For this reason, a radical change in the organization of the NHS is needed, in harmony with a change in the role played by the state. According to the WHO-GARD guidelines, we collaborated on the creation of the Italian GARD. The right to health, as defined in the Italian Republic Constitution, is one of the fundamental rights of an individual.
1. to prevent respiratory diseases from developing through a consistent reduction of the number of smokers in the community and total control of risk factors;. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper.
Pharmaco-economics
Association between chronic obstructive pulmonary disease symptoms and hyperinflation and its impact on exercise and performance. Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trial. Efficacy and tolerability of budesonide/formoterol added to tiotropium in patients with chronic obstructive pulmonary disease.
Efficacy of salmeterol propionate/fluticasone in GOLD stage chronic obstructive pulmonary disease: analysis from the randomized, placebo-controlled TORCH study. Effect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomized controlled trial. Roflumilast in moderate to severe chronic obstructive pulmonary disease treated with long-acting bronchodilators: two randomized clinical trials.
Clearly, as in other countries, there is a very large undiagnosed COPD population in Canada [3]. Despite this, respiratory diseases rank fourth in Canada as a proportion of health care costs [2]. Hidden COPD in Canada is like a tsunami that is gaining strength but has yet to break the shores of Canada's health care system, a system largely unprepared for the enormous stresses that threaten to overwhelm our infrastructure, health care personnel and financial resources.
Health care in Canada is funded by each of our 10 provinces and 3 territories, with some additional federal funding transfers.
Farmacoeconomia
Practice patterns in the treatment of chronic obstructive pulmonary disease in primary care: the CAGE study. Mortality in the 4-year study of Tiotropium (UPLIFT) in patients with chronic obstructive pulmonary disease. In addition, we need to better understand how the severity of COPD and the clinical expression of the disease can influence the cost-effectiveness of comparative treatments.
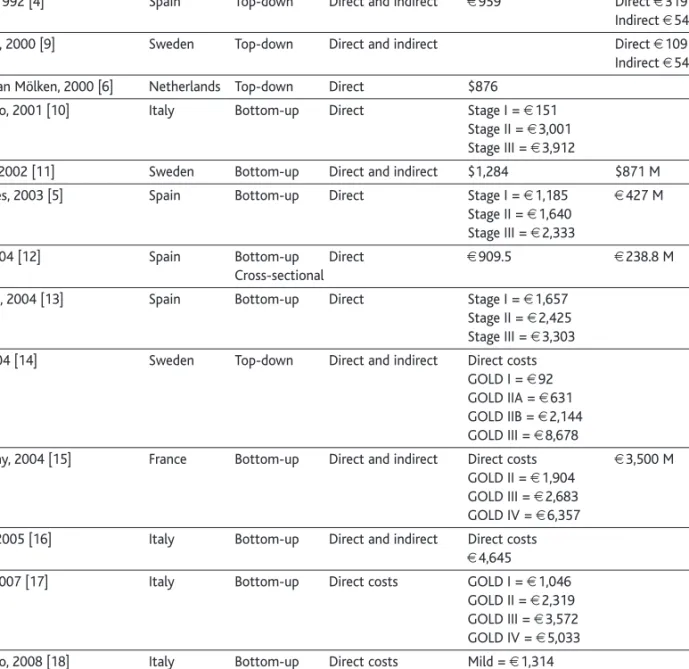
Ipratropium bromide in the management of chronic obstructive pulmonary disease: effect on healthcare costs. Most studies of this type concentrate on the analysis of the costs of the hospital, outpatient and pharmacological treatment related to the disease in question. Despite the observed differences in absolute values between the two types of studies, the distribution of costs was very similar.
If the total direct costs of COPD are divided by the total population of the country, health care for COPD costs each citizen $13.32 per year. Geographical differences in the prevalence and underdiagnosis of COPD: results from the IBERPOC multicenter epidemiological study. Current and future health costs of asthma and chronic obstructive pulmonary disease in the Netherlands.
Costs of chronic obstructive pulmonary disease (COPD) in Italy: SIRIO (Social Impact of Respiratory Integrated Outcomes). Costs of chronic obstructive pulmonary disease (COPD) in Italy: the SIRIO (social impact of respiratory integrated outcomes) study. Clinical and pharmacoeconomic profile of COPD patients with FEV150-60% predicted: pilot study on the impact of the extended indication of ICS/LABA.
Inappropriateness at different steps of COPD management
These staggering statistics make it extremely important to identify risk factors associated with COPD and seek early treatment if symptoms arise. These can be divided into factors responsible for COPD exacerbations and factors responsible for COPD development. Factors responsible for lung function impairment (which already begins during lung function growth), a main feature of COPD, must also be taken into account.
Stopping smoking is the most important thing you can do to prevent or slow down damage to the lungs. In terms of disease progression, other factors of COPD besides direct smoking, which can also influence the course of the disease and its eventual health outcomes as well as the development, include passive smoking (SHS) exposure and occupational exposure [3] . Avoiding conditions that can irritate the lungs can reduce breathing problems in people with COPD.
SHS exposure is an important factor affecting disease severity and health status in COPD [4]. Previous studies suggest that SHS exposure may be a cause of new-onset COPD or reduced lung function. However, the effect of SHS exposure on individuals with established COPD has received little attention.
Because SHS is an modifiable risk factor, clinicians should assess exposure to SHS in their COPD patients and provide advice on how to avoid it.
Inappropriatezza nei differenti passaggi della gestione della BPCO
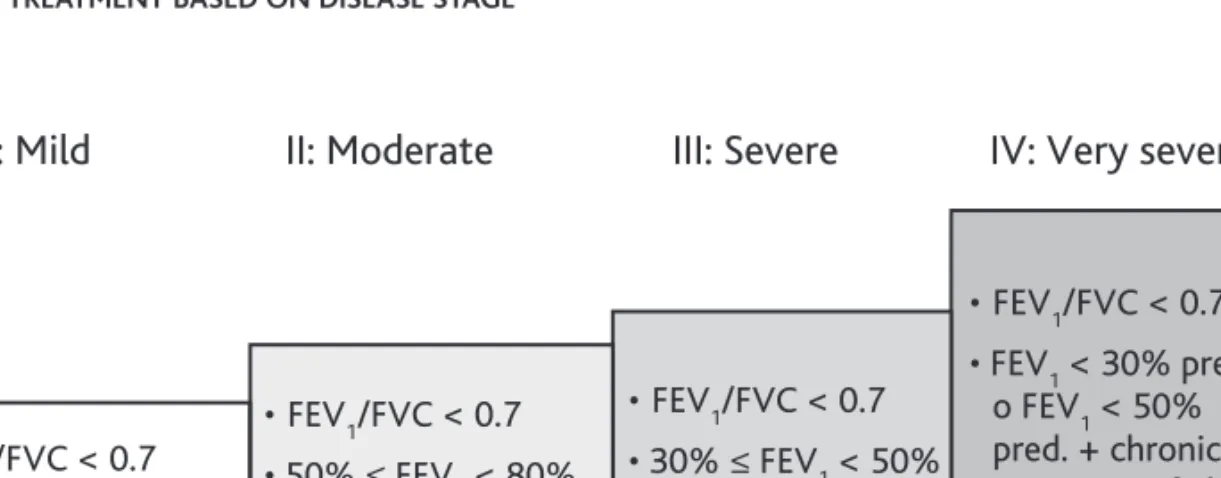
Therefore, in the development of guidelines, efforts should be directed to the screening and selection of interventions with a cost-effective profile. Among lung function parameters, in addition to FEV1/FVC, lung volumes should always be included in the diagnosis of COPD as the assessment of hyper-inflation is an important criterion in the phenotyping of COPD patients. Heart disease, osteoporosis, peripheral muscle weakness and dysfunction, anemia, depression, anxiety, and lung cancer are more common in COPD patients than in the general population.
Recently, there has been concern that the long-term use of inhaled bronchodilators commonly used in the treatment of COPD, including long-acting β2-agonist (LABA) and anticholinergic drugs, may increase the risk of cardiovascular complications. Based on the findings reported in the TORCH trial, Ernst and colleagues reported the results of a nested case-control study in a cohort of nearly 176,000 patients with COPD that examined the use of ICS and the risk of hospitalization for pneumonia . Indeed, in the initial evaluation and follow-up of the patients included in NETT, it became clear that a very low FEV1 and diffusing capacity for carbon monoxide (DLCO) were associated with a very poor outcome.
Low lung function and incident lung cancer in the United States: data from the First National Health and Nutrition Examination Survey. Indeed, after an emergency department visit for an exacerbation of COPD, there is a high probability that a new episode will occur in the first 2 weeks after discharge [3,4]. Available data suggest that an early rehabilitation intervention should be included in the follow-up program.
The explanation can be sought in the heterogeneity of the underlying genetic changes, as well as in the diversity of specific cell targets.
A new decade of COPD
A multivariate model for predicting relapse after outpatient treatment of decompensated chronic obstructive pulmonary disease. Factors associated with frequency of emergency department visits for chronic obstructive pulmonary disease exacerbation. Respiratory rehabilitation after acute exacerbation of COPD can reduce the risk of readmission and mortality: a systematic review.
Striking new evidence regarding the pathogenesis of COPD (especially emphysema) relates to its proposed inclusion in the category of diseases with "premature aging" of the lungs, based on strong similarities with diseases characterized by telomere and stem cell dysfunction [2-4] . In the lungs, telomere erosion can variably affect the renewal potential of different stem cells, thus causing a progressive depletion of relevant parenchymal components, which eventually culminates in alveolar loss and functional abnormality. Interestingly, evidence is accumulating that also idiopathic interstitial pneumonia (IPF) can be included in the pathological category of diseases characterized by "telomere dysfunction" [5-7].
Tobacco smoke is a key pathogenic element in both COPD and IPF and may serve as an environmental co-factor for the development of both diseases [ 5 ]. But how can this proposed similarity between the basic pathogenic mechanisms underlying COPD and IPF be reconciled with the apparent diversity of their pathological and clinical presentations. Thus, in COPD, abnormal apoptosis, aging and loss of function mainly affect cells involved in the production of extracellular matrix proteins (elastin, fibronectin, etc.), with eventual weakening of the mesenchymal structure of the alveoli, leading to a defect. in tissue reserve and "disappearance" of the supporting scaffold for epithelial cells.
In conclusion, this evolving scenario opens up new possibilities for a better understanding of the pathogenic mechanisms of COPD and also of IPF, and may open new perspectives for alternative treatments of these devastating diseases that act on either pharmacological protection or specific replacement of the affected diseases. stem cells [10].
Una nuova decade per la BPCO
Population aging together with lifestyle changes are key factors explaining the increasing prevalence of chronic conditions, which is expected to continue over the next decade, leading to further dysfunctions in health systems worldwide [1-3]. From crisis management to integrated care A recent analysis of the burden of all chronic conditions on hospitalizations in tertiary care [10] pointed to the need to review management aspects of worsening chronic patients with a broad scope, aiming not only to increase the efficiency of care during exacerbations, but also prevention of hospitalizations due to severe exacerbations in weak patients. In view of the high social and economic burden generated by hospitalization of patients with chronic conditions, new care modalities have been developed in recent years that aim to reduce hospitalizations through patient empowerment and the implementation of alternatives to conventional hospitalization [11-12 ].
There is no doubt that the current fragmentation between levels of care and community services is a major limiting factor for the practical application of the principles formulated in the Chronic Care model. The ultimate goal should not be limited to management aspects, but should be to achieve positive modulation of chronic disease prognosis. Expanded Rollout of Integrated Care Service NEXES is the acronym of the project “Supporting Healthier and Independent Living for Chronic Patients and Elderly” designed to address the transition phase from existing pilot experiences to the rollout of health/social services targeting selected patient groups .
NEXES will mainly address patients with one or more of the following chronic conditions: COPD, chronic heart failure and type II diabetes. One of NEXES' primary goals is to provide robust results to health technology assessment agencies and policy makers to facilitate the widespread deployment of the services and the sustainability of the care model. Casas A, Troosters T, Garcia-Aymerich J, Roca J, Hernández C, Alonso A, del Pozo F, de Toledo P, Antó JM, Rodríguez-Roisín R, Decramer M; members of the CHRONIC Project.
The therapeutic challenge presented by COPD is due to the need to target all components of the disease.