Patients undergoing spinal fusion, scoliosis, and lumbar microdiscectomy surgery experience very severe pain in the postoperative period, which may increase the incidence of postoperative morbidity and complications. On the other hand, little information exists about the clinical pharmacist intervention in the operating room, PC Gordon et al. 2004) advised that the SA Association of Anesthesiologists should be involved with the pharmacist for various improvements (28). Due to all the previously mentioned positive impacts of the clinical pharmacist in the different areas, I carried out a new idea by performing the clinical pharmacist intervention after the different anesthesia strategies during spinal fusion, scoliosis and microdiscectomy surgery.
Ketamine
- Mechanism of action
- Ketamine effect on hemodynamic stability
- Uses of low dose ketamine post-operatively as an analgesic
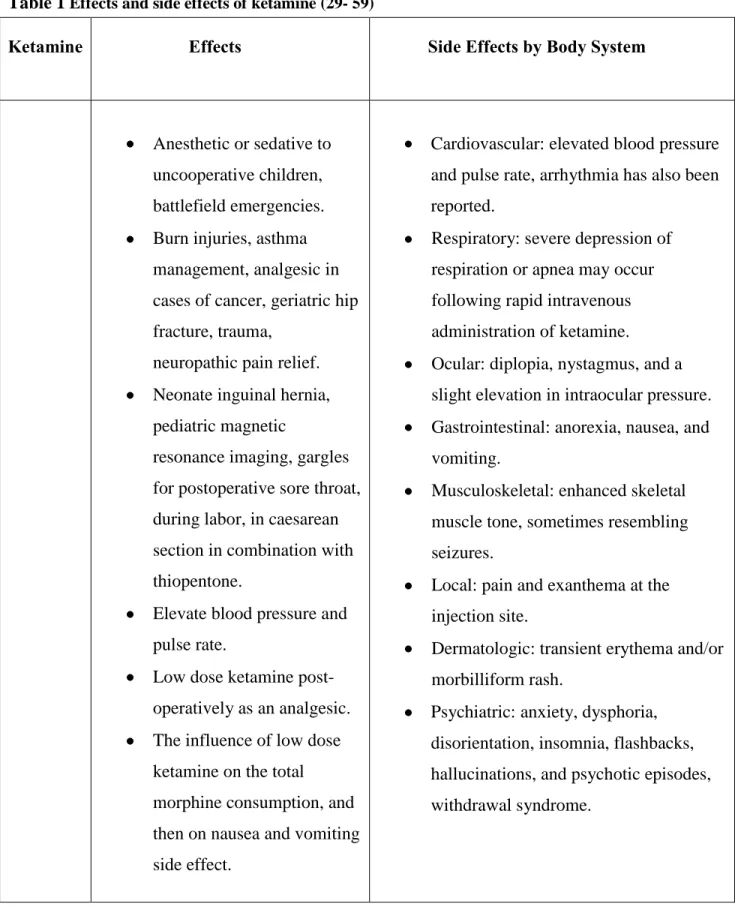
- The influence of low dose ketamine on the total morphine consumption, and then on nausea and vomiting side effects
- Management methods used for post-operative pain in spinal fusion, scoliosis, and microdiscectomy surgery
Effect of low-dose ketamine on total morphine consumption, and subsequently on side effects of nausea and vomiting, then on side effects of nausea and vomiting. Low-dose ketamine (1 μg/kg/min) has previously been tested intraoperatively perioperatively in major abdominal surgery (5) to reduce postoperative intravenous morphine consumption. Effect of low-dose ketamine on total morphine consumption and subsequent side effect of nausea and vomiting.
Clinical pharmacy and pharmaceutical care
Definition and development of pharmaceutical care
The term "pharmaceutical care" has established itself as a philosophy of practice, with the patient and the community as the main beneficiaries of the pharmacist's actions. The model of pharmaceutical care is perhaps the most advanced in the United Kingdom (UK), as evidenced by the National Health Service's (NHS) new contractual frameworks for community pharmacies (CPCF) (65). A number of studies have demonstrated the clinical and economic benefits of clinical pharmacy interventions in hospitals and primary care (20).
Effectiveness of pharmaceutical care
Comprehensive or cognitive pharmacy services involve activities both to ensure good health and to avoid ill health in the population. 71) 2005, looking at the effectiveness of pharmaceutical care services in the community or ambulatory setting on patient outcomes, included 22 randomized controlled trials from 1990 to 2003 (71) and provided an evidence base for improving medication use. The reviews identified in the literature search regarding the role of the pharmacist showed that the pharmacist has significant positive effects on HbA1c levels (73), systolic BP (74) and total cholesterol (75) as well as on low-density lipoprotein (LDL) cholesterol and triglyceride levels.
Three main components of pharmaceutical care
Intestinal clearance can be ordered if the patient is to be operated on in the lower gastrointestinal tract (99). The patient is transferred to the PACU after the surgical procedure, anesthesia reversal and extubation (if necessary). The doctor must be notified if the patient has not passed urine six to eight hours after the operation.
Their families should be involved in preoperative education so that they can help the patient at home. The patient should be monitored for signs of potential complications, such as leg swelling, redness and pain (deep vein thrombosis), shortness of breath (pulmonary embolism), dehiscence (separation) of the incision, or ileus (intestinal obstruction).
OBJECTIVES
METHODS
- Study design and methods
- Spinal fusion surgery
- Scoliosis surgery
- Summary to the inclusion and exclusion criteria for patients undergoing the three types of surgeries
- Data analysis
- Introducing the pharmaceutical care program
- Pharmaceutical care program
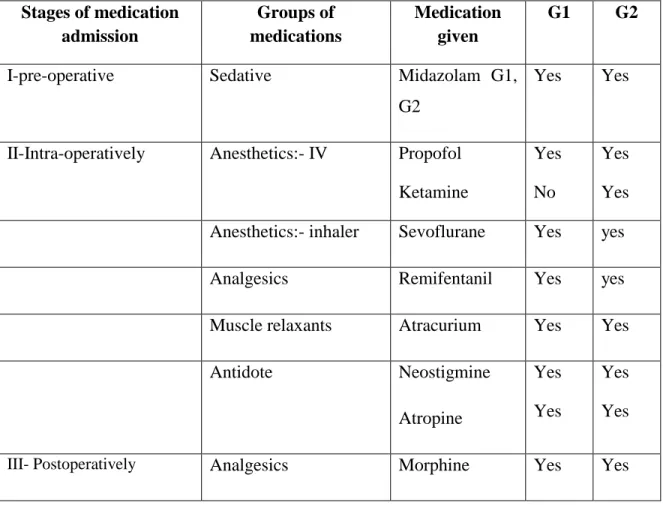
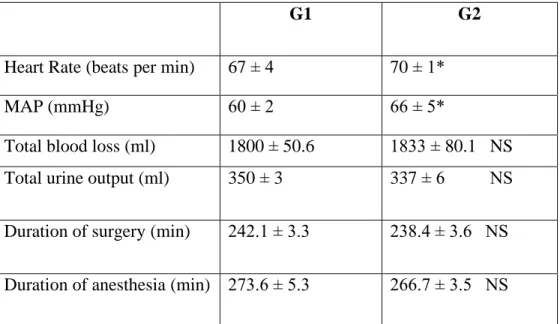
At the end of the operation, all drugs were stopped, both groups received antidotes which were - neostigmine (2.5 mg/IV), atropine (1 mg/IV) and administered together in a single bolus dose from one syringe, which followed by 100% oxygen (Table 10). The severity of postoperative pain was assessed in the first 24 hours after surgery using the Visual Face Rating Scale and pain was controlled with intravenous morphine. Heart rate (beats/min), mean arterial pressure (MAP) (mmHg) were recorded at 5-minute intervals during surgery, where the dose of infused drugs was adjusted to maintain mean blood pressure around 60 mmHg.
The duration of the anesthesia and the total time of the operation (min), the volume of blood loss (ml) and urine output (ml) and the immediate recovery time were recorded. All patients were informed about the details of the procedures and their written consent was observed for each patient. All patients included in this study underwent scoliosis surgery for the first time with a curvature of the spine greater than 40°.
At the end of surgery, both groups received doses of neostigmine, atropine as described above along with 100% oxygen. The duration of the anesthesia and the total time of the operation (min), the volume of blood loss (ml) and urine output (ml), the time to achieve the awakening test and the immediate recovery time were recorded. All patients were informed about the details of the procedures and written consent was obtained from each patient.
All drugs were discontinued at the end of surgery, except G3, where ketamine was administered at a dose of 1 μg/kg/min for 24 hours (Table 14).
RESULTS
- The out results of investigating the influence of adding ketamine in 3 types of surgery intra- and post- operatively by applying pharmaceutical
- Spinal fusion surgery 1. Patient characteristics
- Scoliosis surgery 1. Patient characteristic
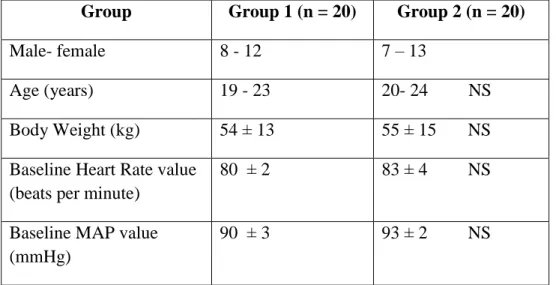
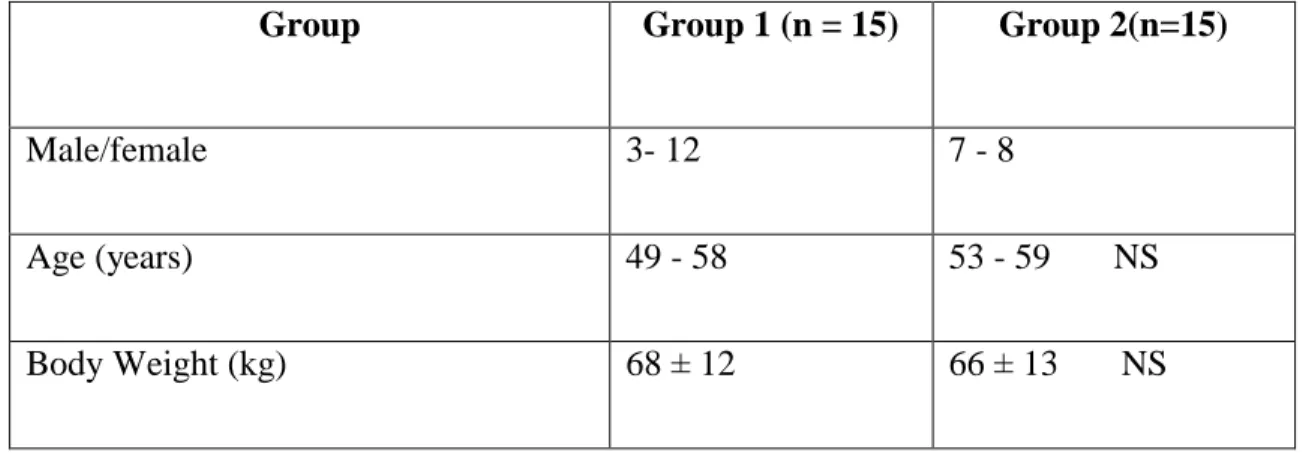
Since no significant differences were found, they were subsequently treated as one group despite the obvious differences in gender and age. No patient in either group reported dysphoria or hallucinations, tremors, and loss of respiration or vision, but no differences were observed in the incidence of purulence and postoperative nausea and vomiting between the two groups. A preliminary analysis showed that there were no significant differences between men and women in their groups for any of the parameters measured, so they were subsequently considered as one group despite the differences in gender and age, which may indicate the success of the initial randomization process (Table 11). .
Regarding the immediate recovery time and the time elapsed until the first patient analgesia request in the PACU, the recorded values were significantly different. No patients in either group reported dysphoria, chills, and respiratory or vision loss, and no differences were noted in the incidence of pruritus, postoperative nausea, and vomiting in the two groups. The three groups of patients studied were found to be comparable in terms of gender, age, weight and duration of surgery (Table 13).
Comparisons of the data found that there were no significant differences (P>0.05) between any of the parameters measured across the groups. In the absence of any significant differences found between the groups, they were subsequently considered comparable groups despite their apparent gender and age differences (Table 13). The duration of the operation was not significantly different between the patients in the three groups (P > 0.05) (Table 21).
The results of statistical comparisons show that there was a significant difference between the scores of G1 and G2 (P > 0.05), and between the scores of G1 and G3 (P > 0.05), while there was no significant difference between G2 and G3. (Table 21).
DISCUSSION
- The influence of adding ketamine in spinal fusion, scoliosis, and microdiscectomy surgery intra operatively, and post operatively by
- Spinal fusion surgery and scoliosis surgery
- Microdiscectomy surgery
- Clinical pharmacists involvement with the study
These results show that the combination of low-dose ketamine and remifentanil infusions as TIVA during spinal fusion and scoliosis surgery can provide better hemodynamic stability so that a greater surgical need is satisfied. Addition of low-dose ketamine hydrochloride infusion may be used as a routine therapy to improve hemodynamic stability during spinal fusion and scoliosis surgery and reduce postoperative morphine consumption. I have investigated the use of low-dose ketamine in both intra- and postoperative lumbar microdiscectomy because it is well known that patients undergoing this type of surgery experience severe pain in the postoperative period (108).
Fountas et al (1999) examined various methods for postoperative pain after lumbar microdiscectomy surgery (23), but did not use a low dose of ketamine, such as 1 μg/kg/min, as used in this study, as a possible method for this. . control. However, this unusual analgesic action is well documented, as well as its ability at low doses to produce a morphine-sparing effect, which can be a very beneficial effect for postoperative use (5), so I chose a low dose of ketamine in this study. Low-dose ketamine (1 μg/kg/min) has previously been tested intraoperatively in back surgery, including scoliosis and spinal fusion surgery, as a randomized, placebo-controlled, two-arm study. In this study, I randomly tested a controlled group G1 with patients G2 who used ketamine intraoperatively and G3 who used ketamine intraoperatively and postoperatively in laminectomy surgery.
These results were similar to mine, as our results showed that lowering morphine consumption is associated with reducing its side effects such as nausea and vomiting, and the use of the low dose (1μg/kg/min) of ketamine was not associated with any transient psychotic effects. This is not the first study in which ketamine has been used in a low concentration after surgery, as Frederic Adame and his colleagues (115) evaluated the effect of low-dose ketamine on postoperative pain relief and total morphine consumption after total knee replacement. arthroplasty, but ketamine was never tested in microdiscectomy. Their results confirmed that low-dose ketamine was a useful analgesic adjuvant in perioperative multimodal analgesia with a positive impact on early knee mobilization.
In this study, I have investigated various parameters regarding the addition of low-dose ketamine intra and postoperatively, other studies have tested additional positive effects of ketamine, on narcotic tolerance patients (53), the achievement of hemodynamic stability (110) and its prevention of postoperative hyperalgesia effect (116), all these parameters give ketamine a superior effect compared to other analgesics.
NEW SCIENTIFIC RESULTS AND CONCLUSIONS
By adding a low dose to overcome the annoying psychotic side effect at the normal dose. Joint clinical pharmacy practice based on pharmacological and pharmacodynamic data played an effective role in improving the overall outcome of the different surgeries. The clinical pharmacist can play many positive roles before surgery, during surgery, and in the management of postoperative pain.
SUMMARY
ÖSSZEFOGLALÁS
Effects of low-dose ketamine on morphine consumption in surgical intensive care patients following major abdominal surgery. 2006) Pharmaceutical care - a new discipline in the curriculum: familiarizing pharmacy students with drug non-compliance Chimia. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. 2006) Clinical pharmacists and hospital nursing: a systematic review. 2008) Economic effects of clinical pharmacy interventions: a literature review. 2000).
Becke K, Albrecht S, Schmitz B, Rech D, Koppert W, Schüttler J,Hering W. 2005) Low-dose intraoperative S-ketamine has no preventive effects on postoperative pain and morphine consumption after major urological surgery in children. Reduction of postoperative pain after instrumented spinal fusion using intrathecal morphine. 2008) Nonsteroidal anti-inflammatory drugs for the management of postoperative pain after lumbar spine surgery: a meta-analysis of randomized controlled trials. 2006). Postoperative analgesia after major spine surgery: patient-controlled epidural analgesia versus patient-controlled intravenous analgesia. 2008).
Farris KB, Fernandez-Llimos F, Benrimoj SI. 2005) Pharmaceutical care in community pharmacies: practice and research from around the world Ann Pharmacother. A systematic review of published studies, 1990 to 2003, examining effectiveness in improving patient outcomes. 2007) Clinical and economic outcomes of pharmacist-directed antimicrobial prophylaxis in surgical patients. 2008) Effects of outpatient pharmacist interventions on adults with diabetes mellitus: a systematic review. Javery KB, Ussery TW, Steger HG, Colclough GW. 1996) Comparison of morphine and morphine with ketamine for postoperative analgesia. 2002) The efficacy of the morphine-Adcon-L compound in the treatment of postoperative pain after lumbar microdiscectomy.
The influence of anesthetic agent selection for scoliosis surgery on the management of intraoperative hemodynamic stability and postoperative pain – pharmaceutical care program.
OWN PUBLICATIONS RELATED TO THE THESIS
ACKNOWLEDGEMENTS
OFFPRINTS OF THE PUBLICATIONS