Objective: Our objective was to identify, characterize, evaluate and organize the current, available evidence that represents existing recommendations and suggestions for the prevention of re-traumatization during the treatment of physical illnesses of survivors of torture in health services. The exact prevalence of torture is unknown, but a significant number of asylum seekers and refugees are torture survivors (Ostergaard et al., 2020). A comprehensive review of relevant research in this area is essential before engaging in a meaningful discussion about how to minimize the re-traumatization of torture survivors during treatment in physical therapy wards.
How strong is the evidence on the treatment of torture survivors in somatic health care, with recommendations to prevent re-traumatization.
Quality Included Records Assessment
This process is illustrated in the results section with the subheading "Themes." To condense the text in the results section and the tables, all included records were numbered from 1 to 40 as shown in the appendix. 10 assessed using the Evaluation of Guidelines Research and Evaluation (AGREE) Instrument, Version II (AGREE II). To ensure a standardized approach, the reviewers (ACS and AKB) completed the AGREE II online training tutorials before conducting the quality assessment (Brouwers et al., 2016).
For the CPGs, a quality score was calculated for the AGREE II (described in Figure S1) six domains using the formula presented in the AGREE II user manual (Brouwers et al., 2010).
Results
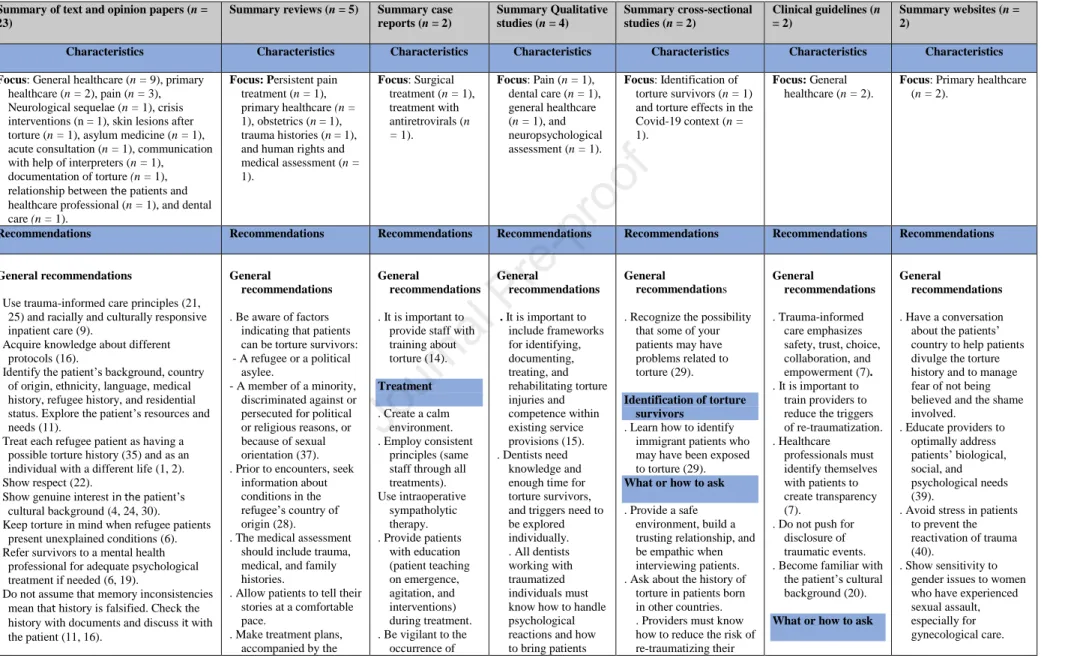
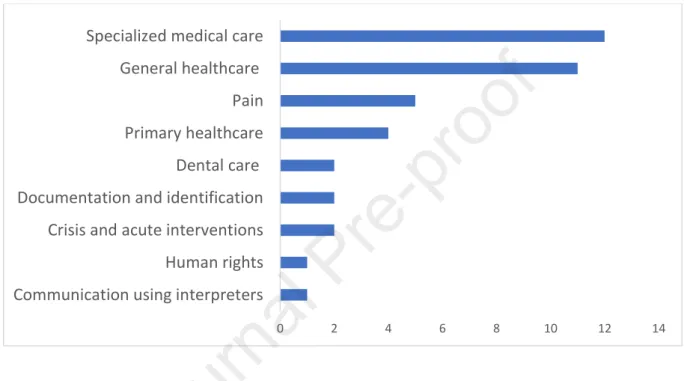
Characteristics of the Included Studies
- Characteristics of Text and Opinion Statements
- Characteristics of the Reviews
- Characteristics of the Case Reports
- Characteristics of the Qualitative Studies
- Characteristics of the Cross-Sectional Study
- Characteristics of the Guidelines
Cultural competence, sensitivity and the importance of using an interdisciplinary team to treat torture survivors are also portrayed as important (2). One study (29) using 121 patients focused on the identification of torture survivors among a general patient population. Summary of characteristics of the included studies and the quality of the themes that emerged.
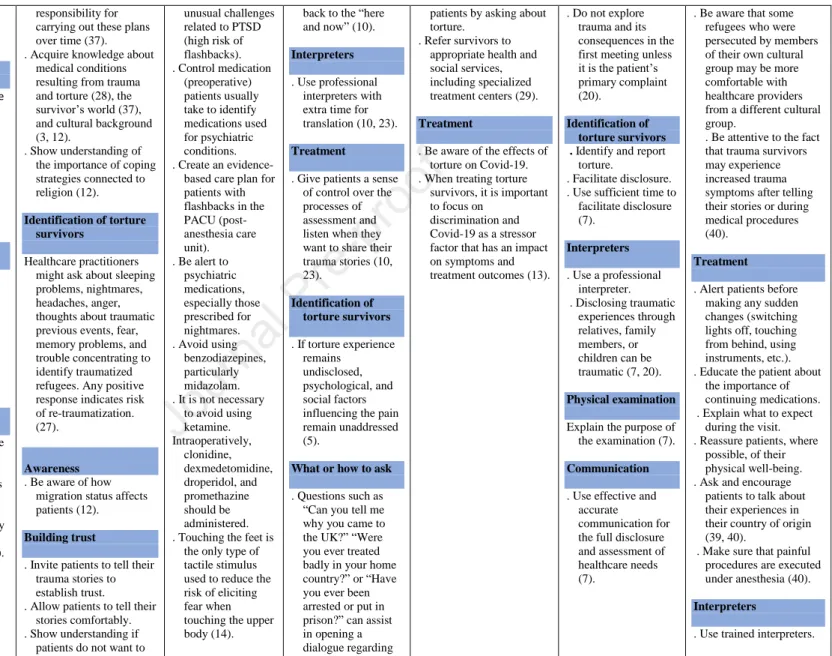
Identify the patient's background, country of origin, ethnicity, language, medical history, refugee history, and residential status. Do not explore the trauma and its consequences during the initial consultation unless it is the patient's primary complaint (20). Pay attention to indirect communication, ask for expressions, tropes and metaphors you do not understand, and talk about the patient's country of origin and exile or different cultures within one country to relax them (24).
In torture survivors, EFV should be used with ZDV, effective antiretroviral treatments, after an appropriate discussion between the patient and provider about this medication's possible role in exacerbating PTSD symptoms (18). To reduce flashbacks, create a calm atmosphere, provide detailed explanations of planned procedures, obtain informed consent, and facilitate the patient's control over procedures (31). Be aware of the possibility that doctors who have participated in torture may be a cause for distrust and discuss this with patients.
Moderate concerns regarding overall methodological quality → two studies with minor concerns: It is unclear whether opinion sources have a reputation for expertise (25, 34). Moderate concerns regarding overall methodological quality → one study with minor concerns in which it is unclear whether the likelihood of publication bias has been assessed (3). Minor concerns regarding overall methodological quality → one study with moderate concerns (it is unclear whether the.
Minor concerns with methodology → in one study it is unclear whether there were strategies to deal with the stated confounding factors (13).
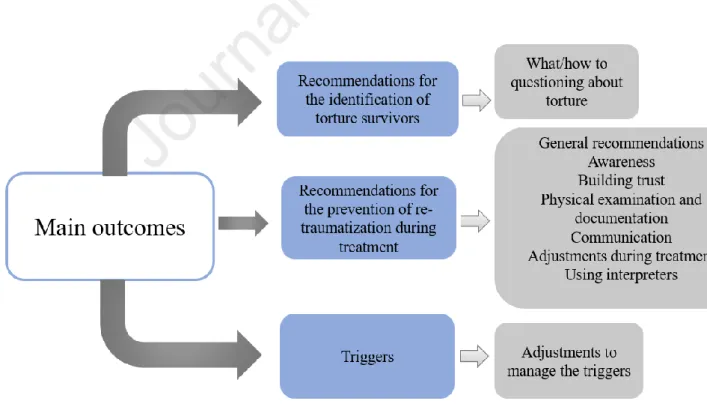
Themes
- Recommendations for Preventing Re-Traumatization During Treatment
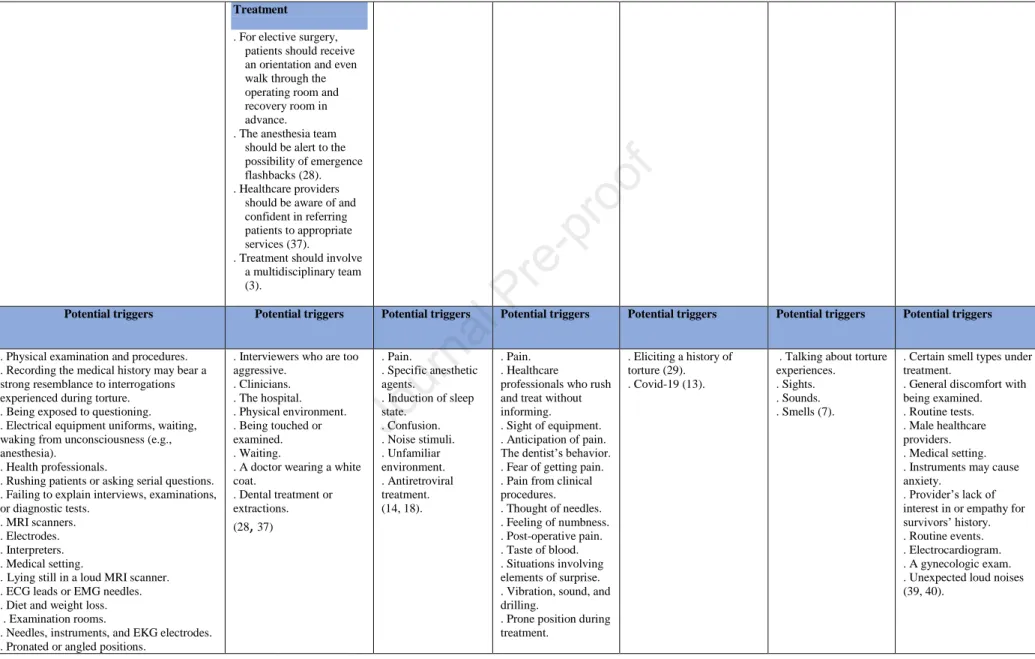
- Potential Triggers and Recommendations for Managing Triggers
Healthcare personnel should be educated about torture and its consequences in order to understand which situations, objects or aspects of interaction can trigger re-traumatisation. For clinical interviews, survivors should be assessed individually (34) in a comfortable environment with adequate time if necessary. Torture and related trauma should be considered health issues by healthcare providers, and torture should be considered in patients with unexplained mental, skin, neurological or orthopedic conditions.
Patients should be referred to a mental health professional for psychological evaluation and therapy as needed. When interpreters are present, doctors need to be aware of potential shortcomings, but when the interpreters are fellow citizens, confidentiality issues can arise. Somatic problems can worsen with new stress, so they should be evaluated as both psychological and somatic.
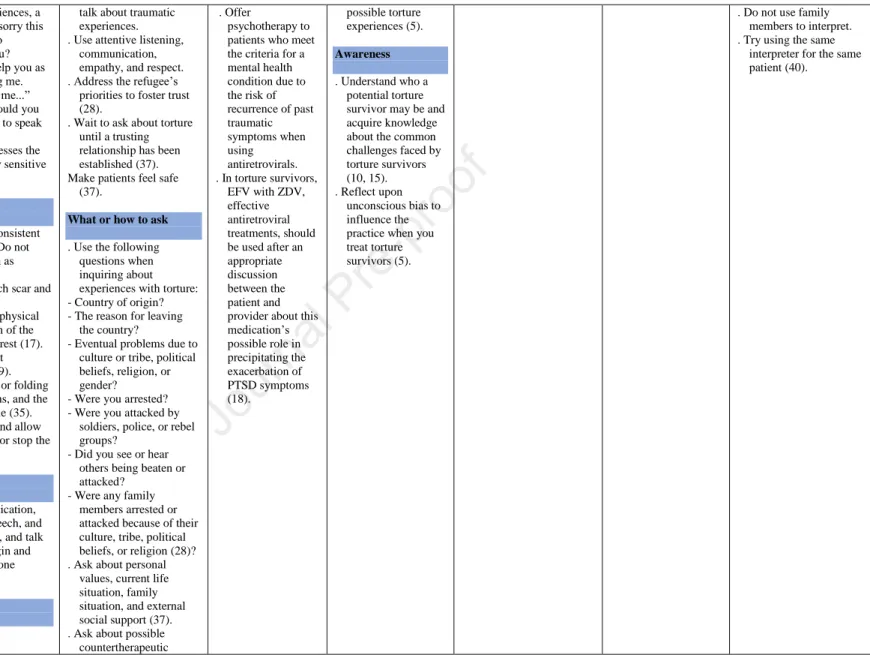
The anesthesia team and nurses should be wary of the occurrence of flashbacks. 30 Patients who meet the criteria for a mental disorder and require antiretroviral therapy should be offered psychotherapy because of the potential for recurrence of PTSD symptoms. Effective antiretroviral drugs should be offered to torture survivors after exact information and conversation with patients about the potential role of the medication in increasing PTSD symptoms.
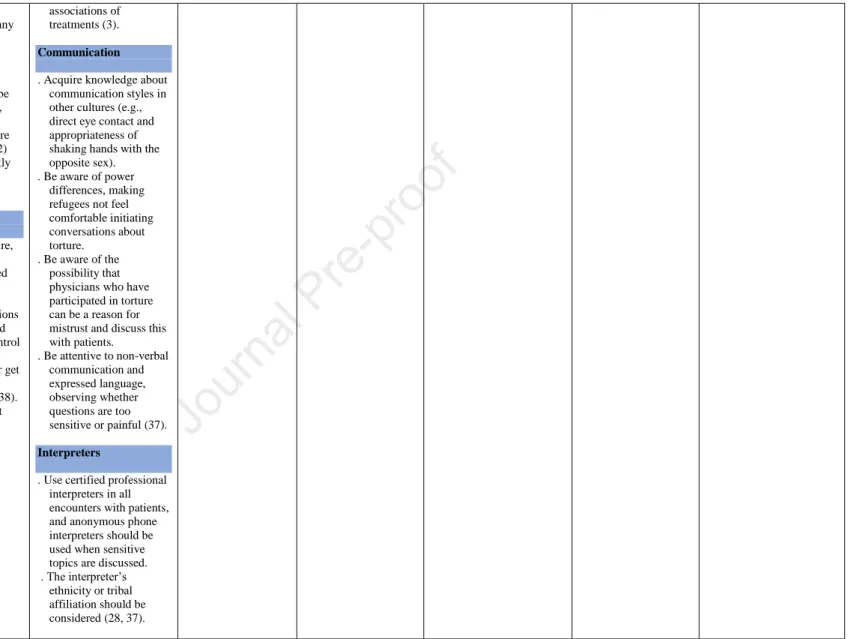
According to the recommendations, bilingual clinicians or certified professional interpreters should participate in encounters with patients with a history of torture to maximize the quality of clinical encounters and reduce the risk of poor treatment outcomes. Interpreters are also subject to the principle of confidentiality, so both healthcare providers and interpreters must be careful when dealing with sensitive topics.
Discussion
Since the clinical context is important for the phenomena of retraumatization (Schock and Knaevelsrud, 2013), providing case study research on torture survivors' experiences of retraumatization during treatment could provide us with vital information on the subject. 36 With an extensive search strategy, this mapping overview covers an important part of the publications within the healthcare sector for torture survivors. This effect may be related to the organizational system in these countries where the treatment of torture survivors is delegated to specialized centers, which also produce the necessary research (Moa Nyamwathi Lønning, 2020).
This small number indicates that torture survivors are underrepresented in studies of treatment in somatic sections and retraumatization. Many torture survivors move around, between and within countries, in search of safety, work and educational opportunities, indicating that researchers can make greater efforts to include survivors in research (Gabriel et al., 2017) so that their voices are also represented in studies is focusing on retraumatization during treatment in somatic health care departments. Furthermore, problems with sampling can create significant biases in the results presented in evidence about our understanding of torture survivors.
There may also be a need for a greater focus on this topic, which supports research into the somatic treatment of torture survivors. According to the evidence from this review, healthcare providers' successful identification of patients who are torture survivors enables them to prepare for patients' treatment and prevent re-traumatization. Managing triggers is an important aspect of preventing torture survivors' re-traumatization during treatment, and almost all included studies discuss potential triggers and communicate suggestions for their effective management.
Thus, healthcare providers must constantly weigh the pros and cons of using interpreters when treating torture survivors. Providing quality healthcare to torture survivors begins with an awareness of a patient's history of torture (Ahrenholz et al., 2015; Mollica, 2004).
Strengths and Limitations
Nevertheless, in the guidelines included in this review, domain scores are higher than 50% (69% and 56%), raising moderate concerns about the ones presented. In terms of assessing the risk of bias, the included studies appeared to be reliable. This is consistent with findings in a systematic review reporting that, while the term is widely used, it is not well understood how to apply the concept in everyday clinical practice (Raja et al., 2015).
As a result, studies from different geographic regions around the world focused on torture survivors were included. Most of the studies were texts and opinions and while these were prepared by experts in the field, the voices of survivors were not as represented. More research on the perspectives and experiences of torture survivors who are retraumatized during treatment is needed in the future to better understand this patient group.
To complement the propositions presented in this mapping review, more studies are needed that present the health care aspects and challenges of providing re-traumatized health services for victims of torture. The included studies provide some recommendations on how to handle situations in which a history of torture is inconsistent with clinical findings or when patients are unwilling to share theirs. As a result, recommendations on how to address inconsistencies in the information provided by victims of torture may be a priority for guideline development.
In parallel with this proposal and considering the presented challenges related to torture survivors' reduced trust in healthcare providers together with challenges related to losing control during treatment, more suggestions are needed on how to attend to their special needs during perioperative treatment with general anesthesia . Future studies are required to contextualize the guidance in the literature to prevent re-traumatization of torture survivors in healthcare settings.
Conclusions
Effects of torture in the context of COVID-19 and variants of continuing trauma type III: peri-post trauma mental health syndrome type III in survivors of torture in Syria. The role of doctors in the investigation, prevention and treatment of torture. care practices for refugee and immigrant youth: 10 clinical gems. Prevalence of torture and trauma history among immigrants in primary care in Denmark: are general practitioners asking questions.
Rehabilitation of torture survivors and prevention of torture: Priorities for research through a modified Delphi survey. Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. 6 Clarysse et al., 2019 Skin lesions, differential diagnosis and practical approach for potential survivors of torture.
7 Cohen and Green, 2022 Quality standards for healthcare professionals working with victims of torture in detention. 12 Kassam, 2019 Understanding experiences of social support as coping tools among immigrant and refugee women with postpartum depression: an integrative literature review 13 Kira et al., 2022 The Effects of Torture in the Context of COVID-19 and. 15 Lønning et al., 2021 “A random system”: The organization and practice of torture rehabilitation services in Norway.
26 Worm, 2004 Documentation of Torture - Methods and Concepts 27 Zander et al., 2015 Development of an interview guide that highlights the. 29 Eisenman et al., 2000 Survivors of torture in a general medical setting: how often have patients been tortured and how often is it missed. 35 Grodin, 2004 Caring for survivors of torture and refugee trauma in the United States and Portugal.
37 Quiroga and Jaranson, 2005 Politically motivated torture and its survivors 38 Wenzel et al., 2007 Torture survivors.