I – Current practices in home mechanical ventilation for chronic obstructive pulmonary disease: a real-world cross-sectional multicentric study. III – Patients' experience of home mechanical ventilation in an outpatient setting Ribeiro C, Jácome C, Oliveira P, Conde S, Windisch W, Nunes R. IV – Long-term health-related quality of life in patients with home mechanical ventilation Ribeiro C, Jácome C, Castro L, Conde S, Windisch W, Nunes R.
VII - Patient perspective and pulmonary function correlates: the importance of questionnaires in home mechanical ventilation.
Abstract
Os objetivos desta tese foram abordar alguns pontos menos pesquisados em relação às medidas de VMD relatadas pelo paciente, tais como: definir as práticas atuais de VMD em pacientes com DPOC, validar a versão em português do questionário S3-NIV, avaliar a experiência de adaptação e acompanhamento ambulatorial dos pacientes -up, analisar a qualidade de vida a longo prazo em doentes com VMD e avaliar o valor preditivo da qualidade de vida relacionada com a saúde e investigar os fatores que condicionam a não adesão aos VMD. A qualidade de vida relacionada à saúde, medida pelo questionário SRI, permanece estável em pacientes com VMD após 5 anos. A diferença entre os pacientes que morreram e os que sobreviveram sugere que o questionário SRI pode ter valor prognóstico e ajudar a prever o estágio final em pacientes com VMD.
Como tal, compreender e melhorar a experiência do paciente VMD é fundamental para alcançar resultados significativos centrados no paciente.
Background
A PREM evaluates the patients' perception of their personal experience of the healthcare service received, while a PROM assesses the perception of their health status and health-related quality of life. The mean score for the SRI-SS was approximately in the middle of the questionnaire's scaling range. It must also be taken into account that the natural history of the diseases leading to CRF and HMV is quite heterogeneous.
Regardless of the setting, once HMV is started, the therapeutic goals should be clear and communicated with the patient.
Aims
Publications
Current practices in home mechanical ventilation for Chronic Obstructive Pulmonary Disease: a real-life cross-sectional multicentric study
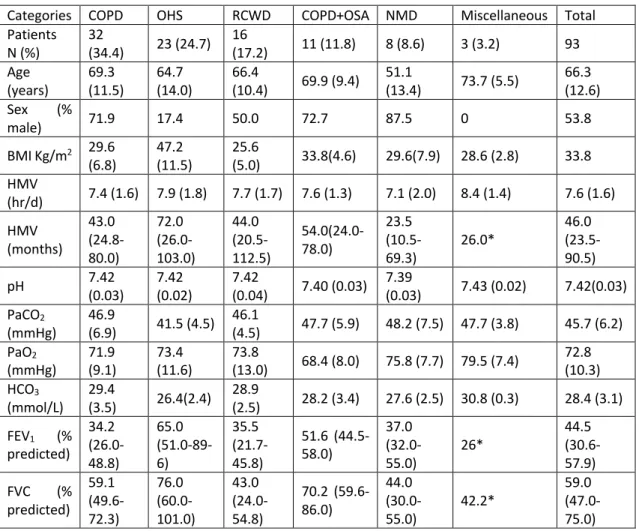
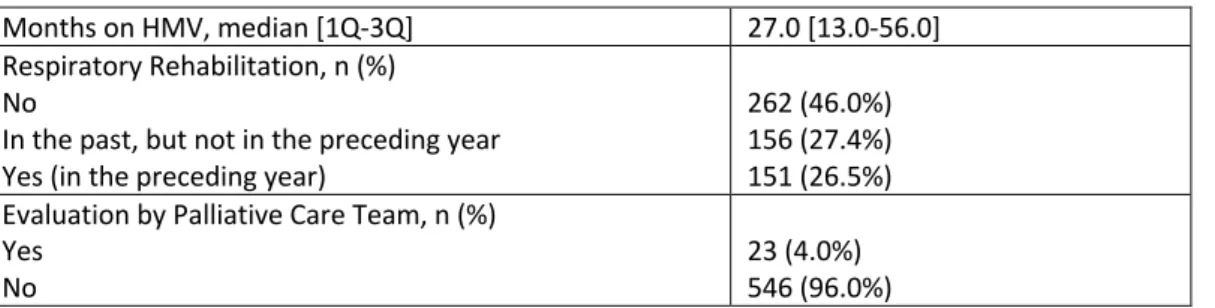
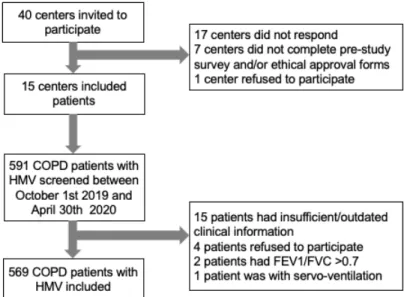
The aim of this study was to provide a detailed description of the current practices and clinical characteristics of patients with COPD at HMV in Portugal. About half of the patients started HMV during or immediately after an exacerbation (49.6%), while the rest were in stable condition. Although more than half of the patients were included in the respiratory rehabilitation program, only about a quarter of them participated in the previous year.
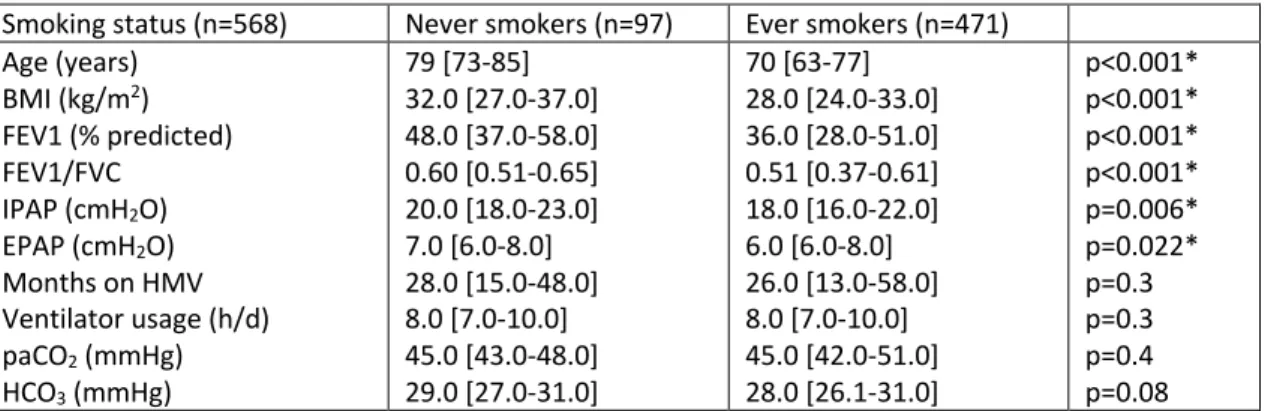
Characteristics of COPD in never smokers and ever smokers in the general population: results from the CanCOLD study.
Transcultural adaptation of the Portuguese version of the S3-Non-invasive Ventilation (S3-NIV) questionnaire for home mechanically ventilated patients
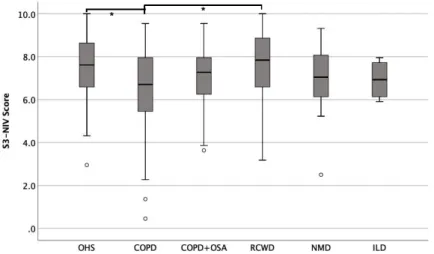
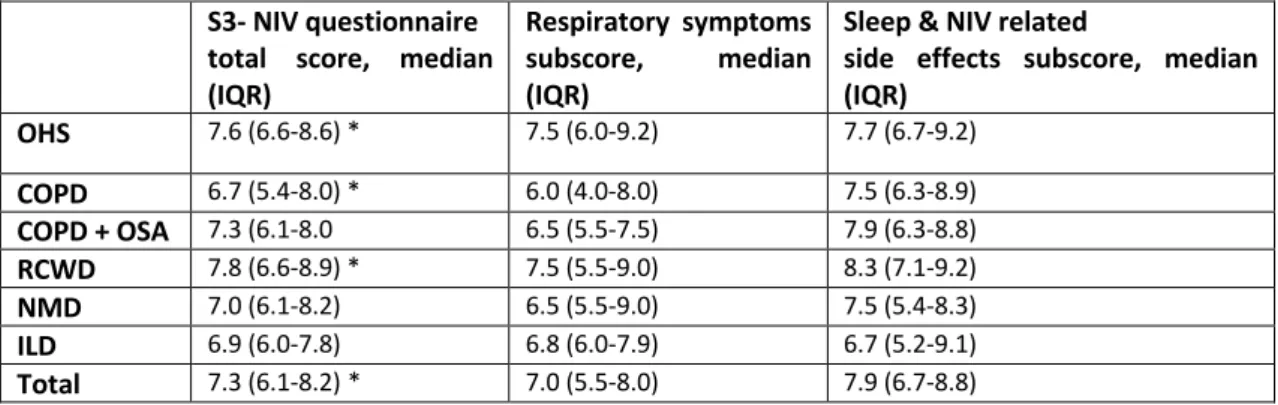
The aim of this study was to produce a professional translation and cultural adaptation of the S3-NIV questionnaire into Portuguese. Considering the translation-back-translation process, all items were graded A except item 10 was graded B for questionable wording - the first translation used the term pressure and it was considered too technical for the patients, and then after trying different wording with colleagues and patients, all authors and translators agreed on the simplified version "the air from the ventilator is too strong". From the 11 items of the scale, eight items (regarding symptoms and sleep) were selected ipsis verbis from the SRI questionnaire, whose Portuguese translation has been externally validated with the SF-36 questionnaire. (11) The remaining items were considered by the authors to be too different from existing questionnaires, and the Quebec Sleep Questionnaire chosen in the original article does not have a validated Portuguese translation and was developed to be used.
This professional Portuguese translation and cultural adaptation of the S3-NIV questionnaire has good psychometric properties and is a simple and valid tool for routine clinical assessment of stable patients with CRF undergoing home NIV.
There was no difference in terms of reported health benefits, side effects, or adjustment time between adjustment settings, but patients who started HMV in the outpatient setting reported better communication and education at adjustment. The development of self-reported questionnaires, namely, patient-reported experience measures (PREMs) and patient-reported outcome measures (PROMs), has grown exponentially over the past several years. The aim of this study was to assess patients' perspectives regarding HMV follow-up in an outpatient setting and to ascertain differences between patients who started HMV in the outpatient setting or elsewhere.
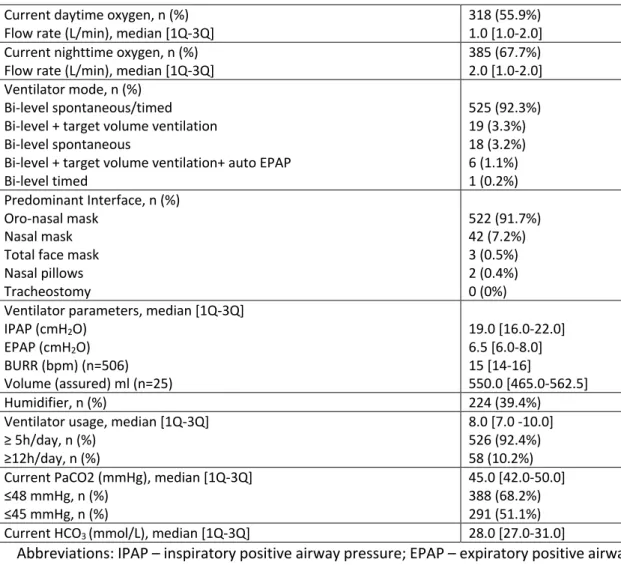
This cross-sectional study was conducted with patients with CRF under HMV recruited between September 2019 and March 2020 in the outpatient ventilation clinic of the Pneumology Department at Centro Hospitalar de Vila Nova de Gaia/Espinho (Portugal), a tertiary care teaching hospital. Patients were excluded if they refused to participate, were unable to understand or answer patient-reported outcomes or if they had an exacerbation in the preceding 3 months. Ventilation parameters and HMV daily use in the previous 3 months were extracted from the readout of the ventilator's built-in software (ResMed AirView® and Philips Care EncoreAnywhere® platforms).
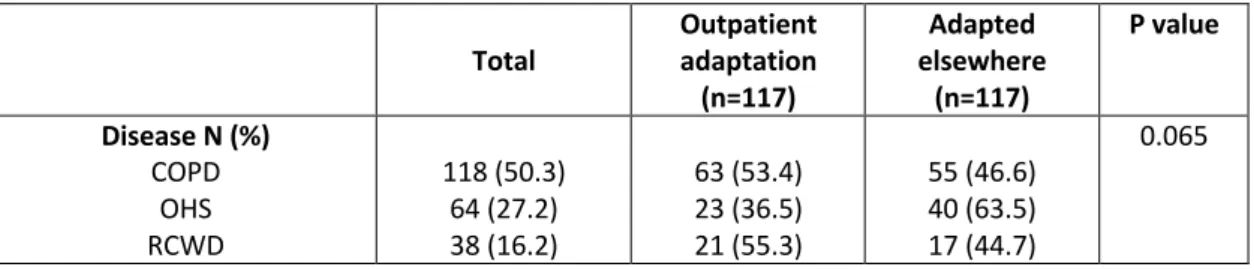
Patients were categorized into two groups: those who were adjusted in the outpatient setting and those who were adjusted elsewhere (hospital ward, emergency department, or home). Comparisons between groups were evaluated through t-test, chi-square, Fisher's exact test. . The non-parametric Mann-Whitney test was used when the parametric assumptions were not valid. Out of 290 patients with HMV followed in the Outpatient Ventilation Clinic in the study period, patients whose characteristics are described in table 1 were included.
We found a difference regarding the location of adaptation within diseases, with neuromuscular disorders (NMD) (66.7%), restrictive chest wall disorders (RCWD) (55.3%) and chronic obstructive pulmonary disease (COPD) (60.4%) being more common in the outpatient clinic compared to OHS (36.5%), this difference was not statistically significant (p=0.065). Patient demographic and clinical characteristics and differences between patients initiated on home mechanical ventilation in the outpatient clinic and elsewhere (n=235).
Factors influencing non-acceptance of home non-invasive ventilation
Home noninvasive ventilation (HNIV) is accepted as the standard of care for patients with chronic hypercapnic respiratory failure (CHRF) due to a variety of conditions [1,2]. Therefore, the current study was aimed at analyzing the factors influencing non-acceptance of HNIV in patients with CHRF. Thirty-nine patients (6.3%) were included in the non-adherent group: 15 patients who refused HNIV and 24 patients who discontinued treatment, of whom 16 abandoned HNIV and 8 with poor adherence ( average: 1h32 0h49/night ), in which treatment was interrupted.
A total of 41 patients started HNIV immediately after the acute exacerbation of patients in the nonadmission group and 32 (41%) patients were well adherent; no significant difference was observed (p=0.655). Univariate analysis found a significant association between non-admission of HNIV and older age, unemployment or retirement, presence of cognitive dysfunction, history of nonadherence to other therapies, and prior history of two or more admissions requiring NIV. . There was no significant association between non-acceptance of HNIV and sex, body mass index, smoking habits, marital status, initial Charlson comorbidity index, or site of NIV initiation (Table 1).
6], which showed good adherence in the elderly population, probably because we detected a higher proportion of patients with cognitive dysfunction in the group that did not receive HNIV. We found that a history of nonadherence to other therapies is an important risk factor for nonadherence to HNIV. A prior history of two or more admissions requiring acute NIV was associated with an increased risk of not receiving HNIV.
Nevertheless, this is a real-world study and one of the few studies evaluating the possible risk factors for non-acceptance of HNIV. In conclusion, older age, a history of nonadherence to other therapies, and a prior history of two or more hospitalizations requiring NIV use are independent factors associated with HNIV nonacceptance.
Patients’ perspective and lung function correlation: the importance of questionnaires in home mechanical ventilation
FVC FVC FVC FVC FVC
ERS International Congress 2021: highlights from the Respiratory Intensive Care Assembly
The sessions we reported on included the symposiums on acute respiratory distress syndrome (ARDS) phenotypes, noninvasive ventilation (NIV) in hypoxic respiratory failure, and new developments in mechanical ventilation and weaning, and the guidelines session on high-flow therapy (HFT) at adults with acute respiratory failure. A randomized crossover study showed that HFT was superior to conventional oxygen therapy in reducing the severity of dyspnea in the first hour of treatment in patients with non-intubated status and hypoxemic respiratory failure [ 17 ]. The PaO2 /FIO2 and the ROX index can be used to classify the severity of hypoxic respiratory failure.
NIV is first-line therapy in COPD patients with acute hypercapnic respiratory failure after a period of medical treatment. Association of non-invasive oxygenation strategies with all-cause mortality in adults with acute hypoxemic respiratory failure: a systematic review and meta-analysis. High-flow nasal oxygen therapy and non-invasive ventilation in the treatment of acute hypoxemic respiratory failure.
Can high-flow nasal cannula reduce the rate of endotracheal intubation in adult patients with acute respiratory failure compared with conventional oxygen therapy and noninvasive positive pressure ventilation. High-flow nasal cannula versus conventional oxygen therapy and noninvasive ventilation in adults with acute hypoxemic respiratory failure: a systematic review. Physiological comparison of high-flow nasal cannula and helmet noninvasive ventilation in acute hypoxemic respiratory failure.
Noninvasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS. ROX index as a good predictor of high-flow nasal cannula failure in COVID-19 patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis.
Highlights from the Respiratory Failure and Mechanical Ventilation 2022 Conference
Validation of the Portuguese Severe Respiratory Insufficiency Questionnaire for home mechanically ventilated patients
- Discussion
- Conclusions and clinical implications
- Future perspectives
- References
Until recently, there was no questionnaire for patients with severe respiratory failure requiring home mechanical ventilation (HMV), regardless of the underlying disorder. It is the aim of the international SRI project to stimulate research activities in the field of HRQL and mechanical ventilation of the house. The mean SRI-SS score (mean 56.6, SD 15.7) was approximately in the middle of the questionnaire's scaling range.
All results were statistically significant except for the correlation between SRI-RC and SF-36 MH. The mean SRI-SS score (56.6) was approximately in the middle of the questionnaire's scaling range. -Related quality of life in patients receiving mechanical ventilation at home: the Spanish version of the severe respiratory insufficiency questionnaire.
When the HMV population was analyzed in the studies, there was a fairly equal distribution by gender, with the exception of the study with only COPD patients. NIV compliance was higher in all diagnostic categories in the Rouen group, with the exception of the NMD category. It has been recognized that the reporting of HMV side effects decreases over time – in a study of the impact of NIV on quality of life there was a 10%.
They also suggest that SRI may be of significant prognostic value and help predict the terminal phase of the disease course in patients on long-term mechanical ventilation at home. The impact of adaptation to HMV in an outpatient setting on outcomes such as quality of life is uncertain.