Chronic rhinosinusitis (CRS), allergic rhinitis and asthma are common conditions, with prevalences between 1-20% in the general population. Sinus surgery is considered when conservative therapy fails to achieve adequate disease control in the treatment of CRS. Currently, very few randomized controlled trials are available comparing traditional functional endoscopic sinus surgery (FESS) with minimally invasive endoscopic sinus surgery.
This thesis aims to investigate whether IDO may play a role in the pathogenesis and evolution of the above diseases and to compare the subjective and objective outcomes of FESS and minimally invasive endoscopic sinus surgery. IV Endoscopic sinus surgery with antrostomy has a better early endoscopic recovery compared to the technique in which the ostium is preserved.
INTRODUCTION
REVIEW OF THE LITERATURE
- Anatomy and physiology of the airways
- Allergic rhinitis
- Epidemiology of AR
- Genetics of AR
- Pathophysiology of AR
- Clinical presentation of AR
- Diagnostic criteria of AR
- Clinical management
- Chronic rhinosinusitis
- Epidemiology of CRS
- Genetics of CRS
- Pathophysiology of CRS
- Clinical presentation of CRS
- Diagnostic criteria of CRS
- Conditions associating or mimicking CRS
- Clinical management of CRS
- Asthma
- Epidemiology of asthma
- Genetics of asthma
- Pathophysiology of asthma
- Clinical presentation of asthma
- Diagnosis of asthma
- Associated comorbidities and differential diagnosis of asthma
- Clinical management
- United airways
- Indoleamine 2,3 dioxygenase
- Tryptophan degradation and Indoleamine 2,3-dioxygenase
- The mechanisms of action of IDO
- IDO and diseases
As an example, Toll-like receptors (TLR) 1-10 are widely expressed in the nasal epithelium (Fokkens et al. 2012). However, their role in the pathogenesis of CRS has not been resolved (Toppila-Salmi et al. 2015). Nasal irrigation with saline (isotonic or hypertonic) is beneficial in terms of symptom relief (Fokkens et al. 2012).
Normal baseline activity in asthmatics could be induced by using inhaled corticosteroids (Maneechotesuwan et al. 2008). Pharmacological inhibition of IDO exacerbated symptoms in experimental allergic asthma (van der Sluijs et al. 2013).
AIMS OF THE STUDY
MATERIALS AND METHODS
- Ethical aspects
- Study design and population
- Study I
- Study II
- Study III
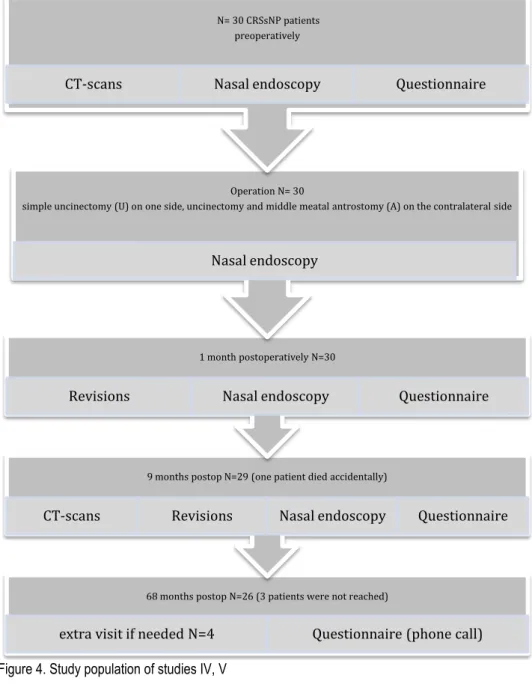
- Studies IV, V
- Laboratory methods
- Biopsies
- Sample staining (I, II)
- Light microscopic evaluation (I, II)
- IDO activity measurement and absolute eosinophil count (III); serum and
- Sinus surgery and clinical evaluation of CRS (IV, V)
- FESS
- Endoscopy (IV)
- CT- scans (IV)
- Questionnaires and symptoms reporting (IV, V)
- Evaluation of job exposure (V)
- Statistical analysis of results
In addition, at least a 6-month period of regular, continuous use of anti-asthma medication must have passed at the time of the decision. Uncinectomy is performed on both sides, in which the lower two thirds of the uncinate. It is performed by removing with scissors the posterior connective tissue of the natural ostium, to double the diameter.
Endoscopic score 0 was normal, 1=mild, 2=moderate, 3=severe changes in the perineum and ostiomeatal complex. The determination of the patient's other comorbidities was based on medical records, interview and medical examination.
RESULTS
The association of IDO to inflammatory upper airway diseases in
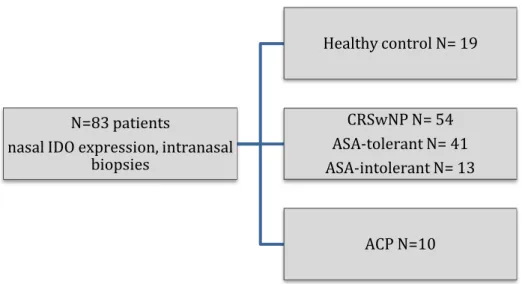
- Expression of IDO in the nasal cavity during CRSwNP and ACP (I)
- Expression of IDO in the maxillary sinus mucosa during CRSsNP and
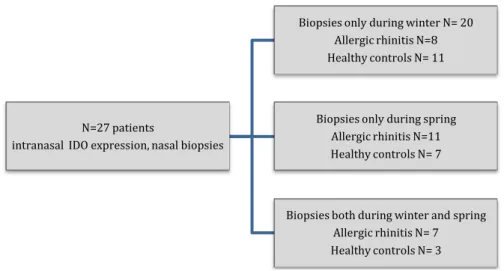
- IDO expression in patients with allergic rhinitis (II)
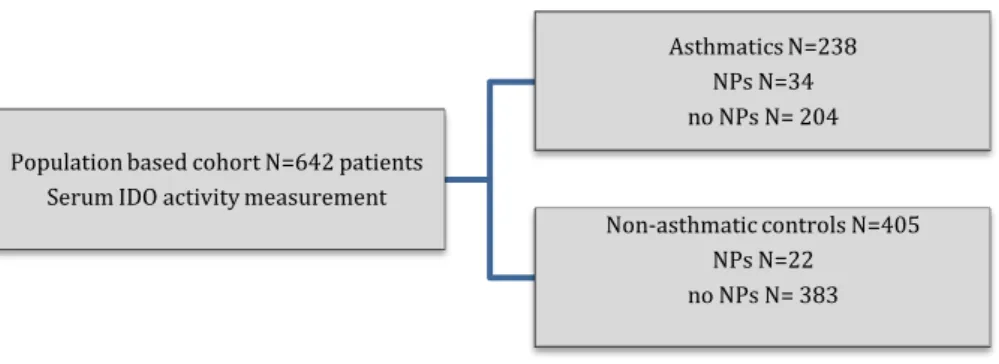
- IDO activity
- Blood eosinophilia
- Relationships between asthma, CRSwNP and aspirin intolerance
- Effect of rural environment during childhood
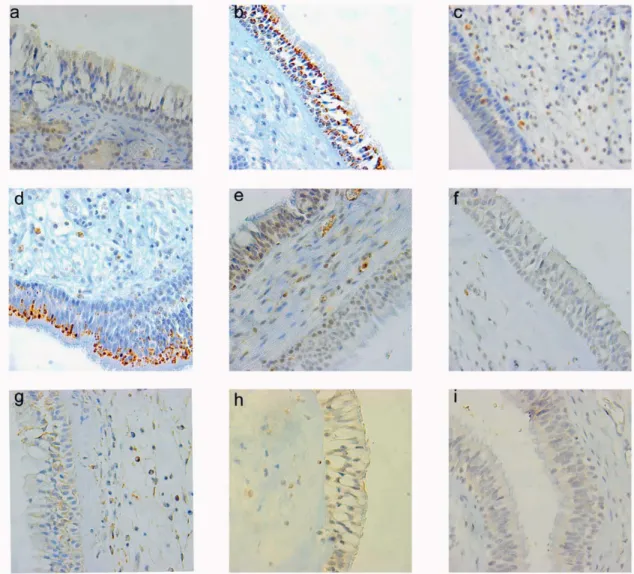
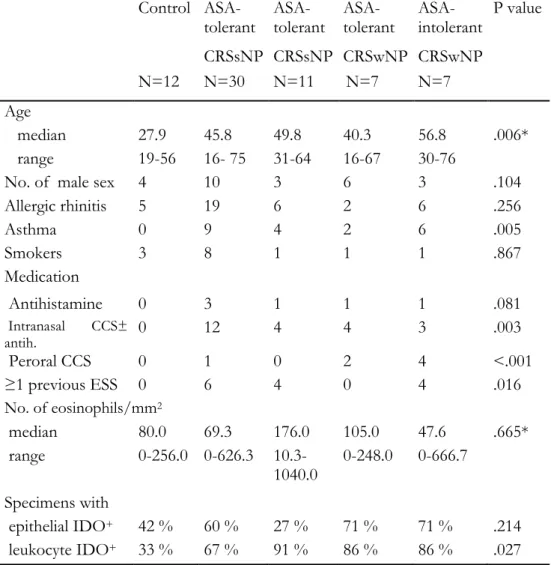
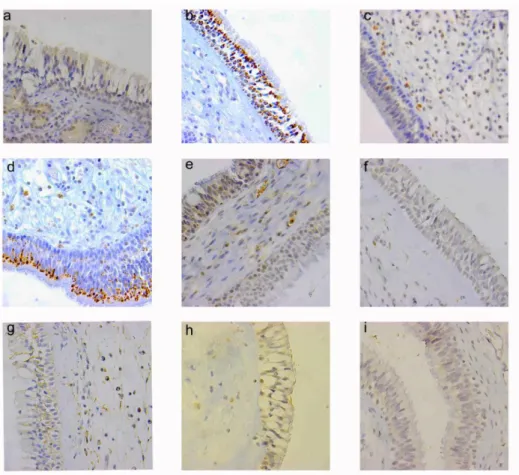
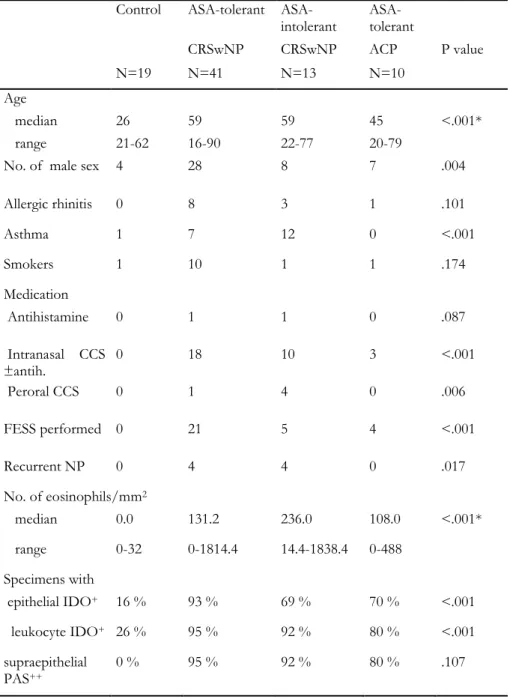
The percentage of IDO positive leukocytes was significantly higher in CRSwNP and ACP samples, compared to control inferior turbinates (p < 0.001 and p . < 0.05, respectively). The median percentage of IDO positive leukocytes correlates with epithelial IDO positivity (median percentages of IDO positive and negative eosinophils 13% and 0%, respectively, p < 0.001). The median number of eosinophils was significantly higher in epithelial IDO positive than in epithelial IDO negative groups (median number of mucosal eosinophils 10.4/mm2 and 0.04/mm2, respectively, p < 0.001). Furthermore, the number of eosinophils/mm2 correlated significantly with the percentage of IDO positive leukocytes (p < 0.01, r . = 0.41).
In contrast, the median percentage of IDO positive leukocytes was significantly higher in CRSwNP samples compared to both control sinus mucosa and CRSsNP groups (p < 0.05). The number of mucosal eosinophils did not differ in CRSsNP or CRSwNP groups, compared to control sinus mucosa (p > 0.05). Epithelial IDO positive and negative groups did not differ statistically significantly in the median percentage of IDO positive leukocytes and in the median number of eosinophils (respectively p > 0.05 and p > 0.05).
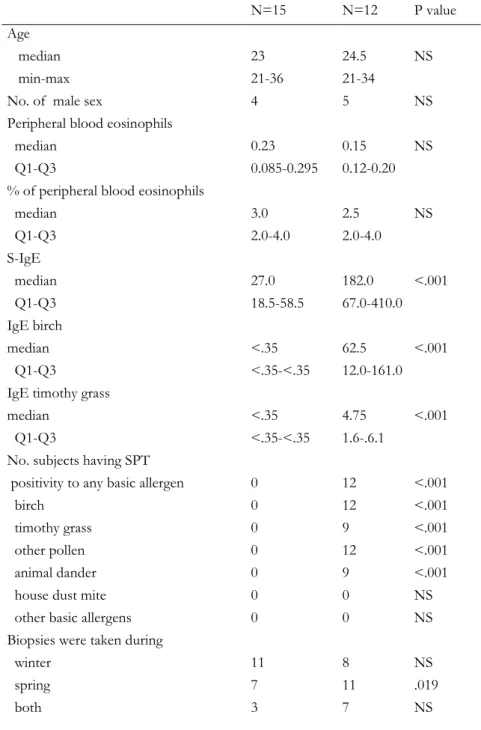
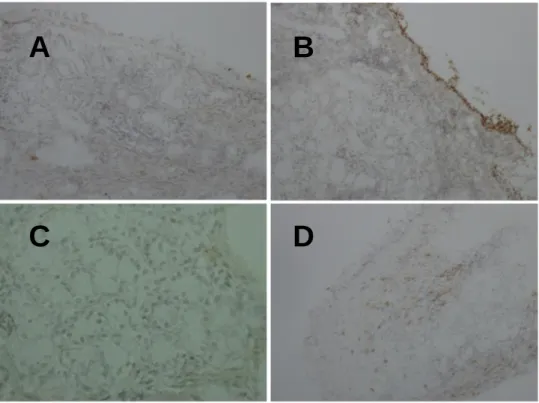
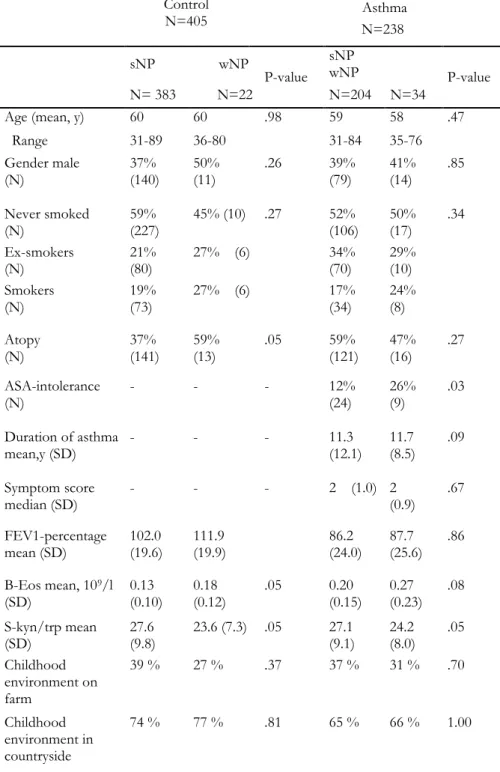
The number of eosinophils/mm2 did not correlate with the percentage of IDO-positive leukocytes (p > 0.05). Subjects had no changes in epithelial IDO expression or in the percentage of IDO-positive leukocytes when comparing winter and spring samples from the same individuals (P>0.05). The median mucosal eosinophil count was significantly higher in atopic than non-atopic subjects only during the symptomatic spring (P=0.044), while percentage eosinophils did not differ significantly between atopic and non-atopic subjects (P>0.05).
Interestingly, during the spring the number of mucosal leukocytes and the percentage of IDO-positive leukocytes correlated significantly (P<0.05, r=0.46. IDO activity, measured by the serum kynurenine to tryptophan ratio, was studied in asthma, CRSwNP and atopy, in to detect changes of IDO activity at the serum level during airway inflammation Childhood spent on the farm or in the countryside was not associated with patient-reported physician-diagnosed CRSwNP (Table 2).
Outcomes of endoscopic sinus surgery in patients with CRSsNP (IV, V)
- Endoscopic outcomes (IV)
- Correlation of endoscopic findings to paranasal CT-scans
- Correlation of endoscopic findings to patient factors, symptoms and adhesions
- Subjective outcomes (V)
- Symptoms during the debridement visit
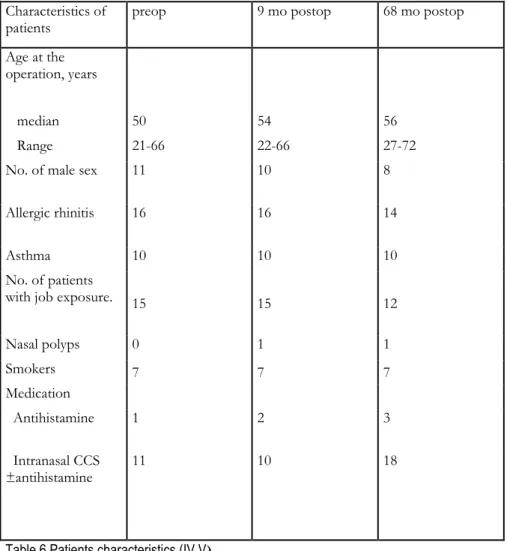
- Post-operative symptoms (9 and 68 months post-surgery)
- Satisfaction with operation and revision surgery
- Exacerbations of CRSsNP post-surgery
- The influence of patient history
There were no peri- or postoperative differences between the operative techniques in terms of additional ostium, maxillary mucosal edema and secretions, evaluated endoscopically (p>0.05, p>0.05 and p>0.05, respectively). However, there was a correlation between maxillary sinus secretions and endoscopic middle meatus score at 9 months postoperatively, but not with maxillary mucosal edema (the uncinectomy-only side P<0.01, R=0.67; the antrostomy side P<0.01, R=0.58 , p> 0.05, respectively). In contrast, the endoscopic score was not associated with age, gender, smoking, asthma or medication (p>0.05).
Sex, allergic rhinitis, asthma, smoking, nasal corticosteroids and/or antihistamine use were not associated with an obstructed maxillary sinus ostium, a swollen maxillary sinus mucosa or secretions, or adhesion formation (asthma not tested) (p>0.05, p> 0.05, p>0. and p>0.05 Pre- or postoperative endoscopic scores correlate with any of the symptoms asked at the same time on either ostium-preserving or -enlarging sides (p >0, 05).symptoms 9 months postoperatively (p>0.05).
A swollen mucosa of the maxillary sinus, the presence of adhesions or secretions was not associated with any of the required postoperative symptoms at the same time on either the ostium-preserving or augmenting sides (p<0.05 and p>0.05, respectively). There were no significant differences between surgical techniques in the mean values of each of these four symptoms (p>0.05). Furthermore, delta values indicating the change of these three symptoms before and after surgery did not differ between surgical techniques at nine months and on average at 68 months after surgery (p>0.05).
When satisfaction with the operation was observed at nine months and on average 68 months postoperatively, the majority of patients expressed good/moderate satisfaction and there were no differences between operative techniques in the reported satisfaction (p>0.05). Revision surgery was performed on one antrostomy side and three uncinectomy-only sides for 3 out of 26 patients during the observation period, but this difference between the sides remained statistically insignificant (p>0.05). Moreover, these symptom and satisfaction values did not correlate with age or the number of acute sinusitis/year (p>0.05).
DISCUSSION
In contrast to our findings, which showed that local IDO is not associated with AR pollen and at a systemic level with asthma, other studies suggest that IDO has a role in the control of atopic airway diseases (Odemuyiwa et al. 2004, von Bubnoff, Bieber 2012). Pharmacological inhibition of IDO causes marked exacerbation of inflammation and exacerbation of disease symptoms in a mouse model of inflammatory bowel disease (Gurtner et al. 2003). Endoscopic findings, such as middle turbinate size, possible adhesions, crusting, and inflammation, have been shown to have acceptable interexaminer reproducibility and are suitable for evaluating ESS (Smith et al. 2012, Nair 2009).
Moreover, our findings of successful long-term endoscopic recovery with both techniques correlate with the observations of others (Mace et al. 2010, Guo et al. 2010). This finding is in line with a study showing that successful recovery just one month after surgery also appears to predict the long-term success of ESS (Rudmik et al. 2011). The study concluded that ESS is more effective than conservative therapy in improving quality of life (measured by sinonasal outcome test-22), endoscopic assessment and use of medication (Smith et al. 2014).
Operative management of CRS refractory to conservative therapy requires suspicion of asthma in patients with CRSwNP (Hakansson et al. 2014). It is now known that full recovery after surgery takes months and up to more than a year after surgery (Verim et al. 2014). Similarly, local immune impairment has been reported in eosinophilic diseases of the upper respiratory tract, including CRSwNP and AR (Hupin et al. 2013).
This is consistent with previous observations that risk factors influence the need for ESS revision, or subjective outcomes after balloon sinuplasty (Hox et al. 2012, Koskinen et al. 2012). Furthermore, the presence or absence of AR does not appear to influence the endoscopic diagnosis of CRS (Tomassen et al. 2011). The anti-IDO MAB we used cannot distinguish between IDO1 and IDO2 isotopes, which may have different roles ( Lob et al. 2009 ).
CONCLUSIONS
2009, "Gene Expression Profiling Associated with Asthma Exacerbations", Clinical and Experimental Allergy: Journal of the British Association for Allergy and Clinical Immunology, vol. 2003, "Comparison of Airway Response to Segmental Antigen Bronchochallenge in Atopic Asthma and Allergic Rhinitis", Journal of Allergy and Clinical Immunology, vol. 2012, "Lung injury and airway remodeling in severe asthma", Clinical and Experimental Allergy: Journal of the British Society of Allergy and Clinical Immunology, vol.
2007, "The role of indoleamine 2,3-dioxygenase in transplantation", Transplant international: official journal of the European Society for Organ Transplantation, vol. 2014, “Host-microbial interactions in patients with chronic rhinosinusitis,” The Journal of Allergy and Clinical Immunology, vol. 34;Genetics of Chronic Rhinosinusitis: State of the Art and Directions Forward", The Journal of allergies and clinical immunology, vol.
2013, "Indoleamine 2,3-dioxygenase expression is associated with chronic rhinosinusitis: review of the evidence", Current Opinion in Allergy and Clinical Immunology, vol. 2014, "Role of nasal packing in surgical outcomes for chronic rhinosinusitis with polyposis", Laryngoscope, vol.124, no. 34;Asymptomatic atopy is associated with increased indoleamine-2,3-dioxygenase activity and interleukin-10 production during seasonal allergen exposure", Clinical and Experimental Allergy: Journal of the British Society for Allergy and Clinical Immunology, vol.
Indoleamine 2,3-dioxygenase (IDO) is an enzyme expressed in many cells involved in the catabolism of the essential amino acid tryptophan to kynurenine. Indoleamine 2,3 dioxygenase (IDO) is an intracellular enzyme that initiates the first and rate-limiting step of tryptophan degradation along the kynurenine pathway (14). Indoleamine 2,3 dioxygenase (IDO) is an intracellular enzyme that initiates the first and rate-limiting step of tryptophan degradation along the kynurenine pathway [1].
Indoleamine 2,3dioxygenase (IDO) is an enzyme involved in the catabolism of the essential amino acid tryptophan (Trp) to kynurenine (Kyn). Indoleamine 2,3 dioxygenase (IDO) is an intracellular enzyme that initiates the first and rate-limiting step in the cleavage of tryptophan (Trp) along the kynurenine (Kyn) pathway. Accelerated second immunogenic tumor transplant rejection in mice under inhibition of indoleamine 2,3dioxygenase activity by ethyl pyruvate.
Endoscopic and radiological findings of the mucosa and mouth of the maxillary sinus were significantly correlated 9 months after surgery.