Dissemination
Thepreviouschapterlookedattheproblemsassociatedwiththepresentationofincidentreports. It
wasarguedthattheformatandstructureofthesedocumentsmustbetailoredsothattheysupport
theirintendedrecipients. Itwasalso arguedthatcaremustbetakentoensurethat therhetoricis
notusedtomaskpotentialbiasinanincidentreport. Thischaptergoesontoexaminetheproblems
that areassociated withthe disseminationof thesedocuments. Itis of littlebenetensuringthat
reportsmeetpresentationguidelinesiftheirintendedrecipientscannotaccesstheinformationthat
they provide. There are signicant problems associated with such dissemination activities. For
example,theFDA'sMedical Bulletinthat presentsinformationabouttheirMedWatchprogram is
currentlydistributed to 1.2million healthprofessionals. Later sections analysethe ways in which
manyorganisationsareusingelectronicmediatosupportthedisseminationofincidentreports. This
approach oers many advantages. In particular, the development of the Internet and Web-based
tools ensures that information can be rapidly transmitted to potential readers across the globe.
There are, however, numerous problems. It can be diÆcult to ensure the security and integrity
of information that is distributed in this way. It can alsobe diÆcult to help investigatorssearch
throughthemanythousandsofincidentsthatarecurrentlybeingcollectedinmanyofthesesystems.
Theclosingsectionsofthischapterpresentarangeoftechniquesthatareintendedtoaddressthese
potentialproblems.
14.1 Problems of Dissemination
Chapters 11.5and 12.4 havealready described someof the problems that complicate thedissem-
inationof informationaboutadverse occurrencesand near miss incidents. Forexample, itcanbe
diÆculttoensurethatinformationismadeavailableinapromptandtimelyfashionsothatpotential
recurrencesareavoided. It can alsobediÆcultto ensurethat safetyrecommendationsreachall of
themanydierentgroupsthat mightmake useof this information. The followingpages build on
thesepreviouschapterstoanalysethesebarrierstodisseminationin greaterdetail.
14.1.1 Number and Range of Reports Published
It is important notto underestimate the scaleof the task that canbe involvedin thedissemina-
tion of incident reports. Even relatively small, local systems can generate signicant amounts of
information. Forinstance,oneoftheIntensivecareUnitsthat wehavestudiedgeneratedatotalof
111recommendationsbetweenAugust 1995and November1998. 82 of these were `Remind Sta'
statements. The29 other recommendations concerned the creationof new procedures orchanges
toexistingprotocols(e.g. `produceguidelinesforcareofarteriallines'),orwere equipmentrelated
(e.g. `Obtainspareheliumcylinderforaorticpump tobekeptinICU').
As one might expect the task of keeping sta and management informed of recent incidents
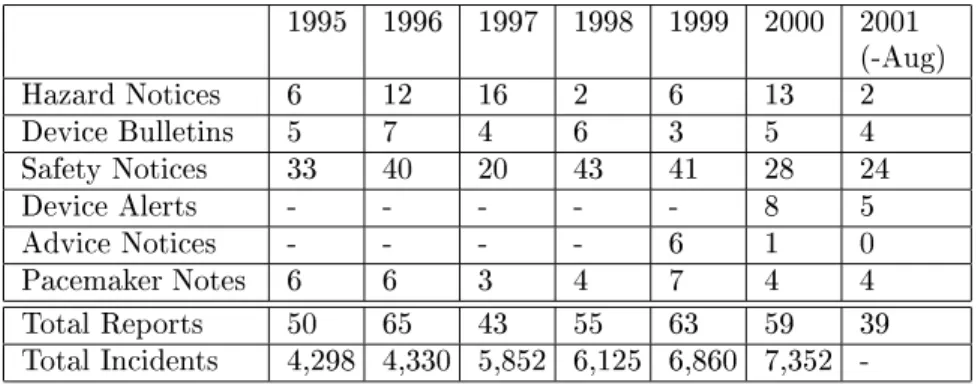
andrecommendations issignicantlymorecomplexin nationaland internationalsystems. This is
illustratedbyTable14.1,whichpresentsthetotalnumberofdierentreportsthatwerepublishedby
1995 1996 1997 1998 1999 2000 2001
(-Aug)
HazardNotices 6 12 16 2 6 13 2
DeviceBulletins 5 7 4 6 3 5 4
SafetyNotices 33 40 20 43 41 28 24
DeviceAlerts - - - 8 5
AdviceNotices - - - - 6 1 0
PacemakerNotes 6 6 3 4 7 4 4
TotalReports 50 65 43 55 63 59 39
TotalIncidents 4,298 4,330 5,852 6,125 6,860 7,352 -
Table14.1: AnnualFrequencyofPublicationsbytheUKMDA
theUKMedicalDevicesAgency(MDA)overthelastveyears. Itshould benotedthatthegures
for 2001are currentlyonly available until August. As we haveseen from the Maritime examples
in the previous chapter, incident reporting agencies produce a range of dierent publications to
disseminatetheirrecommendations. InTable14.1,hazard noticesarepublishedfollowingdeathor
seriousinjuryorwheredeathorseriousinjurymighthaveoccurred[543]. Amedicaldevicemustalso
beclearlyimplicatedandimmediateactionmustbenecessarytopreventrecurrence. Devicebulletins
addressmoregeneralmanagementinterests. Theyarederivedfrom adverseincidentinvestigations
and consultation with manufacturers orusers. They are also informed by device evaluations. In
contrast,safetynoticesaretriggeredbyless`serious'incidents. Theirarepublishedincircumstances
wherethe recipients'actionscan improvesafetyorwhere itis necessaryto repeatwarningsabout
previous problems. Device alerts are issued if there is the potential for death or serious injury
particularly through the long term use of a medical device. Finally, Pacemaker Technical Notes
publish information about implantable pacemakers, debrillatorsand their associatedaccessories.
Forthepurpose ofcomparison,Table14.1alsocontainsthetotalnumberofadverseincidentsthat
were reported in the MDA's annual reports [540]. As canbe seen, there has been a gradual rise
inthefrequencyof incidentreports whilethetotalnumberofpublicationshasremainedrelatively
stable. Such an analysismust, however,bequalied. Thetotal incidentfrequencies arebased on
the MDA's reporting year. Hence the gure cited for 1996 is, in fact, that given for 1996-1997.
However,thenumberofreportsandassociatedpublicationsprovidessomeindicationofthescaleof
thepublicationtasksthat confrontorganisationssuchastheMDA.
1997 1998 1999 2000 2001
(-Aug)
SafetyAlerts 55 55 54 67 38
DrugLabeling 239 519 512 505 241
BiologicsSafety - 24 10 29 14
FoodandAppliedNutrition 3 2 2 2 2
Devicesand Radiology 9 12 9 4 3
Table14.2: AnnualFrequencyofPublicationsbytheUSFDA'sMedWatch Program
ThelevelofactivityindicatedinTable14.1ismirroredbytheguresinTable14.2. Thispresents
publicationgures forthe US Food and DrugAdministration's MedWatch initiative. This Safety
Information andAdverse EventReporting Programme is intendedto `servesbothhealthcare pro-
fessionalsandthemedicalproduct-usingpublic'[272]. Itcoversabraid rangeofmedicalproducts,
`includingprescriptionand over-the-counterdrugs,biologics,dietary supplements,and medicalde-
vices'. It,therefore,hasaslightlywiderremitthanthatoftheUKMDA.TheprimaryMedWatch
publicationprovidesSafetyAlertsaboutdrugs,biologics,devicesanddietary supplements. Ascan
groupswithintheFDA. Itpublishessafety-relateddrug labelingchangesummariesthat havebeen
approvedbyFDACenterforDrugEvaluationandResearch. Italsoincorporatesrecalls,withdrawals
andsafetyissuesidentiedbytheCenterforBiologicsEvaluationandResearch. Theprogramalso
publishesselected warnings and other safetyinformation identied by the Center for Food Safety
and Applied Nutrition. Finally, the Medwatch initiative incorporates safety alerts, public health
advisoriesandnoticesfromtheCenterforDevicesandRadiologicalHealth. Wehavenotcalculated
totalsfor Table14.2 aswedid for Table 14.1because of theinherent diÆculty of calculating the
frequency of recommendations to change drug labelling in the FDA adverse event reporting pro-
gramme. Some drugs form the focus of several reports in the same year. Recommendations can
be applied to aparticular generic named product orto thedierentbrands of that product. We
havechosentocalculate frequenciesonthebasisof nameddrugs identiedin theCenterforDrug
EvaluationandResearchwarnings.
It is alsoimportant to stressthat the reports identied in Tables14.1 and14.2 onlyrepresent
a small subset of the publications that the FDA and the MDA publish in response to adverse
incidents. For instance, the MedWatch programme alsodisseminatesarticles that are intendedto
supportthecontinuingeducationofHealthcare professionals. Theseinclude informationaboutthe
post-marketingSurveillanceforAdverseEventsAfterVaccinationandtechniquesforassuringdrug
quality. TheFDAalsoprovidesmoreconsumerorientedpublicationstoencouragecontributionsfrom
thegeneralpublic. Itusesincidentinformationtoaddressspecicconsumerconcerns,forinstancein
specialreportsondrugdevelopmentandtheinteractionbetweenfoodanddrug. Thewidescopeof
thesepublicationactivitiesisalsoillustratedbytheUserFacilityReportingBulletins. Thisquarterly
publicationisspecicallytargetedathospitals,nursinghomesand`deviceuserfacilities'.
Dissemination activitiesare not onlyfocussedon the generation of specic incidentreports or
articlesonmoregeneralissues. Theyalso include theorganisationofworkshops,such asthe1998
meetingon `MinimisingMedicalProductErrors'[263]. TheUKMDA hostsimilarevents,suchas
their annual conference which in 2001 will address the theme `Protecting Patients - Maintaining
Standards'[546]. The MDA also holds morefocussedstudy days. These providesta trainingto
addresscommonproblemswithparticulardevices. Forexample,theMDAsetuparecentmeeting
fornursesonbest practiceandthepotentialpitfalls inoperatinginfusionsystems[544].
14.1.2 Tight Deadlines and Limited Resources
Thepreviousparagraphsillustratethehigh frequencyand thediversityof disseminationactivities
that are conduced by many incident reporting organisations. It is diÆcult to under-estimate the
logisticalchallengesthat such activitiescanimpose uponnite resources. There isalso increasing
pressure in many sectors to increase the eÆciency of many reporting bodies. For instance, one
governmentmeasureestimatesthat theMDA managedto increaseitsoutputby 9%withastable
workforcebetween2000-2001.Thesepressurescanalsobeillustratedbysomeoftheobjectivesbeing
promotedbytheMDA. For 2001-2002,itis intendedthat allHazardNoticeswill beissuedwithin
20workingdays;90%ofSafetyNoticeswillbeissuedwithin60daysand75%within 50days. Itis
alsointendedtoincreasethenumberofadverseincidentreportsthatwillbepublishedbyafurther
9%while atthesametimemaking`eÆciency'savingsof2%[540].
Theresultsoftightnancialconstraintscanalso beseenin themanner inwhichthe FDA has
altered it's publication policy in recent years [868]. Previous sections have mentioned the User
FacilityReportingBulletin,thispublicationisintendedforhospitals,nursinghomesandotherend-
userfacilities. Theinitial twenty, quarterlyissues ofthe Bulletinwereprintedin theconventional
mannerandwerepostedtoanyorganisationthatrequestedacopy. Atitspeak,77,000subscribers
received copies of these documents that presented summarised reports based on recent incident
reports. Budgetary restrictions forced the FDA to review this policy. In Issue 17, readers were
askedto respond to aretentionnotice. If they didnotrespondthen theywere removed from the
distributionlist. It was hoped that the high initial administrative overhead associated with this
initiativewouldyieldlonger termsavingsin distribution costs. By1999,however,Federalfunding
cutspreventedanydistributioninpaperform. Thetwenty-rstissueoftheBulletinwas,therefore,
theirfeelingsaboutthis situation;`weregretthe needto moveto this newtechnology ifit means
thatmanyofourcurrentreaderswillnolongerhaveaccessto theBulletin' [868].
Thejointpressuresimposed bythe needto disseminate safetyinformation in a timely fashion
andtheneedto meettightnancialobjectiveshasresultedin anumberof innovations in incident
reporting. Manyof thesesystemsstartwith thepremisethat itis impossibletoelicit and analyse
voluntaryincidentreportsacrossanentire industry. Evenwithmandatoryreportingsystemsthere
will be problemsof contribution bias that resultin a verypartial viewof safety-related incidents.
Theseproblemsstempartlyfromthecostandcomplexityoflargescalevoluntaryreportingsystems.
Theyalsostemfromthepassivenatureofmostmandatorysystemsthatsimplyexpectcontributors
tomeettheirregulatoryrequirementswhenrespondingtoanadverseoccurrence. Aswehaveseen,
evenifapotentialcontributorwantstomeetareportingobligationtheymayfailtorecognisethata
safety-relatedeventhasoccurred. Mostregulatoryandinvestigatoryorganisationslacktheresources
necessarytotrainpersonnelacrossanindustrytodistinguishaccuratelybetweenreportableandnon-
reportableevents. Similarly,therearesignicantnancialbarriersthatpreventroutineinspections
andauditstoreviewcompliance.
Sentinel reporting systemsprovidean alternative solutionthat is intended to reduce the costs
associated withincident reporting and, therebyensure that recommendations aredisseminated in
atimely fashion. This approach identies a sample of all of the facilitiesto be monitored. This
siteswithinthesamplearethenoeredspecialisttraininginbothmandatoryandvoluntaryincident
reporting. The incidents that are reported by these sentinel sites can then form afocusfor more
generalsafetyinitiativesacrossanindustry. Theseideasareextremelysuasivetomanygovernmental
organisations. Forinstance,theFDAModernisationAct(1997)requiredthattheFDAmakeareport
to Congressin late 1999aboutprogresstowardssuch asentinelsystem [264]. InSeptember 1996,
CODAInc. wasawardedacontracttoconductastudytoevaluatethefeasibilityandeectivenessof
asentinelreportingsystemforadverseeventreportingofmedicaldeviceuse. Theexplicitintention
wasto determinenotwhether asentinelsystemcouldsupplementpassive,voluntarysystems,such
asMedWatch, but to replace them entirely. Thetrial ranfor twelve months and the nal report
emphasised the importance of feedback and dissemination in the success of any sentinel system.
The CODA trial provide several dierent forms of feedback. These included a newsletter, faxes
ofsafety notices, responses to questions presentedby StudyCoordinators. The individualreports
that were received bythe projectwere summarised,anonymised andthen published in bimonthly
newslettersforStudyCoordinators. ThesecoordinatorsactedasaneÆcientmeansofdisseminating
safetyrelatedinformationwithin thesamplesites.
This projectnothasimportantimplications forthe eÆcient disseminationof safety-relatedin-
formation. It also provides important insights aboutthe practical problems that can arise when
attempting to ensure the timely dissemination of incident recommendations and reports. Many
reportingsystemsendeavourtoensurethatoperators,safetymanagersandregulatorsareprovided
with information about incidents accordingto a sliding timescale that reects the perceived seri-
ousnessof theincident. This is thecase withthe MDA targets, cited above. It can, however,be
extremelydiÆculttoestimatetheseriousnessofanincident. Previouschaptershavereferredtothe
`worst plausible outcome' that is often invokedto support such assessments. The practical prob-
lemsofapplying such heuristicscanbeillustratedbytheCODA pilotstudy. Theprojectanalysts
determinedthat only 14%ofthe reports received would havebeenclearlycoveredby theexisting
mandatorysystems. 56%ofthereportsdescribedlessseriousincidentsthatfellwithinthevoluntary
reporting provisions. 30%of all submission, or96 reports, fell between these twocategories; `the
determinationofseriouspatientinjuryaccordingtoFDA'sdenitionwasdiÆculttomake'. Ofthese
96,60%weresubmittedonvoluntaryforms. 25%ofthereportsclearlydocumentingseriouspatient
injuryalso were submittedon voluntary forms. If these resultsprovidean accurate impression of
thetrueseverityof the incidentsthen theyindicate that analystscannot acceptthe contributors'
severityassessmentsatfacevalue. Twoseniornurse-analystsagreedtoreviewallreportsandclassify
themurgencyusingascaleof: veryurgent,urgent,routinemonitoring,well-knownproblemornot
important. Approximatelyone-third(113) were classiedasveryurgentorurgent. Of these, only
19were clearlymandatory reports. This is asignicant concerngiventhat distribution deadlines
Theresultsof thisanalysis canbepresentedin anotherway. As mentioned,14%ofallreports
clearly fell within the existing mandatory systems. About half of these, according to the nurses'
analysis,neededonlyroutinemonitoring. TheFDAcitetheexampleofa`problemwithacatheter
in which there was medical intervention, but for which FDA already had taken action, so that
additionalreportswouldnotmakeaveryvaluablecontributiontotheagency'[264]. However,50of
the175reports thatfell under voluntaryreporting ruleswererated asveryurgentorurgent. This
creates considerable problems for the prompt dissemination of safety-relatedinformation. Delays
in aregulatoryresponse donotsimply stemfrom thetime requiredto analyseareport and make
recommendations. Theyalso stemfromtheamountoftime that ittakesacontributorto actually
gleareportintherstplace. Someofthecontributorscomplainedaboutthetimelimitsthatwere
recommendedforreportingparticularclassesofincidents. Insomecases,whatcontributorsclassed
aslesssevereoccurrenceswentunreportedformorethan tendays. Thepreviousparagraphshave
questioned thereliabilityof suchseverityassessmentsand so it seemslikelythat such delaysmay
beasignicantfactorin ensuringtheprompt disseminationofalertsandwarnings.
14.1.3 Reaching the Intended Readership
Chapter12.4arguedthatthetaskofdraftingincidentreportsiscomplicatedbythediversereader-
shipsthatthesedocumentscanattract. Thissectionextendsthisargument. Thediversereadership
of these documents not only complicates the drafting of an incident report but also exacerbates
theirdissemination. There isan immediateneed to ensurethat individuals within aworking unit
areinformedof anyrecommendations followinganincident. Chapter 4.3argued that such actions
are essential to demonstrate that contributions are being acted on in a prompt manner. In par-
ticular,reportsshould be sentto the individuals whoinitially provided notication of anadverse
occurrence. These requirement apply to the dissemination of incident reports in both large and
smallscale systems. National and internationalschemes face additionaldistribution problems. In
particular,incidentreportsmustforwardedtoother `atrisk' centres. Thisis anon-trivialrequire-
ment because it can often be diÆcult to determine precisely which centres might be aected by
anypotentialrecurrence. Within these associatedworking groups,itis importantto identify who
will assume responsibility for ensuring the reports are read by individual members of sta. This
caninvolvecloseliaisonbetweentheinvestigatorswhodraftareportandsafetymanagersorother
seniorstadistributedthroughouttheirorganisation.
It is possibleto identify anumberof dierent dimensionsthat characterise thedistribution of
incident reports. The following list summarises these dierent dimensions. Particular reporting
systemmaytailortheapproachthattheyadopt accordingtothenature oftheincident. Theymay
alsouse hybridcombinations ofthese techniques. Forexample,aclosed distribution policy might
be exploited within the organisation that generate the report to ensure that information wasnot
prematurelyleakedtothemedia. However,ahorizontalapproachmightalsobeusedtoensurethat
keyindividualsinothercompaniesarealsomadeawareofapotentialproblem:
Closeddistribution.
Thisapproachrestrictsthedisseminationofincidentreportstoafewnamedindividualswithin
anorganisation. Thiscreatesconsiderableproblemsinensuringthatthoseindividualsandonly
those individualsactually receivecopies ofareport. It isalso importantto note throughout
this analysis that the receipt of areport doesnot implythat it will be either read oracted
upon.
Horizontaldistribution.
This approach allows the dissemination of incident reports to other companiesin the same
industry. Thedistributionmaybefurthertargetedtothoseorganisationsthatoperatesimilar
applicationprocesses.
Verticaldistribution.
This approach allows thedissemination of reports to companies that occurwithin thesame
downthesupply chainto ensurethat companies, which relyontheproducts andservices of
thecontributororganisation,are alteredtoapotentialproblem. Supplycompaniesmay also
beinformed if anincident occurs as theresult of problems at previous stages in the supply
chain.
Parallel distribution.
Thisapproachensuresthatreportsaredistributedtocompaniesinotherindustriesthatoperate
similar processes. For example, incidentsinvolving thehandling and preparation of nuclear
materialscanhaveimplicationsin thedefence,medicalandpowergenerationindustries. It is
for this reasonthat organisations such as theUS Chemical Safety and Hazard Investigation
Boardweresetuptospanseveralrelateddomains.
Open distribution.
This approach allowsthe freedistribution ofincident reports. Increasingly,this approach is
beingadoptedbyregulatoryorganisations,includingtheFDAandMDA,andbyindependent
research organisations, such asthe NHS Centre for Reviews and Dissemination [192] As we
shallsee, theseopenpublicationinitiativesincreasinglyrelyuponInternet-baseddistribution
techniques.
The healthcare industry provides extreme examples of the problem associated with distributing
incidentreportstoadiverseaudience. In2000,theMDAreceived7,249reportsofadverseincidents
involving medical devices. These resulted in 4,466 investigations after an initial risk assessment.
49 safety warnings were published; the MDA's annual report bases this gure on the sum of the
numbersofHazardNotices,SafetyNoticesandDeviceAlertsinTable14.1[540]. SafetyNoticesare
primarilydistributedthroughtheChief ExecutivesofHealthAuthorities,NHSTrustsandPrimary
CareTrustsaswellasthedirectorsofSocialServicesinEngland. Theseindividualsaresponsiblefor
ensuringthattheyarebroughtto\theattentionofallwhoneedtoknoworbeawareofit"[536]. Each
TrustappointsaliaisonoÆcerwhoensuresthat noticesaredistributed tothe`relevantmanagers'.
Similarly,eachlocalHealthAuthorityappointsaliaisonoÆcertoensurethatnoticesaredistributed
to Chairsof Primary CareGroups, Registration Inspection Units, Independent Healthcare Sector
and representatives of the Armed Services. The MDA also requires that notices are sent to the
ChiefExecutivesofPrimaryCareTrustswhoarethenresponsibleforonwarddistributionto their
sta. Social Services Liaison OÆcers play a similar role but are specically requested to ensure
distributiontoRegistrationInspectionUnitsandResidentialCareHomes.
The distributionresponsibilities of the individuals in the MDA hierarchyare presentedin Ta-
ble14.3. Thedetailedresponsibilitiesofeachindividualandgroupare,however,lessimportantthan
thelogistic challenges that must beaddressedby theMDA when theyissue aSafety Notice. For
instance, anyindividual warningwill onlybesenttosomeportionof thetotalpotentialaudience.
ManySafetyNoticesarenotrelevanttotheworkofSocialServices. Inconsequence,eachpublished
warningcomeswithalistofintendedrecipients. Theseareidentiedbytherstlevelinthedistri-
butionhierarchy:HealthAuthorities,NHSTrusts,PrimaryCareTrustsandSocialServices. Liaison
oÆcersarethenresponsibleforensuringthatinformationisdirectedtothoseatthenextlevelinthe
hierarchy. Thisselectivedistributionmechanismcreatespotentialproblemsif,forexample,aSocial
Servicedepartmentfails to identify that aparticular Safety Noticeis relevantto their operations.
TheMDA, therefore,issueaquarterlychecklistthatisintendedtohelp liaisonoÆcersensurethat
theyhavereceivedandrecognisedallapplicablewarnings.
TheMDAdistributionhierarchyillustratesanumberofimportantissuesthataectallreporting
systems. Thereis atensionbetweenthe needto ensurethat anyone withapotentialinterestin a
SafetyNoticesreceivesacopyofthewarning. This impliesthat LiaisonOÆcersshould erronthe
side of caution and disseminate them as widely as possible. On the other hand, this may result
in a large number of potentially irrelevant documents being passed to personnel. The salience
of any subsequent report might then bereduced bythe need to lter these lessrelevantwarning.
Thesearguments,togetherwiththeexpenseassociatedwithmanyformsofpaper-baseddistribution,
impliesthatLiaisonOÆcersshould targetanydistributionastightlyaspossible. Later sectionsof
thischapterwillreturntothistensionwhenexaminingthegenericproblemsofprecisionandrecall
Organisation LiaisonOÆcerforwardsto Foronwarddistribution to
NHSTrust AppropriateManager RelevantstatoincludeMedicalDi-
rectors, Nurse Executive Directors,
DirectorsofAnaesthetics,Directors
of Midwifery, Special Care Baby
Units/PediatricIntensiveCare,Ma-
ternity Wards,OperatingTheatres,
Ambulance NHS Trusts and Acci-
dentandEmergencyUnits.
HealthAuthority PrimaryCare Directors of Primary Care Local
Representatives Committees Chief
ExecutivesofPrimaryCareGroups
Individual GP Practices Dentists
OpticiansPharmacists
RegistrationInspectionUnits Care in the Community, Homes
(Group Homes), Nursing homes,
Managers of independent sector
establishments, Private hospitals,
Clinicsandhospices
SocialServicesDepartment In-houseservices Residential Care Homes (elderly,
learning diÆculties, mental health,
physical disabilities, respite care),
Day Centres, Home Care Services
(in-house and purchased), Occupa-
tional Therapists, Children's Ser-
vices, Special Schools, Other ap-
propriate Local Authority depart-
ments (for example Education de-
partments for equipment held in
schools).
RegistrationInspectionUnit Any of the above servicesprovided
bytheindependentsector.
Table14.3: MDA'sDistributionHierarchyforSafetyNotices
The success of theMDA distribution hierarchy relies on individual Liaison OÆcers. Theyex-
ercisediscretion in disseminating particularwarningsto appropriatemanagersand directors. The
signicanceoftheLiaisonOÆcerisalsoacknowledgedbytheMDAinarangeofpracticalguidelines
thatareintendedtoensuretheintegrityofthesedistributionmechanisms. Forinstance,healthcare
organisationsmustidentify afaxnumberande-mailaddressfortheprimaryreceiptofHazardNo-
tices and Device Alerts. They must also arrangefor someone to deputise in the LiaisonOÆcer's
absence. The Liaison OÆcer is responsible for ensuring that Hazard Notices and Device Alerts
are distributed immediately after publication. Safety Notices cantake aless immediate route, as
describedinpreviousparagraphs. LiaisonOÆcersarealsoresponsiblefordocumentingtheactions
thataretakenfollowingthereceiptofHazardNotices,DeviceAlertsandSafetyNotices. Inpartic-
ular,theymustrecordtherecipientsofthese variousformsof incidentreport. Thedocumentation
shouldalsorecordwhenthereportswereissuedandasignedassurancefrom therecipientthatany
requiredactionshavebeentaken.
LiaisonOÆcersnotonlypassonSafetyNoticesto`appropriate'managers,theycanalsochoose
to distribute particular warnings to sta. For instance, such direct actions might be used to en-
sure that new employees or contract sta are brought upto date with existing warnings. These
ferent industries. Not onlydo they create the need for special procedures in the national system
operatedbytheMDA, theyalso complicatethetask ofcommunicatingrecommendationsfrom lo-
cal systems. Changesin working procedures in individual hospitaldepartmentscreate signicant
trainingoverheadsfortemporary`agency'stawhomaybetransferredbetweendierentunitsover
arelativelyshortperiodoftime. Whensuchtrainingisnotexplicitlyprovidedthenitislikelythat
communicationsproblemswilloccurduring shifthand-overs[344].
PrevioussectionshavearguedthatLiaisonOÆcersplayanimportantrolewithintheparticular
distribution mechanisms that are promoted by the UK MDA. Aspects of their role are generic;
theycharacteriseissuesthat mustbeaddressedbyallreportingsystems. Forexample,theconict
between the need for wide distribution and the problems of overloading busy sta apply in all
contexts. Manyreportingsystemsmustalsoensurethatnewworkersandcontractstaarebrought
up to date. Similarly, there is a generic tension between enumerating the intended recipients of
a report and allowing local discretion to determine who receives a report. This last issue can
be illustrated by the way in which particular, critical reports constrain or guide the actions of
LiaisonOÆcers. Forexample,arecentDevice Bulletinintopatientinjuryfrombedrailsexplicitly
statedthat it should be distributed to allsta involvedin the procurement, use, prescriptionand
maintenance of bed rails. Liaison oÆcers were specically directed to ensure that copies of the
report were forwarded to `health and safety managers; loan store managers; MDA liaison oÆcers
(foronwarddistribution); nurses;occupationaltherapists; residentialandnursing homemanagers;
risk managers.' [539] In contrast, other Device Bulletins explicitly encourage Liaison OÆcers to
adopt afar broader dissemination policy. A report into the (ab)use of single-use medical devices
enumerated the intended recipients as all Chief executives and managers of organisations where
medicaldevicesareused, allprofessionalswhousemedicaldevices,allprovidersofmedicaldevices
andallstawhoreprocessmedicaldevices[537].
Previous paragraphshave focussed on the problems of ensuring that incident reports are dis-
seminatedeectivelywithintheorganisationsthat participateinareportingscheme. Wehavenot,
however,considered the additionalproblems that arise when anylessons must be sharedbetween
organisationsthatoperatetheir ownindependentreporting systems. Legislationis, typically,used
toprovideregulatorswiththeauthoritynecessarytoensurethatsafety-relatedinformationisshared
throughnationalorindustry-widesystems.Suchlegalrequirementsoftenfailtoaddresstheconcerns
thatmanycompaniesmighthaveaboutprovidinginformationto such reportingsystems. There is
a clear concern that commercially sensitive information will be distributed to competitors. The
exchangeof safety-relatedinformationoftenraisequestionsaboutcondentialityandtrust:
\(The)FDAis keenlyawareofand sensitivetotheimpactsofthesenewregulatory
requirementsonthepace oftechnologicaladvancementand economicwell-beingofthe
medical device industry. At the same time, the agency is cognizant of the usefulness
of information aboutthe clinical performance of medical devices in fullling itspublic
healthmandate... FDA mayrequirethe submissionof certain proprietaryinformation
becauseitis necessarytofully evaluatetheadverseevent. Proprietaryinformationwill
bekeptcondentialinaccordancewith Sec. 803.9,which prohibitspublic disclosureof
tradesecretorcondentialcommercialinformation.." [254]
Lesscriticalinformation,forinstanceaboutnear-missoccurrences,mayberetainedwithincorporate
reportingsystems. Other organisationscanthenbepreventedfromderivinganyinsightsthat such
reportsmightoer. Theabilityto overcomethesebarriersoftendependsuponthemicro-economic
characteristicsoftheparticularindustry. Forinstance,itcanbediÆculttoencouragethealtruistic
sharing of incident reports in highly competitive industries. In other markets, especially those
thatare characterised byoligopolistic practices,itcanbefareasier toensurethe cooperationand
participationofpotentialrivals. Forexample,themajortrainoperatingcompaniescombinedwith
theinfrastructureprovidestoestablishtheCIRASreportingsystemonScottishrailways[198]. This
scheme has alot in common with the CNORIS regional reporting system that has recently been
establishedacrossScottishNHShospitals[419]. Anotherfeature ofthesesystemsis,however,that
thelessons are seldom disseminatedbeyond the smallgroup ofcompaniesor organisationswithin
The increasing impact of a global economy has raiseda number of diÆcult moral issues that
were not initially considered by the early proponents of reporting systems. For example, there
have been situations in which the operators of a non-punitive reporting system have identied
failuresby individualswhowork in counties that dooperatepunitive,legal approachesto adverse
occurrences[423]. Such situations can create particularproblems when individual employees may
havecontributedanincidentreportontheunderstandingthattheywereparticipatingina`noblame'
system. Althoughthese dilemmasarerelativelyrare,itisimportantto acknowledgetheincreasing
exchange of data betweendierentreporting systems. For instance, the 49 MDA warnings, cited
inpreviousparagraphs,resultedin 32noticationsbeingissuedto otherEuropeanUnionmember
states[540].
The direct distribution of reports by the MDA to other EU member states represents one of
several approached to the international dissemination of safety-related information. It eectively
restricts the dissemination of information, in the rst instance, to the other participants in the
politicalandeconomicunion. Otherdistribution mechanismsmustbeestablishedonacountry-by-
countrybasisfor thewiderdistributionofinformation, forexamplewith theUSFDA.TheGlobal
Aviation Information Network initiatives represent an alternative approach to the dissemination
of safety-related incident reports [310]. As the name suggests, the intention is to more beyond
regionaldistributionto provide globalaccess to this safetyinformation. Similar initiativescanbe
seenin the work of theInternationalMaritime Organisation(IMO) and the InternationalAtomic
EnergyAuthority. Suchdistributionmechanismsfaceimmensepracticalandorganisationalbarriers.
Thesameissues of trustand condentialitythat complicate the exchange of information between
commercialorganisations also aect these wider mechanisms. There is also anadditionallayer of
politicalandeconomicself-interestwhenincidentsmayaecttheviabilityandreputationofnational
industries. Theseproblemspartlyexplainthehaltingnatureofmanyoftheseinitiatives. Theyare
addressingthedistributionproblembymakinginformationavailabletomanynationalandregional
organisations. However,theyoftenfailtoaddressthecontributionproblembecauseveryfewreports
areeverreceivedfromsomenations.
14.2 From Manual to Electronic Dissemination
Previous paragraphs have argued that the problems of disseminating information about adverse
occurrences and near miss incidents stem from the frequency and diverse range of publications;
from tight publication deadlines and resourceconstraints and from the diÆculty of ensuring that
theintendedreadershipcanaccessacopyofthereport. These problemshavebeenaddressedin a
numberof ways. Forexample,thelast sectionexaminedanumberofdistribution modelsthat are
intendedtoeasethelogisticsofdisseminatingincidentreports. Thehierarchicalapproachadoptedby
theMDAwasusedtoillustratethemannerinwhichkeyindividuals,suchasLiaisonOÆcers,often
lieattheheartofhierarchicalapproaches. Incontrast,thissectionmovesonfromtheseorganisation
techniquestolookatthewayinwhichdierenttechnologiescanberecruitedtoaddresssomeofthe
problemsthatcomplicatethedisseminationofincidentreports.
14.2.1 Anecdotes, Internet Rumours and Broadcast Media
Itisimportantnottooverlookthewayinwhichinformationaboutanincidentcanbedisseminated
bywordofmouth. Thiscanhaveveryunfortunateconsequences. Forinstance, theU. S.Foodand
DrugAdministration'sCenterforFood SafetyandAppliedNutritiondescribehowthecompanyat
thecentre ofaninvestigationrst became aware ofapotentialproblemthroughthecirculation of
rumours about theirinvolvement[255]. They report that `the rstnews the dairy plantreceived
that theywere being investigated in relation to this outbreak wasthrough rumour onthe street'.
Theplantoperatorsthen demanded to knowwhat wasgoingon; `Apparently someonehad heard
someoneelsetalkingabouttheYersiniaoutbreakandhowitwasconnectedtothedairyplant'. These
informalaccountsthenhadtobeconrmedwithaconsequentlossofcondenceintheinvestigatory
Informalchannelsareoftenfasterand, insomesenses,moreeectiveatdisseminatinginforma-
tionthanmoreoÆcialchannels. Rumoursoftencirculateaboutthepotentialcauseswellbeforethey
arepublishedby investigatoryorganisations. VeryoftenoÆcial reportsinto anadverseoccurrence
ornear-misscomeaslittlesurprisetomanyoftheindividualswhoworkinanindustry. Thedissem-
inationofsafety informationby wordof mouthis notentirelynegative. Manyorganisations, such
astheFDAandtheMDArelyuponsuchinformalmeasuresgivenlimitedprintingbudgetsandthe
vastaudiencesthattheyenvisageforsomewarnings. Similarly,theuseofanecdotesaboutprevious
failureshasprovidedanimportanttrainingtoolwellbeforeformalincidentreportingsystemswere
everenvisagedorimplemented.
Thereisadanger,however,thattheinformationconveyedbytheseinformalmeanswillprovide
apartial orbiased account of the information that is published by more oÆcial channels. Word
ofmouthaccountsarelikelyto provideanincompleteviewbeforetheoÆcialreportisdistributed.
ThiscanalsooccuraftertheoÆcial publicationofanincidentreportifindividualsmis-understand
orforget the main ndings of an investigation. They may also be unconvinced by investigators'
ndings. In such circumstances, there is atendency to develop alternativeaccounts that resolve
uncertainties abouttheoÆcial report. These unauthorisedreportsare, typically, intendedto gain
thelisteners'attentionrather thanto improvethe safetyofapplication processes. It isdiÆcultto
underestimatetheimpactofsuchinformalaccounts. Theycanunderminethelisteners'condence
intheinvestigatoryagencyeventhoughtheymayretainsignicantdoubtsovertheveracityofthe
alternativeaccount[280].
Inrecentyears,theinformaldisseminationofincidentrelatedinformationhastakenonarenewed
importance. Thegrowthofelectronic communicationmediahasprovidedsignicantopportunities
forinvestigatoryagenciestodistribute`authorised'accounts. Thesametechniquesalsoenableengi-
neers,focusgroupsandmembersofthegeneralpublictorapidlyexchangeinformationaboutadverse
occurrencesandnearmiss incidents. Therecognitionthat e-mail,Internetchatroomsandbulletin
boards canfacilitatethe`unauthorised' disseminationofsuchinformation hasattracted signicant
attentionfrom organisations,such astheFDA. Theissuessurroundingthese informalcommunica-
tionsareextremelycomplicated. Forexample,there isaconcernthat drugscompaniesanddevice
manufacturersmightexploit these communicationmediato activelypromotetheirproducts. This
resultedin a recent initiative to directly consider the position of the FDA towards`Internet Ad-
vertising and the Promotion of Medical Products' [258]. Duringthis meeting, a representative of
onepharmaceuticalcompanyarguedthattheyhadanobligationtomakesurethattheinformation
available to the public was asaccurate aspossible. Given the lackof Internet moderation, how-
ever,it wasimpossiblefor companies to correct everymisconception that mightarise; `wedo not
correcteverypiece ofgraÆtithat maybepaintedinsomeremoteareaof AustraliaorAlabamaor
Philadelphia,butwedorespondwhere wefeelthisis signicantandweneedto clarifytheissues'.
Arepresentativeofanother drugcompanyaddressedrumoursaboutadverseeventsmoredirectly:
\theremaybearumourthatacertainproductisgoingtobewithdrawnatacertaintimeandifno
onecomesinandstepsinwhohasaauthoritativeinformationandsays,`Thisisnottrue',thatkind
ofrumourcanabsolutelysnowballandcanbecomeuncontrollableifitisnotquashedrightwhenit
starts"[258].
Companiesarenottheonlyorganisationsthatcanhaveadirectinterestinrefutingwhatcanbe
termedInternetrumours. TheFDArecentlyhadtolaunchasustainedinitiativetocounterrumours
aboutthesafetyoftampons[265]. TheFDAidentiedthree dierentversionsofthisrumour:
1. One Internet claim is that U.S. tampon manufacturers add asbestos to their products to
promoteexcessivemenstrualbleedinginordertosellmoretampons. TheFDAcounteredthis
rumour by stating that `asbestos is not, and never has been, used to make tampon bers,
accordingto FDA, whichreviewsthedesignandmaterialsforalltamponssoldintheUnited
States'[276].
2. Anotherrumourallegedthatsometamponscontaindioxin. TheFDAreiteratedthat`although
past methods of chlorine bleaching of rayon's cellulose berscould leadto tiny amounts of
dioxin(amountsthatposednohealthrisktoconsumers),today,celluloseundergoesachlorine-
3. AnalInternetrumourarguedthatrayonintamponscausestoxicshocksyndrome(TSS)and
couldmakeawomanmoresusceptibleto otherinfectionsand diseases. TheFDA responded
that `whilethere isarelationshipbetweentampon useandtoxicshocksyndrome{abouthalf
ofTSS casestodayareassociatedwithtampon use{thereis noevidencethat rayontampons
createahigherriskthancottontamponswithsimilar absorbency'.
Inordertocounterthesevariousrumours,theFDAlaunchedacoordinateddistributionofinforma-
tionontheInternetandtothebroadcastmedia. Thisresponseindicatestheseriousnesswithwhich
theyregardtheInternetasadistributionmediumforalternativeor`unoÆcial'accountsofparticular
incidents,inthiscaseinvolvingToxicShockSyndrome. Suchactionsdonot,however,comewithout
aprice. Theyhelp to ensurethat the publicare aware ofthe scienticevidence in support of the
FDA claims. Theyalso inadvertentlyraise theproleof thoseInternetresourcesthat disseminate
therumoursin the rstplace. TheFDA's response,therefore,adds aform ofreected legitimacy
totheoriginalargumentsaboutthelink betweenTampon'sandTSS.It isimportanttoemphasise
that our use of the term `rumour' is not intended to be pejorative. In many cases, the informal
disseminationofinformationcanprovideausefulcorrectivetothepartialviewputforwardbymore
`oÆcial'agencies. Such alternativesourcesofinformationmust,however,supporttheirclaimsand
statements withappropriate warrants. Inparticular, it canbeargued that these informalsources
of information force oÆcial agencies to focus moredirectly on the issuesand concerns that aect
thegeneral public. TheInternet rumours about therelationship between tampons and TSS may
havecontainednumerous statementsthat couldnotsubsequentlybesupported, however,theydid
persuadetheFDAtoclarifytheexistingevidenceonanypotentiallinks.
Thepreviouscasestudyillustratessomeofthecomplexchangesthatareoccurringinthemanner
inwhichinformationaboutadverseoccurrencesisbeingdisseminated. Internetbulletinboardsand
chatroomshelpto publiciserumoursthat arethenpickedupbythepopularmedia. Atthisstage,
regulatory authorities must often intervene to correct or balance these informal accounts. It is,
however,insuÆcientsimplytopublisharesponseviaanoÆcialwebsitewhichisunlikelytoattract
many of the potential readers whohavean interest in aparticular topic. The regulatory agency
is,therefore,compelledto exploitmoretraditionalforms ofthebroadcastmediato refuterumours
thatwere primarilydisseminatedviathewebandrelatedtechnologies.
Thisreactiveuseofthemediarepresentsarelativelyrecentinnovation. Moretypically,investiga-
toryagencieshaveusedthepress,radioandtelevisioninamoreproactivemannertodisseminatethe
ndingsofincidentreports. Aswehaveseen,thisuseofthemediarequirescarefulplanning;thereis
adangerthat thepartiesinvolvedinaninvestigationmaylearnmoreabouttheirinvolvementfrom
thepressthanfrommoreoÆcialchannels. TheFDAissimilartomanynationalagenciesinthat it
followsdetailedguidelinesontheuseofthemediato disseminateinformation. Forexample,media
relationsmustbeexplicitlyconsidered aspartofthestrategydocumentsthatare preparedbefore
each product recall. Thedissemination of information in this manner must be treated extremely
carefully. It is important that the seriousness of any recall is communicated to the public. It is
alsoimportanttoavoidanyform ofpanicoranyadversereactionthat mightundulyinuence the
longtermcommercial successofthecompaniesthatmaybeinvolvedin anincident. Thesensitive
natureofsuchrecallnotices isrecognisedin theFDAprovisionthat thewarningsmaybereleased
eitherbytheFDAorbytherecallingrmdependingonthecircumstancessurroundingtheincident
[259]. The political sensitivity of these issues is also illustrated by the central role that is played
bytheFDA'sDivision of Federal-State Relationsduring Class I recalls. Thisclassicationisused
whenis expected and when the`depth' ofthe recall isanticipated to requireactionby aretailers
andconsumers. The Federal-State Relations division isrequired to use e-mailto notify stateand
local oÆcials of recalls that are associated with serious health hazards or where publicity is an-
ticipated. These oÆcials are then issued with enforcementpapersthat are preparedby the FDA
PressRelationsSta. This mechanismillustrates themanner in which investigatoryagenciesmay
operateseveral paralleldissemination activitieseach withverydierent intentions. In additionto
thepublicationofincidentreports,pressreleasesarepreparedtoinitiateactionsbythepublicand
byretailers. These maybe distributed at press conferences, by direct contactwith particular re-
portersandbyreleasestoallAssociatedPressandUnitedPressInternationalwireservices. Further
briefed'torespondtoquestionsfrom thepress.
Itisalsoimportanttoacknowledgethecentral roleofpressand mediarelationssta. Not only
doesthisdepartmentwarnother membersoftheorganisation ofmedia interest. Theyalsoensure
thattheir colleaguesareadequatelybriefed to respondto media interest. Theirabilityto perform
thesetasksisdependentuponthem beingnotiedintheearlystagesof anyincidentinvestigation.
FDA regulationsrequirethat thePressRelationsSta arenotied byanyunit that `publicityhas
occurredrelatingtotheemergencycondition,aswellaspending requestsforinformationfrom the
media and/or public' [259]. The seniormedia relations sta then liaise directly with theoÆcials
closest to the scene to ascertain what information needs to be released and when it should be
disseminated to best eect. It can, however, be diÆcult to ensure that such press releases will
be giventhe prominencethat is necessaryin order to attractthe publics'attentionto apotential
hazard. Somewarningshave arelativelyhigh newsvalue. The FDA's Consumer magazine often
providesjournalistswithavaluablestartingpointfortheseincidents. Forinstance,arecentwarning
centredonaparticulartypeofsweetorcandythathadresultedinthreechildrenchokingtodeath.
Someoftheseproductscarriedwarninglabels,suggestingthattheyshouldnotbeeatenbychildren
or the elderly. Other labels warn of a choking hazard and say to chew the sweets thoroughly.
Someweresoldwithoutanywarning. Thisstoryattractedimmediateand focussedmediainterest.
Anotherwarning,whichwasissued onthesameday astheonedescribed above,attractedfarless
mediaattention. Thisconcerned thepotentialdangers ofconsuming amislabeledpoisonous plant
calledAutumnMonkshood[268]Thepackagescontainingtheplantweremistakenlylabeledwiththe
statement,`Allpartsofthisplantaretastyinsoup'. Theyshouldhaveindicatedthatconsumptionof
theplantcanleadtoaconitinepoisoningandthatdeathcouldoccurduetoventriculararrhythmias
ordirect paralysisof theheart. Simplyreleasing informationto themedia aboutpotentiallyfatal
incidentsdoesnot implythat all incidentswill be equallynews worthy northat theywill receive
equalprominenceinpress,radioortelevisionbroadcasts.
As we haveseen, itcan be diÆcultfor regulatory and investigatoryagencies to use the media
asameansofdisseminatingsafetyinformation. Thisinvolvesthecoordinationofpressreleasesand
conferences. It also involvesthetraining ofkeysta, such aspressliaisonoÆcers, andthe use of
electronic communicationstechniques to ensure that other members of sta are informed how to
respondtomediaquestions. Evenifthisinfrastructureisestablishedthereisnoguarantee,without
legalintervention,thataparticularwarningwillreceivetheprominencethatisnecessarytoattract
publicattention. Such problems are mostoften encountered bylarge-scalenational systems. The
issuesthat areraisedbymedia dissemination ofincidentinformation are, typically,quite dierent
for smaller scale systems. There can also be a strong contrast in media relations when incident
informationattracts`adverse'publicity. Thisisbestillustratedbythephenomenonknownas`doctor
bashing' which hasemerged in the aftermath of anumber of incidents within the UK healthcare
industries. Many professionals nd themselves faced by calls from the government and from the
media to be increasingly open about potential incidents. For example, Alan Milnburn the UK
HealthSecretaryhasarguedthatthe\NationalHealthServiceneedstobemoreopenwhenthings
go wrong so that it can learn to put them right" [111]. Together with this increased openness
\theywouldalsohavetobeaccountablefortheirerrorsandpreparedtotakeresponsibility". Some
doctorshavedescribed such statementsand theassociatedmedia publicity as`hysterical'. Recent
BBC reports summed up this attitude by citing a General Practitioner from the North West of
England;\Shameon themedia for sensationalisingand exaggeratingincidents...shame on you for
failingtoreport accuratelyadverseclinicalevents"[110].
Public and government pressure to increase the dissemination of information about medical
incidentsmustovercomemanydoctor'sfearof adverseor`sensational'presscoverage. Atpresent,
many NHS trusts have still to face up to the consequences of this apparent conict. They are
reluctant to disclose information about previous incidents even to their own sta for fear that
detailsmight`leak'to thepress. Inthis domainat least, weare averylongwayfrom theculture
of openness that the proponents of incident reporting systems envisage as a prerequisite for the
eective implementation of their techniques. It is important not to simply view these tensions
assimply the result of media interest in disseminating sensational accounts of adverse incidents.
Doctors'Committee sawthis when heargued that \wehave amoreconsumeristsociety... people
arecomplainingmoreabouteverything... thereisalotof doctor-bashinginthepress"[108]. Such
quotationsillustrate the way in which the media not only inform society, asin the case of FDA
warnings,buttheyalsoreecttheconcernsofsociety.
Thissectionhasfocussedonthe`informal'disseminationofinformationaboutadverseincidents.
Inparticular,ithasfocussedonthewayinwhichelectronicandInternet-basedcommunicationshave
provided new means of distributing alternative accounts of near-misses and adverse occurrences.
We have also described how regulatory organisations have used the same means to rebutt these
alternativereports. Theconventional media is routinelyused to support these initiatives. It can
alsobeused to publicise moregeneralsafetywarningsand caninitiate investigationswhere other
forms of reporting have failed to detect safety-related incidents. This more positive role must be
balanced with the problems of media distortion that dissuade managers from disseminating the
ndingsof incident reporting systems. There is astark contrast between theuse of themedia to
publicisenecessarysafetyinformationandthefearofpublicityintheaftermathofanadverseevent.
14.2.2 Paper documents
Theprevioussectionhasdonelittlemorethat summarisetheinformalcommunicationmediathat
support the distribution of safety related information. Similarly, we have only touched upon the
complex issues that stem from the role of the media in incident reporting. These related topics
deservebooksintheirownright,however,brevitypreventsamoresustainedanalysisinthisvolume.
Incontrast,theremainderofthischapterfocusesonmore`oÆcial'meansofdisseminatingincident
reports. Inparticular, thefollowingsectionanalysesthe strengthsand weaknessesofconventional
paper-basedpublicationstodisseminatesafety-relatedinformation.
Oneofthemostsuasivereasonsforsupportingthepaper-baseddisseminationofincidentreports
isto meetregulatory obligations. The importance of this media is clearlyrevealed in thevarious
regulationsthat governthe relationshipbetweenthe FDA, manufacturingcompaniesandtheend-
usersofhealthcareproducts. Theprimary focusof theseregulationsison theexchange ofwritten
orprinteddocumentation. This emphasis isnotthe resultof historicalfactors. It isnot simplya
defaultoptionthathasbeenheldoverfrompreviousversionsoftheregulationsthatweredraftedin
anagebeforeelectronic disseminationtechniques becameapracticalalternative. Aswehaveseen,
therecommendationsinsomeincidentreportscanhavealegalforce. Companiesmayberequiredto
demonstratethat theyhavetakenstepsto meetparticularrequirements. Thiscreatesproblemsfor
theuseofelectronic mediawhereitcanbeverydiÆcultto determinetheauthenticityofparticular
documents. It would be relativelyeasy to alter manyof the reports that are currently hosted on
regulatoryand governmental web-sites. Latersections will describearangeof techniques,such as
theuseof electronicwatermarks,that canincreaseareader's condenceabout theauthenticity of
the documents that are obtained over the Internet. Unfortunately, none of the existing incident
reporting sites have adopted this technology. In consequence, paper versions continue to exist
as the `gold standard' against which compliance is usually assessed. Copies obtained by other
distribution mechanisms are, therefore, seens as in some way additional to this more traditional
formofpublication.
Afurtherbenetofconventional,paper-baseddisseminationtechniquesisthatregulatoryagen-
ciescanexploitexisting postaldistributionservices. Ahostofexternalcompaniescanalsobeused
to assist with the formatting, printing and mailing of these documents. The technology that is
requiredto perform these tasksis well understood andis also liableto bereadilyavailable within
mostorganisations. These areimportantconsiderations. Simplicity andfamiliarity helpto reduce
thelikelihood of failures occurring in the distribution process, although aswehave seenthey are
notabsoluteguarantees! Minimalstatrainingisneededbeforeinformationcanbedisseminatedin
thisway. Itisforthisreasonthatmostsmallscalereportingsystemsinitiallyexploitthisapproach.
Typically, newsletters are duplicated using a photocopying machine and are then made available
eitherinstacommonareasorinaposition thatisclosetoasupplyofreportingforms.
Paper-baseddisseminationtechniquessimplify thetaskofdistributing incidentreportsbecause
VeryWell Well NotWell NotatAll
17,862,477 7,310,301 4,826,958 1,845,243
Table14.4: 1990USCensusDataforSelf-ReportedAbilityin English
statepostalservices. There are further advantages. Noadditionaltechnology, suchasa PC with
anInternetconnectionorCD-ROM,isrequiredbeforepeoplecanaccesssafety-relatedinformation.
This is a critical requirement for the dissemination of someincident reports. One participant at
arecentFDA technical meeting wasextremelyirritated bythe continualreference towebsites as
a primary communication medium. He asked the others present whether they knew how many
Americancould access the Internet orcould understand English[262]. Such comments act asan
importantreminder that paper-based publications continue to have an important role in spite of
the proliferation of alternativedissemination techniques. For the record, Table 14.4 provides the
latestavailableguresfrom the1990US Censusdescribingself-reportedEnglishability. Thetotal
US populationwas reported as230,445,777of which thereweresome198,600,798individuals who
reported that theycould onlyspeak English. There were 31,844,979who described themselvesas
beingprimarilynon-Englishspeakers. Theself-reportedguresforthestandardofEnglishamongst
thiscommunityareshowninTable14.4. Theproportionofthepopulationwhoexpressproblemsin
understandingEnglishappearstoberelativelysmall. However,theremaybeasignicantproportion
ofthe populationwho didnotreturn acensusform and there is aconcernthat theproportion of
non-Englishspeakersmightberelativelyhigh inthis community. Thereis alsoanaturaltendency
to over-estimatelinguistic ability in such oÆcial instruments. Such factors motivatethe provision
ofalternatelanguageversionsofsafety-relatedinformation[823]. The2000censusprovidedfurther
insightsintothegrowthoftheInternetamongsttheUSpopulation[824]. Thecensusasked`Isthere
apersonalcomputerorlaptopinthishousehold?'. Thereturnsindicatedthat54,000,000,or51%,of
householdshadoneormorecomputersinAugust2000. Thiswasanincreaseof42%fromDecember
199845,000,000,or42%,ofhouseholdshadatleastonememberwhousedtheInternetathone,This
hadrisenfromonly26%in1998and18%in1997. Suchstatisticsreinforcethepointthatsignicant
proportionsofthepopulationinwhatisarguablytheworld'smosttechnologicallyadvancednation
still do nothave Internet access. This is liable to be less signicant for incident reports that are
targeted at commercialorganisations, for which onemight expect ahigher percentageof Internet
connectivity. The census statistics are, however,a salient reminder for moregeneral reports and
warningsuchas thoseissuedbytheFDAthat aredeliberatelyintendedforthegeneralpublic.
Paper-based dissemination techniques are also resilient to hardware failures. It is arelatively
simplemattertondalternativeprintingfacilitiesandpostalservices. Itcanbefarmorecomplexto
introducealternativeweb-serversorautomaticfaxroutingservices. Thereliabilityofthedistribution
serviceisonlyoneaspecttothisissue. Therecanalsobeconsiderableproblemsinensuringthatthe
intendedrecipientsofincidentreportscansuccessfullyretrievealternativeformats. Postalservices
are seldom swamped by the volume of mail. The same cannot be said by web servers or even
bytheuse of fax-baseddistributiontechniques. If theintended recipient's faxmachine isbusy at
thetimewhenanautomateddistributionserviceattemptsto distributeanincidentreport, critical
informationcan bedelayedbyhoursand evendays. At peak timesof theday, manyrequestscan
either fail entirely or be signicantly delayed as users request incident reports from the FDA or
MDAweb-sites. Oneparticularproblemhereisthatmanygovernmentwebsites onlymakelimited
useof more advanced techniques, such as predictive cacheing or mirrorsites [418]. Similarly, the
serversthatprovideaccesstoincidentreportsmayalsobeusedtoprovideaccesstootherdocuments
thatattractalargevolume ofusersthroughouttheday. Thereis acertainironyin themannerin
whichsomeincidentreportingwebsitesalsoelicituser-feedbackaboutthefailureofthosesitesthat
areintended to provide access to otherforms of incidentreports. Even ifreaderscan downloada
computer-basedreport,thereisnoguaranteethattheypossesstheapplicationsoftwarethatmaybe
requiredtoviewit. Chapter12.4describedhowmostincidentreportingsites exploiteither HTML
and PDF. The former supports the dissemination of web-based documents because no additional
isformattedin HTMLwillbefaithfullyreconstructedwhenprinted. Thisissignicantbecausethe
psychologicalliteraturepointsto numerouscognitiveandperceptualproblems associatedwith the
on-screenreadingoflongandcomplexdocuments[876]. Inconsequence,manyorganisationsexploit
Adobe'sproprietaryPDF format. PDFreaderscanbedownloadedformostplatformswithoutany
charge. Problemsarise,however,whenincidentreports thathavebeenpreparedforviewingunder
oneversionof thereadercannotthen beviewedusingother versions. Forinstance, arecentMDA
reportintoBloodPressureMeasurementDevicescontainedthefollowingwarning: \AdobeAcrobat
v.4isrequiredtoviewonscreenthecontentofthetablesatp.9+16...AdobeAcrobatv.3canview
remainder of document and can print in full". Paper-based dissemination techniques avoid such
problems,whichpresentaconsiderablebarrierformanyuserswhomightotherwisewanttoaccess
thesedocuments.
Therearefurtherbenetstomoretraditionaldisseminationtechniques. Forinstance,thephysical
nature of paper-based publications enablesregulators to combine documents in asingle mailshot.
Thisisimportantbecausepotentialreaderscanskimtheserelateditemstoseewhetherornotthey
arerelevantto theirparticulartasks. ThiscanbefarmorediÆcultto achievefromthehypertext
labelsthatare,typically,usedtoencouragereaderstoaccessrelateditemsovertheweb[758]. The
exiblenatureofprintedmediacanbeillustratedbythewayinwhichIncidentReportInvestigation
SchemenewsandsafetyalertsweredirectlyinsertedintoprintedcopiesoftheAustralianTherapeutic
Goods Administration newsletter [45]. Similar techniques have been adopted by many dierent
investigation schemes. Safety-related information is included into publications that are perceived
to have a wider appeal. This is intended to ensure that more people will consider reading this
informationthaniftheyhadsimplybeensentasafety-relatedpublication.
Therearealsosituationsinwhichinvestigatoryandregulatoryorganisationshavenoalternative
buttouseprintedwarnings. Forexample,theFDAtookstepstoensurethatprintedwarningswere
distributedaboutthedangerofinfectionfromvibriovulnicusasaresultofeatingrawoysters[256].
Thesignsandsymptomsofpreviouscasesweredescribedandtheresultingwarningswerepostedat
locationswherethepublicmightchoosetobuyorconsumetheseproducts. TheuseoftheInternet
orofbroadcastmediaprovideslessassurancethatindividualswhoareabouttoconsumerawOysters
areawareofthepotentialrisks. Thisincidentalsoillustratessomeofthelimitationsofpaper-based
disseminationtechniques. ManyofthecasesofinfectionwereidentiedinandaroundLosAngeles.
TheFDA soon discoveredthat,as notedabove, a signicant proportion of this community could
notspeak orread Englishat thelevelwhich was requiredto understand thesigns that had been
posted. TheStatesofCalifornia,Florida,andLouisianaonlyrequiredOystervendorstopostsigns
inEnglish. Inconsequence,theFDAsupplementedtheseprintedwarningswitha24-hourconsumer
`SeafoodHotline'thatprovided informationinEnglishandSpanish.
There area number ofproblems that limittheutility of paper-based disseminationtechniques
asa meansof distributingthe documents that are generated by incident reporting systems. The
most obvious of these issues is the cost associated with both the printing and shipping of what
canoftenbe largeamountsofpaper. These costscanbeassessedin purely nancialterms. They
arealso increasinglybeingmeasuredin terms oftheir widerecologicalimpact,especially forlarge
scale reporting systems that can document many thousands of contributions each year. Many
organisationsattempttodefraytheexpensesthatareassociatedwiththegenerationanddistribution
ofincidentreportsbychargingreaderswhowanttoobtaincopiesofthesedocuments. Thisraisesa
numberof complex,ethicalissues. Forexample,thecostof obtainingacopyofanincidentreport
canact asapowerfuldisincentiveto the dissemination of safety-relatedinformation. This should
notbeunderestimated forstate healthcareserviceswhere anyfunds that areused to obtainsuch
publications cannot then be spent on moredirect forms of patient care. Some regulatory bodies,
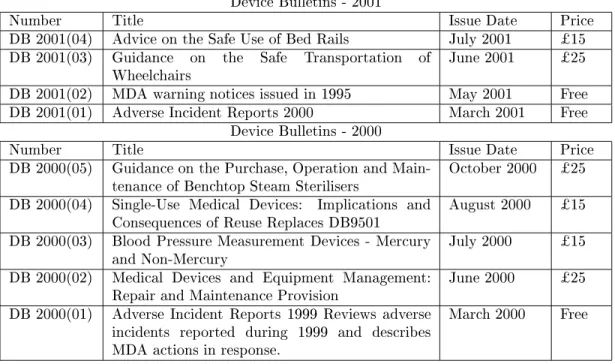
therefore,operateatiered pricingpolicy. Forexample,theMDAdo notmakeacharge forany of
theDeviceBulletinsrequestedbymembersoftheNationalHealthService. Incontrast,Table14.5
summarisesthepricesthatmustbepaidtoobtaincopiesofanumberofrecentMDAdocumentsby
thoseoutsidethenationalhealthsystem[541].
ThecostsillustratedinTable14.5donotsimplyreecttheoverheadsassociatedwiththeprinting
andshippingofthesedocuments. Theyalso,inpart,reectthecostsofmaintainingacatalogueof
DeviceBulletins-2001
Number Title IssueDate Price
DB2001(04) AdviceontheSafeUseofBedRails July2001 $15
DB2001(03) Guidance on the Safe Transportation of
Wheelchairs
June2001 $25
DB2001(02) MDA warningnoticesissued in1995 May2001 Free
DB2001(01) AdverseIncidentReports2000 March2001 Free
DeviceBulletins-2000
Number Title IssueDate Price
DB2000(05) GuidanceonthePurchase,OperationandMain-
tenanceof BenchtopSteamSterilisers
October2000 $25
DB2000(04) Single-Use Medical Devices: Implications and
ConsequencesofReuseReplacesDB9501
August2000 $15
DB2000(03) Blood PressureMeasurementDevices - Mercury
andNon-Mercury
July2000 $15
DB2000(02) Medical Devices and Equipment Management:
RepairandMaintenanceProvision
June2000 $25
DB2000(01) Adverse Incident Reports 1999 Reviews adverse
incidents reported during 1999 and describes
MDA actionsin response.
March2000 Free
Table14.5: PricingPolicyforRecentMDA DeviceBulletins
storagethatisrequiredtoholdthelargenumbersofpublicationsthatweredescribedintheopening
pagesofthis chapter. TheMDAhaspublishedwellover300dierentreportsin thelast veyears.
Thelogistics of supporting thepaper-based distribution of such acataloguehas led many similar
organisations to abandon such archivalservices. The Australian Institute of Health and Welfare
nowonlyprovidethedetailed back-updataand tablesfor many oftheirpublications inelectronic
format[41].
A number of further limitations aect the use of paper-based dissemination techniques. The
previousparagraphs haveargued that such approaches do not suer from the problems of server
saturationandnetwork loadingthat canaect electronic distribution mechanisms. Unfortunately,
moreconventiondisseminationmechanismscansuerfromotherformsofdelaythatcanbefarworse
thanthose experienced with Internet retrievaltools. Even with relatively eÆcient administration
procedurestherecanbeasignicantdelaybetweentheprintingofareportandthetimeofitsarrival
withthe intended readership. These delays are exacerbatedwhen safetymanagers ormembers of
thegeneralpublicrequireaccesstoarchivedinformationaboutpreviousincidents. Forinstance,the
MDA promiseto dispatchrequested reports by thenextworkingdayif theyarein stock [542]. If
theyarenotcurrentlyinprintthentheywillcontactthepersonororganisationmakingtherequest
withinforty-eighthours. ThesedelayscanbeexacerbatedbytheuseoftheUK'ssecond-classpostal
servicetodispatchtherequested copiesof thereport. Thisreduces postagecosts,however,it also
introducesadditionaldelays. Thesecondclassserviceaimstodeliverbythethirdworkingdayfrom
when it was posted. Inthe period from April to June 2001, 92.5% of second class `impressions'
satisedthistarget. Thisisanimportantstatisticbecauseitimpliesthatevenifthereisarelatively
long delay before any requested report can be delivered, the duration of this delay is relatively
predictable. Inthesameperiod,theUKpostalserviseachievedcloseto100%reliabilityintermsof
thenumberofitemsthat werelost. Thehigh volumeofpostaltraÆcdoes,however,maskthefact
thatConsigniareceived223,495complaintsaboutlostitems,40,529complaintsaboutservicedelays
and37,256complaintsaboutmis-deliveriesbytheRoyalMailservicefrom Aprilto June2001.
Thedelaysintroducedbyarelianceonthepostalserviceorsimilardistributionmechanismsalso
createsproblemsin updatingincidentreports. Inconsequence,organisationsmaybeintheprocess
revised in the nal report. Updating problems aect a wide range of the publications that are
produced from incident reporting systems. For instance, the FDA explicitly intended that their
TalkPapers,whicharepreparedbythePressOÆcetohelppersonnelrespondtoquestionsfromthe
public,aresubjecttochange`asmoreinformationbecomesavailable'[269]. Evenwhenrevisionsare
madeoveralongertimeperiod,itisimportantnottounderestimatetheadministrativeburdensand
the costs of ensuring that all interestedparties receive new publications about adverse incidents.
This point can be illustrated by the problems surrounding Temporomandibular Joints (TMJs).
Theseimplantshavebeenusedinseveraldentalprocedures. Theywereinitiallyintroducedontothe
market beforea 1976amendment that requiredmanufacturersto demonstratethat such products
were both safe and eective. TMJs were, therefore, exempt from the terms of the amendment.
From1984toJune1998,theFDAreceived434adverseeventreportsrelatingtothesedevices. 58%
of these incidentsresulted in injury to the patient. In 1993, the Dental Products AdvisoryPanel
reclassiedTMJsintotheirhighestriskcategory(III).AllmanufacturersofTMJdeviceswerethen
requiredtosubmitaPremarketApprovalApplication,demonstratingsafetyandeectiveness,when
called for by the FDA. In December 1998, the FDA called for PMAs from all manufacturers of
TMJimplants. This wasfollowedupbythepublicationin 1999of aconsumerhandbook entitled,
`TMJ Implants- A ConsumerInformational Update'. In April 2001 this was updatedto present
furtherinformationaboutthechangingpatternofincidentsinvolvingthesedevices. Ascanbeseen,
adverse occurrencesled to the publication of reclassication information in 1993. This had to be
disseminatedto alldevice manufacturers. This wasrevisedin 1998 whenthePremarketApproval
Applicationswere called for. This change has considerable implications; theFDA have to ensure
thattheycontactallofthecommercialorganisationsthatmightbeaectedbysuchachange. TMJ's
arerelativelyspecialistdevicesandsoonlyahand-fullofcompaniesareinvolvedin manufacturing
themin theUnited States. Itis importanttorecognise,however,that theClass III categorisation
alsoappliedtothesaleofforeignimports. Onesolutiontothepotentialproblemsthatmightarisein
suchcircumstancesistouselegalpowerstorequirethat alldevice manufacturerstakemeasuresto
ensurethattheyareawareofanychangestotheregulatorystatusofthedevicesthattheyproduce.
Such anapproachis, however,infeasibleformembersofthegeneralpublic andevenfor clinicians.
ItwouldclearlynotbeaproductiveuseofFDAresourcesiftheiradministrativestahadtoanswer
repeatedrequestsfromconcernedindividualswhoweresimplywantingtocheckwhetherornotthey
hadreceivedthemostrecentinformationaboutparticulardevices.
Theweboersconsiderablebenetsforthedisseminationofupdatedinformationaboutadverse
occurrencesandnear-missincidents. A singleweb-sitecanactasaclearinghouseforinformations
aboutparticularproducts,suchasTMJs,userscanthenaccessthispageinordertoseewhetheror
nottheinformationthere hadbeenupdated. This approach raisesinterestingquestions aboutthe
relationshipbetweenthereaderandthe regulatoryorinvestigatoryorganisationthat disseminates
theinformation. Inaconventionalpaper-basedapproach,apushmodelofdistributionwasused. The
incident reporting organisation actively sentconcerned individuals updated copies of information
that they had registered an interest in. This enabled regulators to have a good idea about who
read theirreports. Theoverheads associated withthis approach persuaded someorganisationsto
adoptapullmodelinwhichinterestedreadershadtoexplicitlyrequestparticulardocuments. The
dissemination of reports could then be targeted on those who actually wanted them rather than
simply sending everyonea copy of everyreport. The administrativecosts associated with such a
schemehavepersuadedmanyorganisationstoadopttheelectronicvariantofthisapproachinwhich
individuals are expected to pull updated reports from a web page of information. This removes
manyof thecosts associated withthe productionand distribution of paper-basedreports. It also
preventsregulatorsandinvestigatorsfromhavinganyclearideaofwhohasreadtheincidentreports
andassociated publicationsthat theyhaveproduced. Web serverlogs canproveto be misleading,
giventheprevalenceofcacheingandothermechanismsforstoringlocalcopiesoffrequentlyaccessed