In CD, fistulas, strictures and abscesses may occur in more than half of patients (Cosnes et al. 2002). This is thought to be due to the development of colonoscopes and colonoscopic techniques (Axelrad et al. 2020).
Aetiology
Epidemiology
In the Nordic countries, the incidence rate for UC is higher than for CD (Molodecky et al. 2012). During the last decade, the incidence has also increased rapidly in Eastern Europe and Asia (Molodecky et al. 2012).
Clinical presentation
Crohn’s disease
Ulcerative colitis
Laboratory findings
Blood tests
ANCA positivity in CD has been associated with UC-like clinical and histological features (Vasiliauskas et al. 2000). ASCA positivity in CD has been associated with earlier disease onset, strictures and invasive small bowel disease (Vasiliauskas et al. 2000).
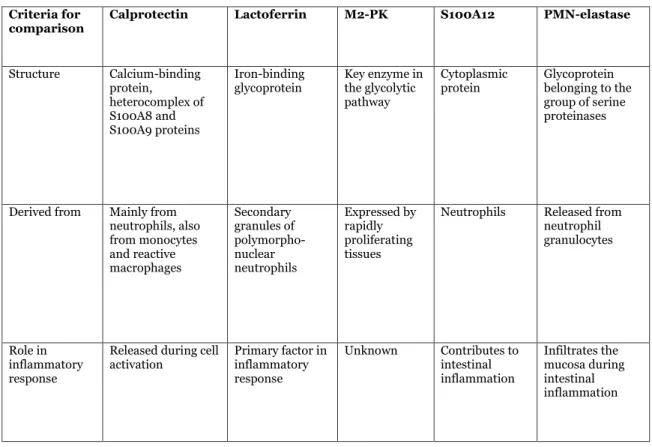
Faecal markers
- Faecal calprotectin in IBD
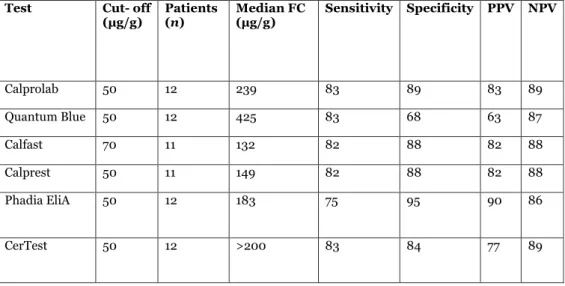
- Faecal calprotectin rapid tests
- Faecal lactoferrin
- Other faecal markers
First described in the 1980s (Roseth et al. 1992), calprotectin is the major cytosolic protein of neutrophil leukocytes. In patients with colonic IBD, FLf levels correlate with the extent of the disease (Rubio et al. 2019).
Endoscopy
Endoscopic indices
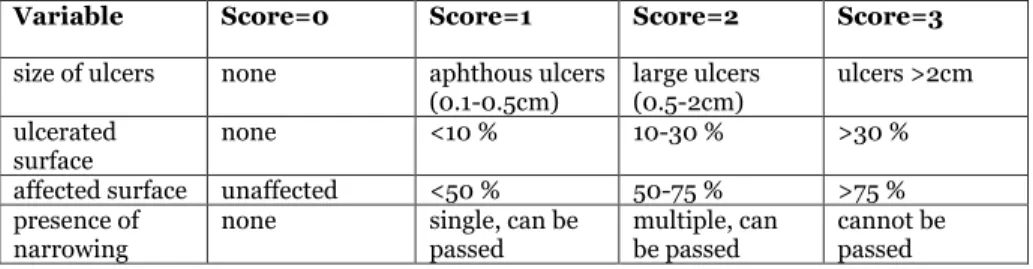
- Endoscopic indices in Crohn’s disease
- Endoscopic indices in ulcerative colitis
The Simple Endoscopic Crohn's Disease Score (SES-CD) was developed to simplify the endoscopic assessment of Crohn's disease compared to CDEIS (Daperno et al. 2004). In 2005, the modified Baron score (Feagan score), a 5-point scale that evaluates vascular pattern, friability, bleeding and ulceration, was developed (Feagan et al. 2005).
Histology
Due to the complexity of the score, a simplified Geboes score was developed (Jauregui-Amezaga et al. 2017). The European Crohn's Disease and Colitis Organization (ECCO) recommends the use of the Nancy histological index in clinical practice (Magro et al. 2017).
Imaging
PSC strongly increases the CRC risk in UC patients in most of the studies (Barner-Rasmussen et al. 2020). Controversially, in a large Finnish registry database study, PSC did not have an effect on the CRC risk (Nieminen et al. 2014).
Aetiology and pathogenesis
Also, changes and dysbiosis of the colonic microbiota can play a role in the development of CRC (Keller et al. 2019). Localized neoplasia occurs in about a quarter of the patients and is more often associated with late-onset IBD (Brackmann et al. 2009).
Epidemiology
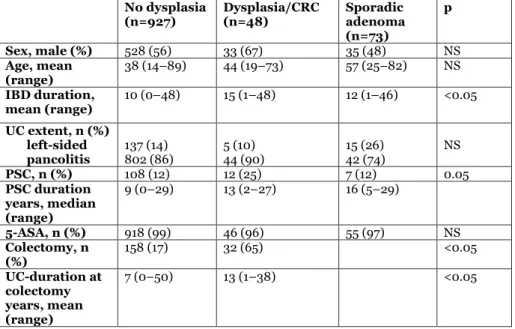
Dysplasia
The elevated FC concentration in CRC may also reflect the shedding of neutrophils from ulcerated tumor (Gilbert et al. 1996). The incidence of sporadic adenomas in IBD patients also increases with age, but the progression of sporadic adenoma to CRC is much slower than in colitis-associated dysplasia (Li et al. 2022). Adenoma-like lesions within the area of histologic colitis may be IBD-associated dysplasia, and close surveillance or colectomy is recommended (Li et al. 2022).
IBD-associated colorectal carcinoma
More than 50% of the unselected population will develop a sporadic adenoma by age 70, and approximately 10% of these will progress to cancer (Johns et al. 2001). Dysplastic polyps that do not arise in segments with macroscopic or histological inflammation are considered sporadic adenomas and can be managed accordingly (Magro et al. 2017). However, features referring to IBD-related dysplasia include young age at diagnosis, long duration of IBD, villous architecture, a mixture of normal and dysplastic epithelium on the polyp surface, increased inflammation in the polyp, and expression of p53 (Torres et al. 1998, Mueller et al. 1999).
Risk factors
Chemoprevention
Dysplasia surveillance
ACG: American College of Gastroenterology, ECCO: European Crohns and Colitis Organisation, ASGE: American Society of Gastrointestinal Endoscopy, BSG: British Society of Gastroenterology, CRC: kolorektalt carcinom, PSC: primær skleroserende cholangitis.
Faecal calprotectin in colorectal neoplasias
Colorectal carcinoma
Colorectal adenomas
Two-thirds of patients alternated between relapse remissions and 20% had continuous activity with relapse every year of follow-up (Burisch et al. 2013). Strictures are typical for ileal disease and penetrating complications for perianal disease (Cosnes et al. 2002, Solberg et al. 2007). A quarter of patients were in clinical remission in all years of follow-up, 18% had active disease in each year, and 57% had intermittent activity (Burisch et al. 2013).
Clinical indices
Clinical indices in Crohn’s disease
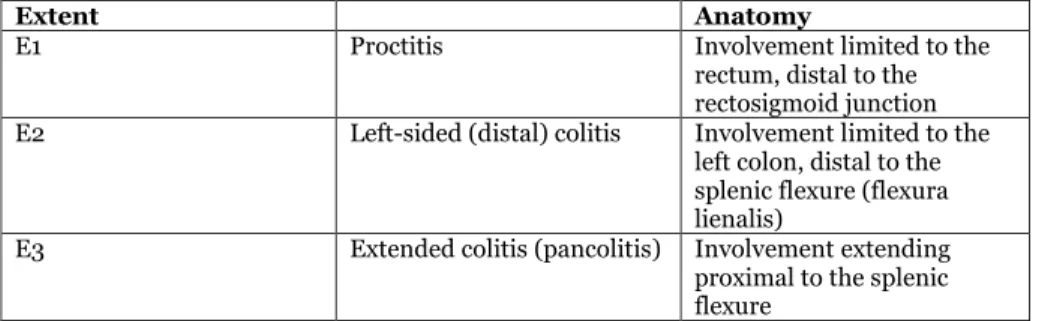
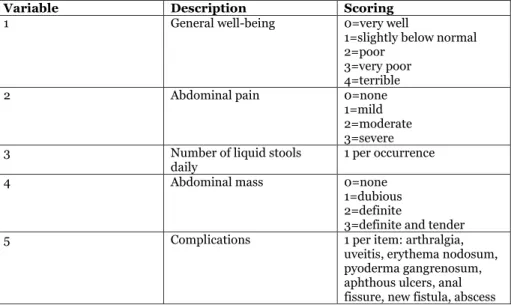
In about 30% of patients with proctitis, the disease progresses to left-sided or extensive colitis during follow-up (Henriksen et al. 2006). The variables selected for the short CDAI are abdominal pain, diarrhea frequency and general well-being (Thia et al. 2011). The Harvey-Bradshaw Index (HBI), developed in 1980, is a simplified index for the clinical evaluation of CD activity (Table 11) (Harvey et al. 1980).
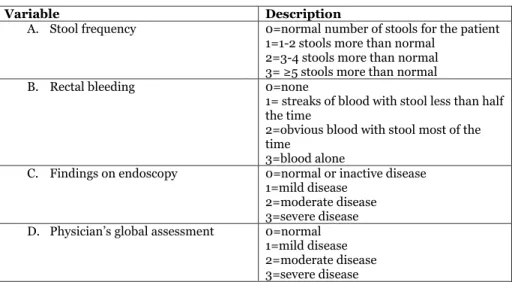
Clinical indices in ulcerative colitis
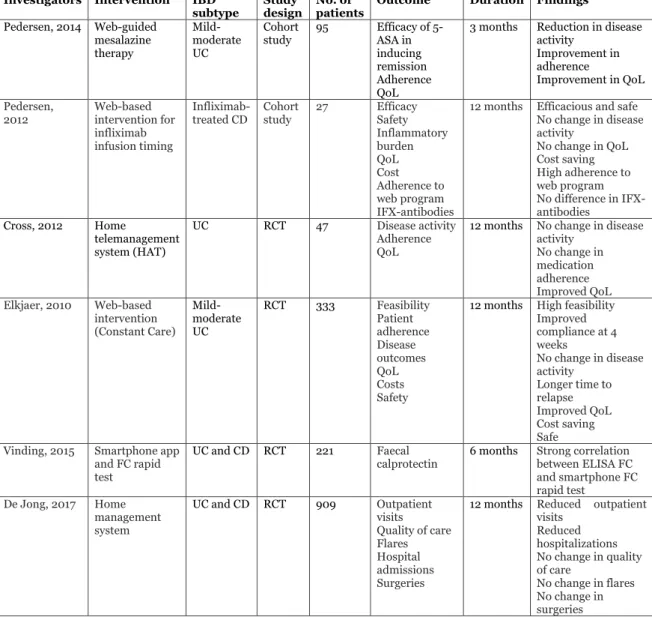
E-Health
E-Health in IBD
IBD is most often diagnosed at a young age and is associated with excessive use of health care resources (Jussila et al. 2013). Based on the positive results of monitoring other chronic conditions, e-health was also introduced in the care of patients with IBD (Aguas et al. 2016, Gaikwad et al. 2009). The first and ground-breaking home monitoring assessment of IBD patients was developed by the Cross group (Cross et al. 2015).
Medical treatment
Surgical treatment
The impact of IBD on the quality of life is due to variable disease course and the lack of definitive cure, and the psychological well-being is often impaired even in patients in remission (Simrén et al. 2002). Almost half of the patients reported that doctors do not ask about the impact of IBD on their quality of life (Ghosh et al. 2007, Mitchell et al. 2009). Health-related quality of life (HRQoL) is a subjective matter, and includes the physical, emotional and social components associated with disease or treatment.
Retrospective studies
Patients in Study I and II
Patients in all studies were recruited from the gastroenterology outpatient clinic at Helsinki University Hospital (Helsinki, Finland).
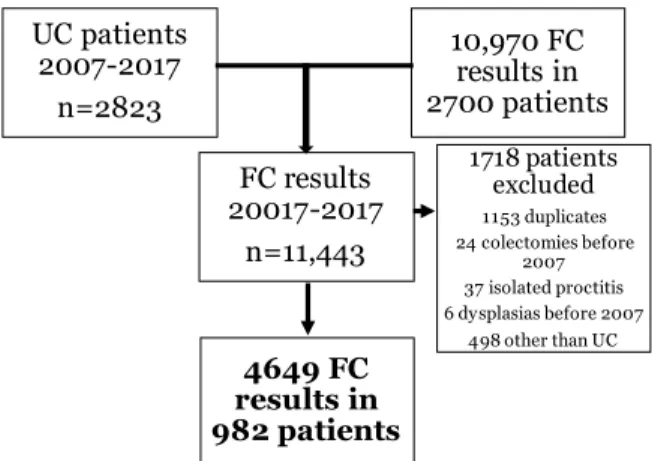
Patients in Study IV
IBD: Inflammatory bowel disease, UC: ulcerative colitis, PSC: Primary sclerosing cholangitis, CRC: colorectal carcinoma, FC: faecal calprotectin, 5-ASA: 5-aminosalicylic acid.
Prospective study
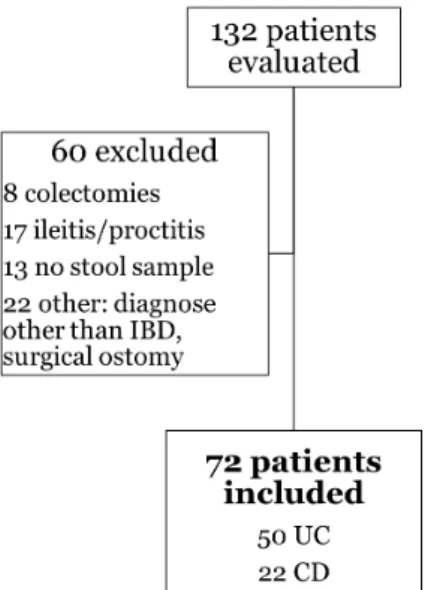
Patients in Study III
Clinical scoring
Endoscopic scoring
Histological scoring
The degree of histological inflammation was determined according to the most severely affected part of the colon.
Faecal markers and blood tests
- Faecal calprotectin
- Faecal lactoferrin
- Blood tests
- Quality of life
- Statistics
- Ethical consideration
The Mann-Whitney U and Kruskall-Wallis tests were used to analyze differences between groups for continuous and ordinal variables. Kendall's tau rank correlation coefficients (r) were calculated to measure the association between two different tests in study I. Receiver operator characteristics (ROC) curve analyzes were performed to visualize the effectiveness of FC different tests and activity indices in studies I–II, and to assess the predictive power of detecting dysplasia or carcinomat time using AUC and carcinomat (AFC) UC for histological inflammation grade (twAUC grade) in study IV.
Rapid tests for faecal calprotectin
NPV for excluding active inflammation at a cutoff of 200 µg/g was higher for CerTest FC (93%) than for CalDetect (79%), but the sensitivity of CerTest FC was clearly lower (25%) than that of CalDetect (67. Comparison of sensitivities, specificities and diagnostic accuracy of CalDetect in ELISA and CDeterect in ELISA) inflammation of moderate/severe inflammation (histological score 0-1 vs. 2-3) with different cut-off limits are presented in Table 20. Comparison of sensitivities, specificities, diagnostic accuracy and negative predictive values of ELISA FC, CerTest FC and CalDetect in differentiating moderate inflammation vs inflammation or moderate histological remission score from moderate inflammation or moderate sever inflammation score (1) 2-3) with different cut-offs in Study I.

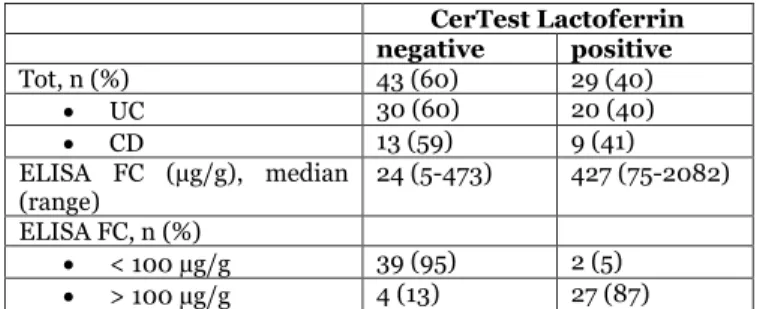
Rapid test for faecal lactoferrin compared to faecal calprotectin . 69
Because of CalDetect's closer correlation with FC ELISA at higher FC concentrations and higher sensitivity in identifying histologic remission, CalDetect was selected for the FC rapid test to be used in the home monitoring study (Study III).
Clinical, endoscopic and histological activity
Patient-reported IBD activity
Patient-reported IBD activity in both studies II-III was low (median IBD symptom index ≤1 point) and was consistent with CalDetect and ELISA FC and clinical and endoscopic indices. The majority of patients in the home monitoring and control groups remained in clinical remission during the study year, with a median IBD symptom index of ≤1 point. Outcomes of patient-reported symptoms and HRQoL in patients monitored and controlled at home at 0, 6, and 12 months.
Physician-reported IBD activity
For the analysis of the patient-reported symptoms in Studies II and III, the IBD symptom index was divided into two parts: partial IBD symptom index without the VAS scale, assessment of the patient-reported IBD activity during the preceding week, and the VAS scale assessing the influence of IBD on the patient's daily life (IBD-VAS). In Study III comparing home monitoring with traditional follow-up of IBD, patient-reported IBD activity did not differ between the home monitoring and control groups, or compliant and noncompliant patients (Table 23). The patient-reported symptoms correlated significantly (p<0.05) with the following parameters in both Studies II-III: ELISA FC (r=0.307), the histological inflammation activity in both CD and UC (r=0.421), and the clinical and endoscopic activity in UC (partial Mayo score r=0.CEIS70, and U.CEIS70).
Combination index
FC: faecal calprotectin, IBD: inflammatory bowel disease pIBD-SI: partial IBD symptom index, VAS: visual analogue scale, pIBD-SI-C: combination index.
Health-related quality of life
The results of the 15D scores in Study III did not differ between the home monitoring group and the control groups at any point in the study (Table 23). Although IBD-VAS was higher at baseline in home-monitored and compliant patients than in non-compliant patients, this difference was not observed for 15D scores. At the end of the study, the median 15D score in home-monitored patients was lower than at baseline, but this difference did not reach statistical significance and was not correlated with more objective markers of IBD activity.
Feasibility of home-monitoring
Effects of home-monitoring in the disease course and the follow-
Effect of the home monitoring on the course of IBD and the follow-up in Study III.
Patient-opinions about the home-monitoring
FC correlates with the inflammatory activity in colonic IBD, especially UC, and is also elevated in colorectal carcinoma in patients with and without IBD (Turvill et al. 2016). This has been linked to the more effective medication, mucosal healing and the comprehensive dysplasia surveillance program (Axelrad et al. 2020). The risk of CRC or advanced colonic neoplasia in colonoscopic surveillance was evaluated in a recent study of 775 patients with colonic IBD (Ten Hove et al. 2019).
In a large study, the median duration of relapses in the home monitoring group was 18 days, compared to 77 days in the control group (Elkjaer et al. 2010). In a Danish home monitoring study (Vinding et al. 2016), academic patients were more compliant than non-academic patients.