Vaahtera M, Kulmala T, Ndekha M, Koivisto A-M, Cullinan T, Salin M-L fi Ashorn P keessatti: Tilmaamtoota da’umsa duraa fi naannoo dahumsaa du’a daa’immanii baadiyyaa Maalaawii keessatti. Biyyi Sahaaraa gadii baha kibba Afrikaa keessa jirtu Maalaawii, addunyaa irratti du’a daa’immanii sadarkaa 7ffaa irratti argamti (UNICEF 2000; Malawi DHS 2000).
REVIEW OF THE LITERATURE
Global development of infant mortality
The trend from 1950 to 1975 was that infant mortality fell just as rapidly (4-5 % decrease annually) in the countries that were highly advanced in 1950 (for example Scandinavia) as in the countries of Eastern and Southern Europe. Reduction of infant mortality rate (IMR) during 1960-1998 in the world Region Reduction of IMR /1000 live births.
Childhood mortality in sub-Saharan Africa
The worst performers in under-five mortality in the 1970s included Burkina Faso, Gambia, Malawi, Mozambique, Senegal and Sierra Leone (Feachem et al. 1991). Malawi stands as an extraordinary country in Africa south of the Sahara with very high infant and under-5 mortality, which has not improved to the same extent as the other East African neighboring countries.
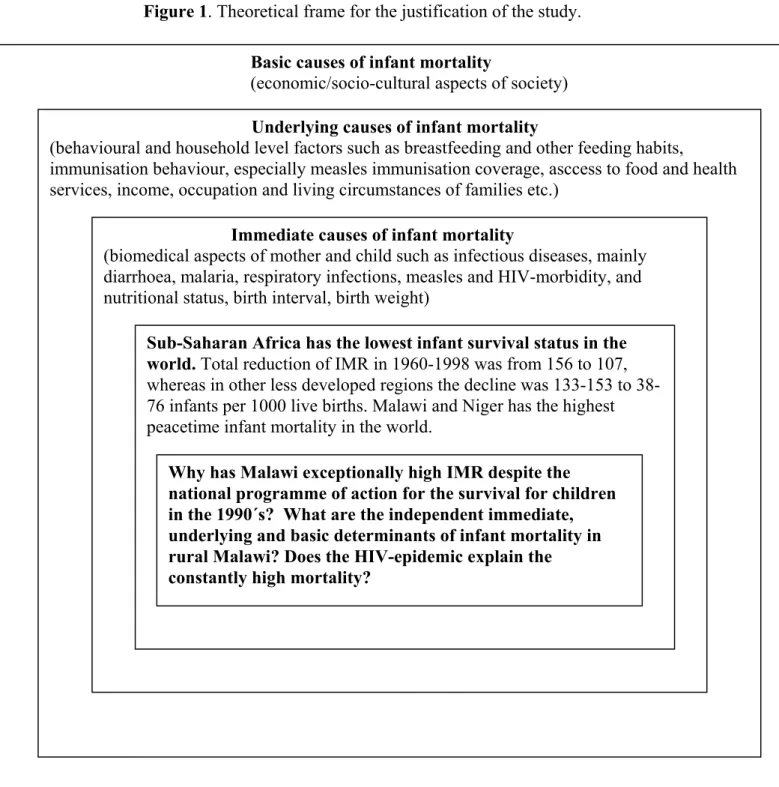
Concept of the causes of infant mortality in developing countries
- Immediate causes of infant death in Africa
- Underlying determinants of infant death in Africa
- Preterm birth/Low birth weight
- Primiparity or high parity, short birth-interval, and previous death of other sibling
- Lack of socio-economic support
- Lack of modern health care or inappropriate health-seeking behaviour
- Maternal HIV-infection
- Inappropriate breastfeeding and complementary feeding practices
- Malnutrition
- Lack of immunisation
The fatality rate (CFR) of measles has been estimated at 3-4% in Africa and Asia (East Africa has a low CFR area) (Aaby et al., 1987). Anthropometric indicators of nutrition are significantly associated with the risk of death (Pelletier et al. 1994).
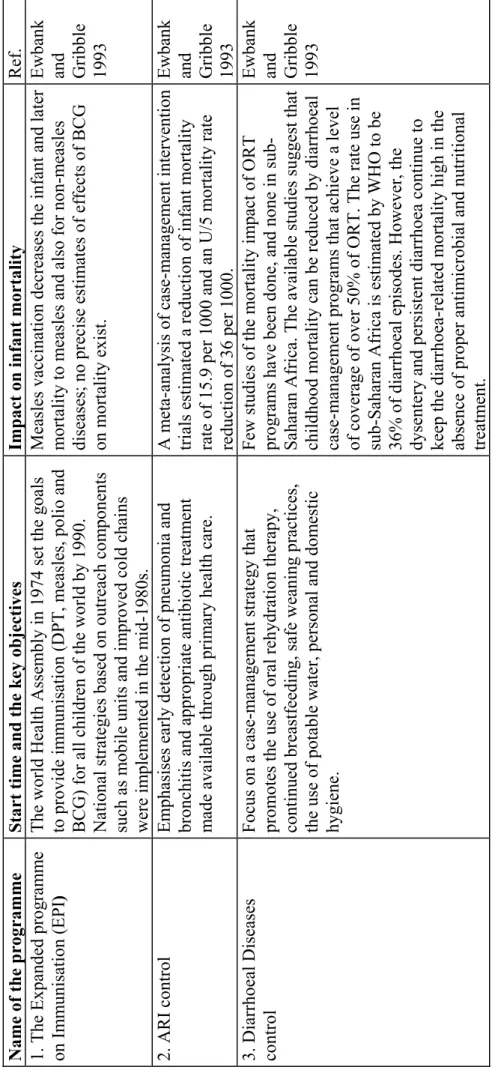
Global programmes on infant health
The Expanded Program on Immunization (EPI) In 1974, the World Health Assembly set the goals of providing immunization (DPT, measles, polio and BCG) to all children in the world by 1990. Only a few studies have been done on the mortality effect of ORT programs. , and none in sub-Saharan Africa.
Government of Malawi-National programme of action for the survival, protection and development of children in the 1990`s
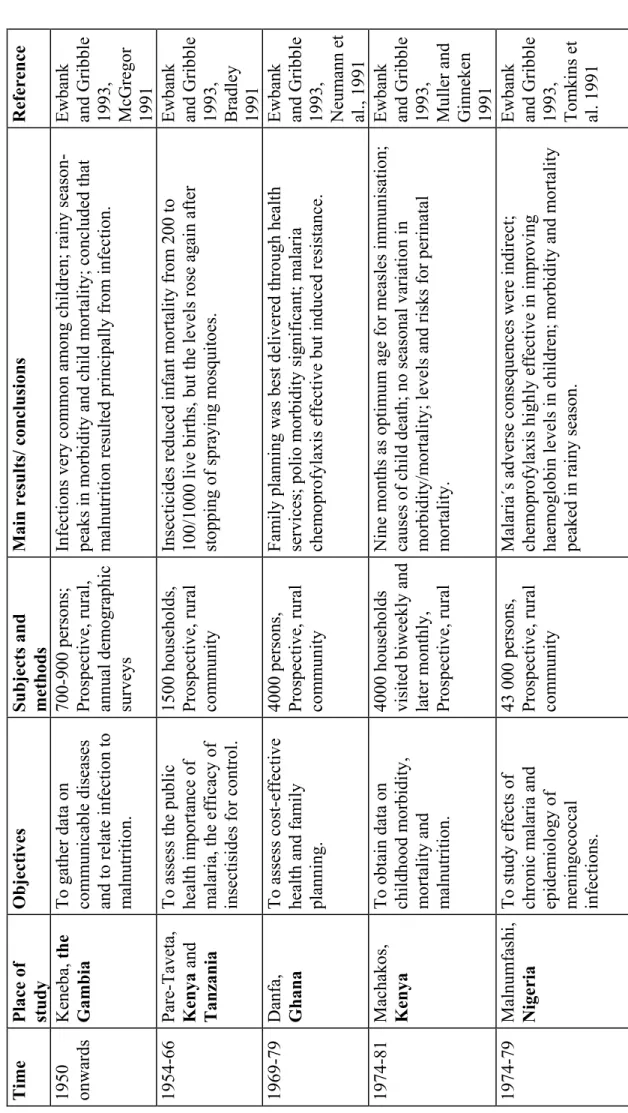
Previous longitudinal studies on infant mortality in sub-Saharan Africa
Four of the six studies reported diarrhea as the leading cause of neonatal death, and measles and malnutrition were also noted as important factors in infant mortality. All of these longitudinal studies have provided some important data on infant mortality rates and the immediate causes of infant morbidity and mortality. Ewbank and Gribble 1993, Neumann et al Machakos, Kenya To obtain data on child morbidity, mortality and malnutrition.
Ewbank and Gribble 1993, Tanner et al., 1991 Juba, SudanTo collect data on morbidity, mortality (causes and death rate) and growth of infants. Watts et al., 1990 Guinea-Bissau To determine infant and under-five mortality rates and leading causes of death. Taha et al Jimma, Ethiopia To describe the socio-economic environments of households, to assess the nutritional status and infant mortality rate.
Semba et al., 1998 Nigeria To assess the risk factors for infant mortality and the causes and seasonality of deaths.
Justification of the study
Why does Malawi have extremely high IMR despite the national child survival program of action in the 1990s? What are the immediate, underlying, and underlying independent determinants of infant mortality in rural Malawi. Immediate causes of infant mortality. biomedical aspects of mother and child such as infectious diseases, mainly diarrhoea, malaria, respiratory infections, measles and HIV morbidity, and nutritional status, birth interval, birth weight).
Underlying causes of infant mortality. behavioral and household factors, such as breastfeeding and other dietary habits, . immunization behaviour, in particular measles vaccination coverage, access to food and health services, income, occupation and living conditions of families, etc.).
HYPOTHESIS AND AIMS OF THE STUDY
To measure the infant mortality rate and to discover the place, time and immediate causes of infant death. To describe mortality rates and health-seeking behavior during episodes of acute fatal illness. To analyze the impact of the HIV epidemic on infant mortality and compare it to other early antenatal, maternal, perinatal and socio-economic events.
To investigate the extent and predictors of exclusive breastfeeding and to describe the changes in infant feeding habits during the first 18 months of life. To analyze the epidemiology, health-seeking behavior and predictors of acute illness episodes among infants. To analyze factors that predict linear growth faltering (severe stunting, ie chronic malnutrition) at twelve months of age.
To describe the population coverage and timing of administration of childhood vaccinations, with a specific focus on measles immunization.
SUBJECTS AND METHODS 1 Setting of studies and follow-up
- Preparatory phase of the study
- Sequence of study examinations
- General set-up of studies
- Study subjects
- Methods
- Summary of studied variables
- Study participants´ background information
- Infant mortality, causes of deaths
- Infant morbidity and health-seeking behaviour
- Growth and development of malnutrition during infancy
- Immunisation practices
- Statistical methods
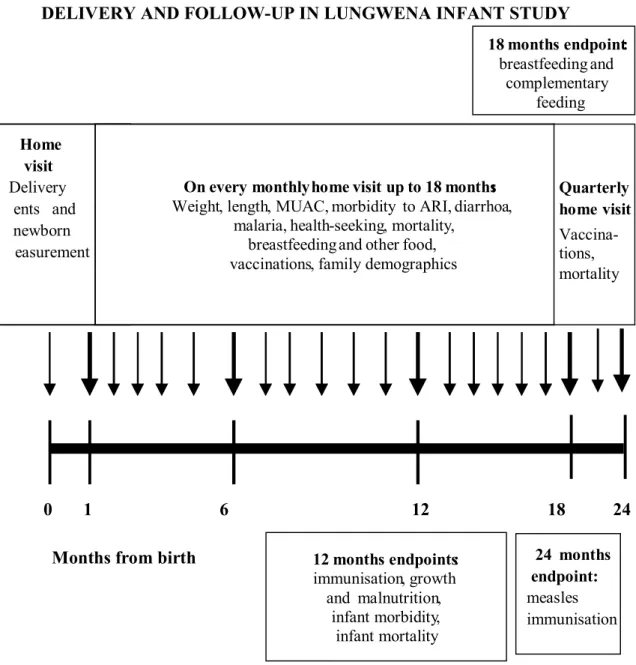
The Lungwena Training Health Center, located in the middle of the Lungwena area, provided conventional preventive and curative modern health services such as family. Residents of the other two areas (south, area 2; west, area 1) did not have access to mobile clinics. In addition, surviving newborns were medically examined by a member of the research team at Lungwena Health Center within four weeks of birth.
The author of this thesis was responsible for field supervision, training and coordination of the research and data collection in Lungwena for two years. Each child received a monthly visit from one of ten local research assistants for the first 18 months of life. Finally, the principal investigator checked the accuracy of the data from the health center records.
Polychotomous logistic regression was performed to test the independent effect of significant predictors of morbidity.

RESULTS
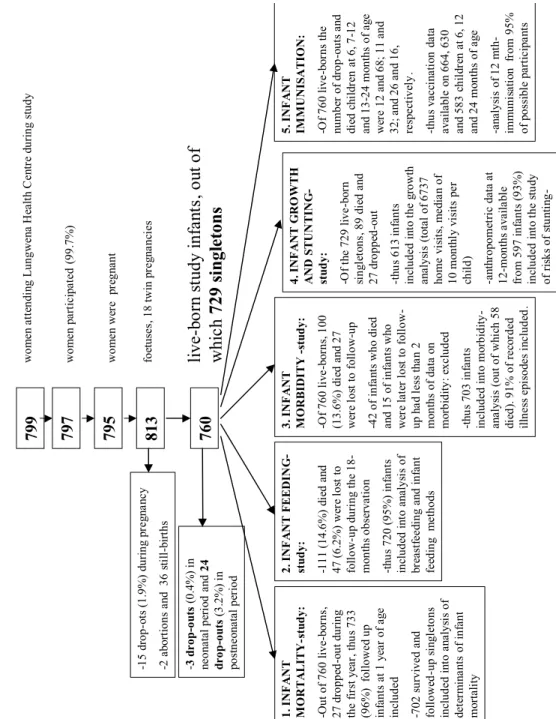
- Enrolment and follow-up
- Levels, immediate causes and predictors of infant mortality (Articles I and III)
- Determinants of breastfeeding and complementary feeding (Article II)
- Infant morbidity and health-seeking (Article III)
- Infant growth, the development of malnutrition and determinants of severe stunting (Article IV)
- Timing and risk factors for incomplete immunisation (Article V)
The Lungwena villages were divided into 4 different areas ("Gulus"), and the average distance to the health center from the center of the area is shown in brackets. There were no differences in overall morbidity or disease duration between survivors and non-survivors (Article III). In a multivariate analysis that adjusted for the child's sex, source of drinking water, sanitation, pet ownership, the presence of fishermen in the household, and some other variables, the child's season of birth was the strongest predictor of infant mortality ( modified OR 2.5).
By four months of age, virtually every infant in the cohort was receiving supplementary foods, and by ten months of age, nearly all infants were eating family foods (Table 2, Article II). Unsafe drinking water increased morbidity risk by 50% and each child in the family by 20%. On the other hand, the morbidity risk was reduced by 23% for each additional Z-score unit (approximately 800 g) in the baby's weight during the first three months of life (Table 4, Article III).
Of all children who remained in follow-up at age two, 81 percent received a measles vaccination through the regular health centers and 3% during the national outreach campaign (Article V).
DISCUSSION
- The hypothesis of high morbidity leading to mortality
- The hypothesis of late health-seeking behaviour
- Vaccine-preventable diseases
- The hypothesis of maternal HIV-infection increasing the infant mortality
- Other underlying determinants of infant mortality
- The hypothesis of malnutrition as underlying cause of infant mortality
- Strengths and limitations of the study
Only one pertussis-like illness has been recorded, which did not lead to the death of the baby. Breastfeeding provides infants with complete nutrition until 4–6 months of age, about half of the nutritional needs for months 6–12 of life, and up to a third of the needs for months of life 12 to 24 (de Cock et et al. 2000). In this study we showed that failure to follow infant feeding guidelines resulted in more than doubling the risk of malnutrition at 1 year of age.
One of the strengths of this study is that exact dates of birth and death were recorded. However, for obvious reasons, causes of infant death were less than accurately recorded, as they were diagnosed through interviews with parents. The fact that many socioeconomic variables were not found to be associated with adverse effects on infant health may be due to the homogeneity of the study population.
However, due to the lack of pediatric HIV testing, we were unable to directly detect the impact of the disease on the growth, morbidity, mortality, and health-seeking behavior of rural Malawian infants.
KEY FINDINGS AND CONCLUSIONS
Breastfeeding was universal until the age of 18 months in Malawi, but the culture of exclusive breastfeeding was absent. Exclusive breastfeeding rates at one, two, three and four months of age were only 0%, respectively. One third of illness episodes were managed at home without outside help, and traditional healers were consulted in 16% and a medical professional in 55% of episodes. Residential area, unsafe water source, low birth weight, and crowding in the family were risks. Factors for increased morbidity.
Boys were significantly more commonly underweight and stunted at one year of age than girls. The lack of exclusive breastfeeding and home deliveries increased the theoretical risk of vertical transmission of HIV to newborn babies. In addition to HIV, the other infectious diseases (acute respiratory infections, diarrhea and malaria) and many underlying determinants (primiparous mother, low weight gain during pregnancy, low birth weight, chronic malnutrition (acquisition) and behavioral aspects related to breastfeeding and health-seeking habits) still the child mortality high in rural Malawi.
Lack of exclusive breastfeeding and very late initiation of family foods in infants (leading to stunting, chronic infant malnutrition).
PUBLIC HEALTH IMPLICATIONS AND TARGETS FOR FUTURE RESEARCH
Thus, the quality of antenatal clinic breastfeeding educational sessions would be important to investigate and the reasons for non-adherence to recommendations should be sought. Thus, antimicrobial treatment in case of dysentery and continuous support and follow-up of advanced growth of infants should be promoted. In light of this knowledge, every opportunity should be taken to immunize against measles in Lungwena, with the help of.
My heartfelt thanks go to the research assistants of Lungwena Child Survival Study and the families in Lungwena, without whom the study would never have been as successful as it is now. I thank Professor John Chipangwi, MD, Professor Emeritus Niilo Hallman, MD, and Professor Emeritus Jarmo Visakorpi, MD, for their significant support for the study. I express my deepest gratitude to the official reviewers, Professor Aulikki Nissinen, M.D., and Professor Olli Simell, M.D., for their very wise and supportive comments on the manuscript.
Tampere University Hospital, the Research Foundation of the Mannerheim League for Child Welfare, the Research Foundation at the University of Tampere and the Tampere City Science Foundation are greatly acknowledged.
Maternal HIV infection and infant mortality in Malawi: evidence of increased mortality due to placental malaria infection. Ewbank DC, Gribble JN (eds, 1993): Effects of health programs on child mortality in sub-Saharan Africa. Koenig MA, Philips JF, Campbell OM, D´Souza S (1990): Birth intervals and child mortality in rural Bangladesh.
Madise NJ, Diamond I (1995): Determinants of infant mortality in Malawi: an analysis controlling for death clustering in families. Pelletier DL, Frongillo EA, Schroeder DG, Habicht J-P (1995): The effects of malnutrition on child mortality in developing countries. Taha TE, Dallabetta GA, Canner JK; Chipangwi JD, Liomba G, Hoover DR, Miotti PG (1995): The effect of human immunodeficiency virus infection on birth weight and infant and child mortality in urban Malawi.
Taha TET, Dallabetta GA, Canner JK, Chipangwi JD, Liomba G, Hoover DR, Miotti PG (1995): The effect of Human Immunodeficiency Virus infection on birth weight and infant and child mortality in urban Malawi.