok_br/18698115.915970/5.892.74.825.67.376/stimulation-endothelial-mononuclear-monocytes-macrophages-production-inflammatory-mediators.webp)