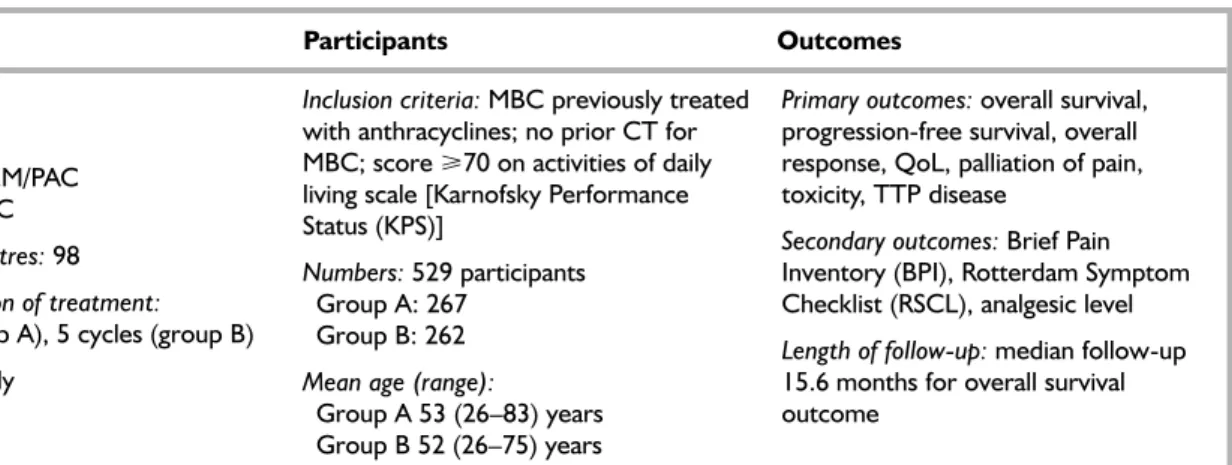
The model assumed a lifelong horizon, which ran until the majority of the cohort was in the absorptive health state (death). The methodological quality of the studies included in the systematic review of clinical effectiveness was assessed by criteria. Metastatic disease was present in 97.0% of the GEM/PAC treatment group and 96.9% of the PAC treatment group.
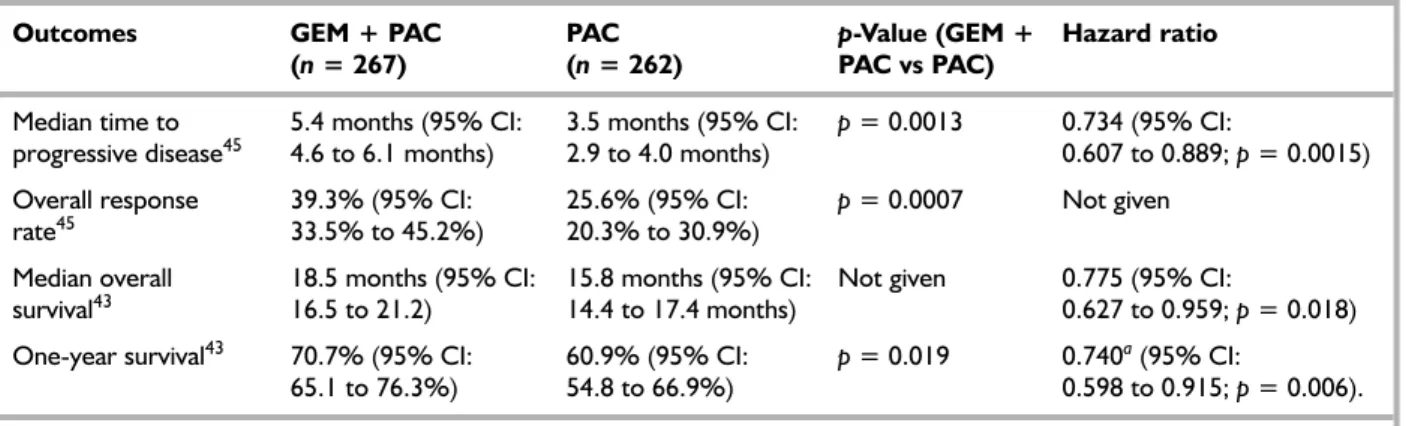
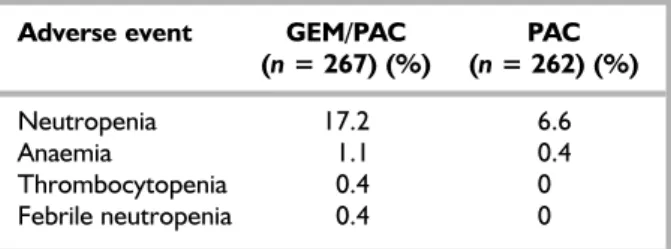
Prior anthracycline therapy was reported to have been given in 96.6% of the GEM/PAC group and 95.8% in the PAC group. Adverse events (AEs) are reported in the summaries of the included RCT and can be seen in Table 4. Survival at 1 year was statistically significantly better in the GEM/PAC group than PAC.
This provides an estimated survival function for the cohort of patients in the PAC arm of the trial. The role of capecitabine, an oral, enzyme-activated fluoropyrimidine, in the treatment of metastatic breast cancer. Cost-effectiveness of letrozole in the treatment of advanced breast cancer in postmenopausal women in the United Kingdom.
Breast cancer staging
No evidence of primary tumor or tumor <2 cm, fixed lymph node positive, no evidence of distant metastases. Tumor of any size with direct extension to the chest wall or skin, negative or positive lymph nodes, no evidence of distant metastases. The review will be undertaken as systematically as time permits, following the general principles outlined in NHS CRD Report 4.41. The research protocol will be updated as necessary as the research program progresses.
Searches will be conducted from the start date of the database to March 2006 and will be limited to the English language. Experts will be contacted for advice and peer review, and to identify additional published and unpublished references. GEM in combination with PAC is the only intervention that will be included in this review as it is the licensed combination.
To isolate the efficacy of GEM in combination with PAC, trials will be excluded if an addn. Participants in the trials to be included in the review are people diagnosed with MBC who were previously treated with anthracyclines. Full economic evaluations of GEM in combination with PAC for the treatment of MBC will be included.
Studies published as abstracts or conference presentations will be included in the primary analysis of clinical and cost-effectiveness if sufficient detail is presented to be made. Data extraction will be undertaken by one reviewer and checked by a second reviewer, with any disagreements resolved through discussion. The quality of included systematic reviews will be assessed using the NHS CRD (University of York) criteria. 41 Quality assessment of RCTs will be assessed in accordance with chapter II.5 of.
Research protocol
Economic evaluations will be assessed using criteria recommended by Drummond and colleagues70 (see Appendix 6) and/or the format recommended and used in the CRD NHS Economic Evaluation Database (CRD Report 6).71. Quality criteria will be applied by one reviewer and checked by another reviewer, with any disagreements resolved through discussion. Clinical effectiveness will be synthesized through a narrative review tabulating results of included studies.
Where data are of sufficient quantity, quality and homogeneity, a meta-analysis of the clinical effectiveness studies will be performed using the Cochrane Review Manager Software. Where QoL data are insufficient to calculate utility estimates in terms of QALYs, data will be derived from the wider literature or estimated from other sources. Published cost-effectiveness studies identified as part of the search strategy documented above will be reviewed in detail, comprising a.
Studies reported in abstract form will be discussed but not reviewed in detail or assessed for quality. Where appropriate, an economic model will be constructed by adapting an existing model or developing a new one, using the best available evidence to estimate the cost-effectiveness of GEM in combination with PAC as second-line treatment for MBC in a UK setting. Data on resource use and costs will come from the published literature and NHS sources where appropriate and available.
Effectiveness data, in terms of the outcomes described above, will be extracted from published studies and used in conjunction with cost data to populate the model. Cost effectiveness will be from the perspective of the NHS and personal social services (costs and benefits). The robustness of the results against the assumptions in the cost analysis and cost analysis.
Documentation of search
Flow chart of inclusion
Paclitaxel plus biweekly gemcitabine in advanced breast cancer: phase II trial and predictive value of the HER2 extracellular domain. Biweekly paclitaxel/gemcitabine in advanced breast cancer: preliminary results of a phase II trial. Results from a phase II study of gemcitabine in combination with paclitaxel in metastatic breast cancer (MBC).
Sanchez P, Medina MB, Mohedano N, Jaen A, Porras I, Gonzalez E, et al. Results of a phase II trial of gemcitabine in combination with paclitaxel in metastatic breast cancer. Preliminary results of an early phase II combination of gemcitabine and taxol in metastatic breast cancer. Salvage treatment with biweekly administration of paclitaxel (P) and gemcitabine (G) in patients (pts) with metastatic breast cancer (MBC) heavily pretreated with regimens containing anthracycline and docetaxel.
Excluded studies
Quality assessment
Was the point of view of the analysis stated and was the study placed in a specific decision-making context? Has a comprehensive description of competing alternatives been given (ie, can you tell who did what to whom, where, and how often). Were the costs and consequences accurately measured in appropriate physical units (eg hours of nursing care, number of doctor visits, work days lost, life years gained).
Where market values were absent (eg volunteer labour), or market values did not reflect actual values (such as clinic space donated at a reduced rate), adjustments were made to approximate market values. Was the valuation of consequences appropriate for the question posed (i.e. was the appropriate type or types of analysis – cost-effectiveness, cost-benefit, cost-utility – chosen). Was the additional (incremental) cost generated by one alternative over another compared to the additional effects, benefits or utilities generated.
If the data on costs and consequences were stochastic (randomly determined sequence of observations), would the appropriate statistical analyzes be performed? If a sensitivity analysis was used, was justification given for the range of values (or for the main parameters of the study). Were the study results sensitive to changes in values (within the . range assumed for the sensitivity analysis, or within the confidence interval about the ratio of costs to consequences).
The presentation and discussion of survey results included all issues of interest to users. Were the conclusions of the analysis based on an overall index or ratio of costs and consequences (eg cost-effectiveness). Did the study address or consider other important factors in the choice or decision under consideration (eg distribution of costs and consequences or relevant ethical issues).
Data extraction form for
Comments: First overall survival analysis by Kaplan-Meier and Cox regression performed at approx. 75% (343) of the deaths needed (440) for the planned final overall survival report. No significant difference was averaged over time between treatment arms in the ITT or symptomatic populations for prespecified outcomes. Also reports that the difference in global QoL as measured by the RSCL was clinically significant.
RSCL: 4 scales to assess QoL, scored 0–100: distress of physical symptoms; psychological distress; activity level; and overall assessment of life (global QoL). Moinpour's PowerPoint presentation states that there was no significant difference in mean time between treatment groups for any scale. Greater improvement was reported by GEM/PAC patients in later cycles for overall life assessment. Significant treatment by time interaction reported in mixed ANOVA; The cycle-specific comparison showed significant.
RSCL Overall Rating of Lifetime Term (GEM/PAC n = 152, PAC n = 162): Cycles 5 and 6 were significantly better for GEM/PAC than baseline and between arms with mixed effects ANOVA. Explanation: States that data from sensitivity analyzes consistently support the findings on the BPI and RSCL. Notes: Dyspnoea appears to be different in the O'Sullivan PowerPoint figure and the Albain PowerPoint - probably means the same thing.
Patients who dropped out early for negative reasons (eg, related to disease progression or toxicity) had worse outcomes. Patients who dropped out late or had positive reasons (e.g. satisfactory response to treatment) had better outcomes. Overall survival data estimated from trial publication was then substituted for OSp(t) in the above equation and log[–logOSp(t)] was regressed against logt.
Model fitting for overall
Equations
Summaries of parameter
Professor Jon Nicholl, Director, Medical Care Research Unit, University of Sheffield, School of Health and Related Research. Professor Deborah Ashby, Professor of Medical Statistics, Department of Environment and Preventive Medicine, Queen Mary University of London. Professor Nicky Cullum, Director of the Center for Evidence-Based Nursing, Department of Health Sciences, University of York.
Professor Miranda Mugford, Professor of Health Economics, University of East Anglia Dr Linda Patterson, Consultant Physician, Department of Medicine, Burnley General Hospital. University of York Professor Kate Thomas, Professor of Complementary and Alternative Medicine, University of Leeds. Professor David John Torgerson, Director of the York Trial Unit, Department of Health Sciences, University of York.
Professor Max Bachmann, Professor of Healthcare Interfaces, Department of Health Policy and Practice, University of East Anglia Professor Rudy Bilous. Professor Jim Neilson, Professor of Obstetrics and Gynaecology, Department of Obstetrics and Gynaecology, University of Liverpool. Professor Scott Weich, Professor of Psychiatry, Division of Community Health, University of Warwick.
Professor Douglas Altman, Professor of Statistics in Medicine, Center for Statistics in Medicine, University of Oxford. ScHARR Deputy Dean, Department of Public Health, University of Sheffield Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge. Senior Lecturer, Department of General Practice and Primary Care, University of Aberdeen, Ms Joan Webster,.