Alguns fatores de risco cardiovasculares tradicionais são preditores independentes do desenvolvimento futuro de doenças cardiovasculares e a. O escore de risco de Framingham é o método mais comumente utilizado para prever a longo prazo a chance de um indivíduo desenvolver doença cardiovascular (17). Esta pontuação de risco foi validada em diferentes populações e grupos étnicos (31–34) e recalibrada em conformidade, permitindo que esta ferramenta compare o risco entre diferentes grupos populacionais (16).
Homma e colegas (45) investigaram a relação entre formação de placa, aumento da espessura da íntima média da carótida e idade, utilizando um aparelho de ultrassom em indivíduos sem muitos fatores de risco para aterosclerose. Este risco é duas a quatro vezes maior em pacientes com diabetes tipo 2 do que em pacientes não diabéticos, independentemente dos fatores de risco cardiovascular clássicos (145). Os fatores de risco tradicionais para prever doenças cardiovasculares, como o escore de risco de Framingham, fornecem um valor preditivo modesto para eventos cardiovasculares futuros (16).
Portanto, é importante identificar indivíduos com risco aumentado de doenças cardiovasculares e modificar precocemente seus fatores de risco. A avaliação da espessura médio-intimal da carótida e a identificação da placa carotídea podem ser úteis para refinar a avaliação do risco cardiovascular em pacientes de risco intermediário (ou seja, pacientes com risco de 6 a 20% em 10 anos de infarto do miocárdio ou morte por doença coronariana que não não ter doença coronariana). Estas associações entre factores de risco tradicionais para doenças cardiovasculares e espessura íntima-média da carótida sugerem que tem potencial como marcador para prever eventos cardiovasculares (201).
OBJETIVOS
MÉTODOS
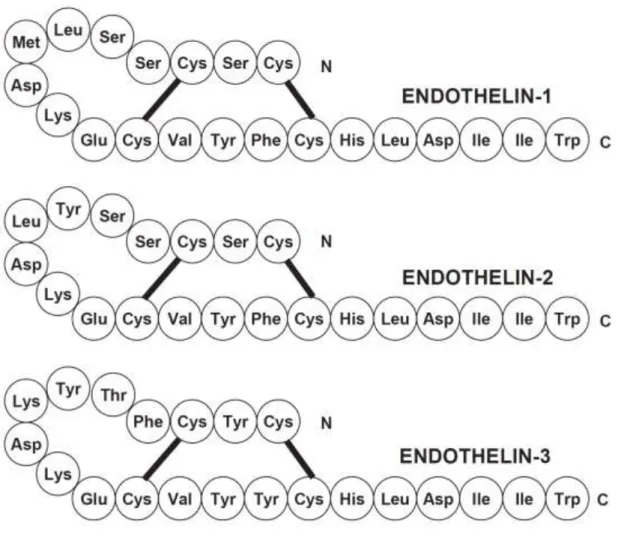
Endothelins
It is produced in small amounts mainly in endothelial cells, acts mainly as an autocrine/paracrine mediator (11) and is continuously released, causing intense smooth muscle contraction, which contributes to the maintenance of endogenous vascular tone (12). However, under pathophysiological conditions, a large number of different cells, including endothelial cells, vascular smooth muscle cells, and inflammatory cells such as macrophages and leukocytes, are stimulated to produce ET-1(11). It is also produced in the heart, kidney, posterior pituitary (13), airway epithelial cells, macrophages, fibroblasts, cardiac myocytes, brain neurons, and pancreatic islets (9).
ET-2 is expressed in the ovarian and intestinal epithelial cells (14) and is known as the vasoactive intestinal contractor. ET-3 is found in brain neurons, renal tubular epithelial cells and intestinal epithelial cells(9) and mediates release of vasodilators(14). ET-4 is found in the intestinal mucosa, lung and kidney epithelial cells and ET1-31 has been discovered in mast cells(9).
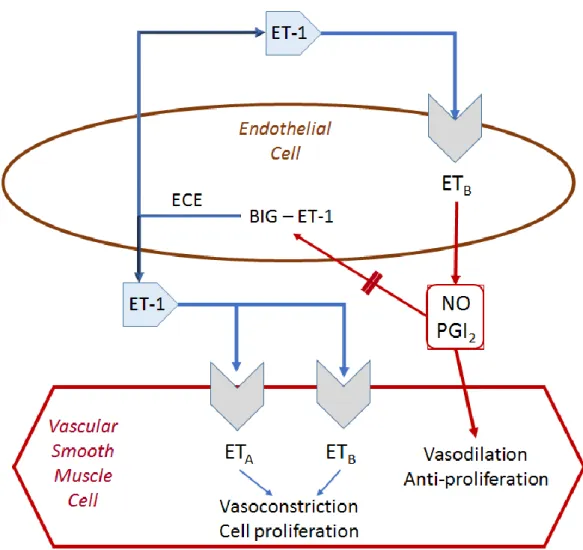
ET-1 is the most abundant and important endothelin produced by vascular cells(15) and it is derived from a 39-amino acid precursor peptide, the pre-proET-1, or. The interaction between ET-1 on endothelial and smooth muscle cells, and the ETA and ETB receptors is shown. ET-1 is derived from the pre-proET-1, or 'big ET-1', which is subsequently cleaved by a family of converting enzymes to pro-ET-1 and then to ET-1.
ETA and ETB receptors are distributed in different tissues and cells, but with different levels of expression (14). In the vasculature, the ETA receptor is found mainly on vascular smooth muscle cells, and the ETB receptor is found mainly on endothelial cells, but is also present on vascular smooth muscle cells (19). Its activation in the endothelium results in the release of nitric oxide and prostacyclin, which cause vasodilation, while stimulation of the ETB receptor in vascular smooth muscle cells causes vasoconstriction (20) (Figure 2).
Many important functions are mediated by activation of ETA and ETB receptors, including vasoconstriction, cardiovascular remodeling, cell proliferation, cell differentiation, extracellular matrix production, and control of water and sodium secretion (22). The ETA receptor appears to be involved in the pathogenesis and development of various diseases such as systemic and pulmonary hypertension, atherosclerosis, diabetes, and cardiac remodeling after myocardial ischemia, while the ETB receptor is classified as a scavenger receptor to prevent ET-1 from stimulating excess of ETA. receptor(23).
Vascular effects of endothelin-1
These molecules can generate reactive oxygen species through the activation of NADPH oxidase, as well as upregulate the activity of transcription factors (such as NF-κB, nuclear factor κB), promoting vascular inflammation that contributes to vascular remodeling and endothelial dysfunction. ET-1 may contribute to vascular dysfunction in aging via multiple pathways, such as direct hemodynamic effects, vascular oxidative stress and inflammatory activity, oxidized low-density lipoprotein uptake, mitogenic stimulation of the vascular smooth muscle cells, and fibrotic processes (26). However, the understanding of the molecular events associated with age-related reductions in endothelium-dependent dilation in humans is unclear(27).
Increased vascular tone is one of the important factors that occur during age-related changes (28). The mechanisms for the increased ET-1-mediated vascular tone with aging include the synthesis of ET-1, the sensitivity or number of ETA/B receptors, and/or changes in the activated pathways through the ET receptors ( 29 ). ET-1-mediated vasoconstrictor tone has been shown to be greater in older men than in young men, but it can be reduced by regular aerobic exercise (30).
In resistance vessels in the human forearm circulation, ET-1 produced a slowly progressive effect, supporting the role of ET in the long-term maintenance of vascular tone ( 31 ). Haynes & Webb (32) showed that endogenous generation of ET-1 contributes to the maintenance of basal vascular tone in humans, in part via ETA receptors. Cardillo et al. (35) showed that blockade of ET-1 receptors improves endothelial-dependent vasodilation in hypertensive patients.
A study using endothelial cells obtained from the brachial artery and peripheral veins showed that ET-1 protein expression is increased in healthy sedentary elderly men and is associated with a reduction in endothelium-dependent dilation. In healthy men, intrabrachial infusion of ET-1 attenuates endothelium-dependent relaxation within 30 min, which can be prevented by coadministration of vitamin C (37). ET-1 has also been implicated in inflammatory processes in the vascular wall through direct activation of macrophages and induction of a number of proinflammatory mediators (39).
Anggrahinite al (39) have demonstrated the role of endothelial cell-derived ET-1 in mediating the recruitment of inflammatory cells and neointima formation induced by carotid artery ligation in mice, thereby promoting the expression of adhesion molecules and the proliferation of vascular smooth muscle cells is stimulated. The ET-1 pathway not only affects vascular hemodynamics but may also be involved in the pathogenesis and progression of several cardiovascular diseases: essential hypertension, atherosclerosis, heart failure, and pulmonary hypertension ( 29 ).

Endothelin-1 and cardiovascular risk factors
- Hypertension
- Diabetes
- Smoking
- Dyslipidemia
The expression of ET-1 and nitric oxide synthase was increased in aging rat arteries (48). Small increases in circulating levels of ET-1 and in functional activity of endothelin-converting enzyme have been observed in very advanced aging in rodents(50). According to Cardillo et al(53), circulating plasma concentrations of ET-1 do not necessarily reflect its vascular effects, but clearance from the blood.
There is also an overproduction of ET-1 in patients with hypertension, chronic renal disease, and diabetes (21). The authors showed that plasma ET-1 is higher in type II diabetes than in type I diabetes, concluding that increased insulin exposure in diabetic patients may have long-term effects on vascular wall structure through stimulation of ET-1 expression (55). . The vascular contribution of ET-1 to hypertension is associated with vasoconstriction and remodeling of resistance vessels, thereby increasing total peripheral resistance.
The role of ET-1 in human hypertension has been investigated by measuring its plasma levels. The implication of ET-1 in hypertension has been controversial and has not been fully elucidated until now. Although some studies have demonstrated an increase in plasma levels of ET-1 in hypertensive patients or animal studies, most studies show unchanged or slightly increased levels (64, 65).
Multiple functions together with predominant expression in vascular tissues suggest that ET alteration may be involved in diseases affecting both the micro- and microvasculature (66). Upregulation of ET-1 by hyperglycemia and insulin has also been demonstrated (77), suggesting that regulation of ET-1 and its receptors may be involved in the vascular complications of diabetes (78). Niemannet al demonstrated an interaction between elevated plasma LDL concentrations and increased ET-1 release in hypercholesterolemic patients, suggesting that oxidized and native LDL stimulate ET-1 production (84).
Studies have shown that a lipid-lowering treatment in patients with hypercholesterolemia reduced the vascular effects of ET-1(89, 90). Moreover, cholesterol-lowering treatment with statins further enhances the beneficial effects of ET antagonism on nitric oxide-mediated vasodilation in hypercholesterolemia (92).
Endothelin Receptor Antagonists
Artigo 2: Relationship between vascular age, arterial stiffness and subclinical atherosclerosis in treated hypertensive patients (Artigo submetido)
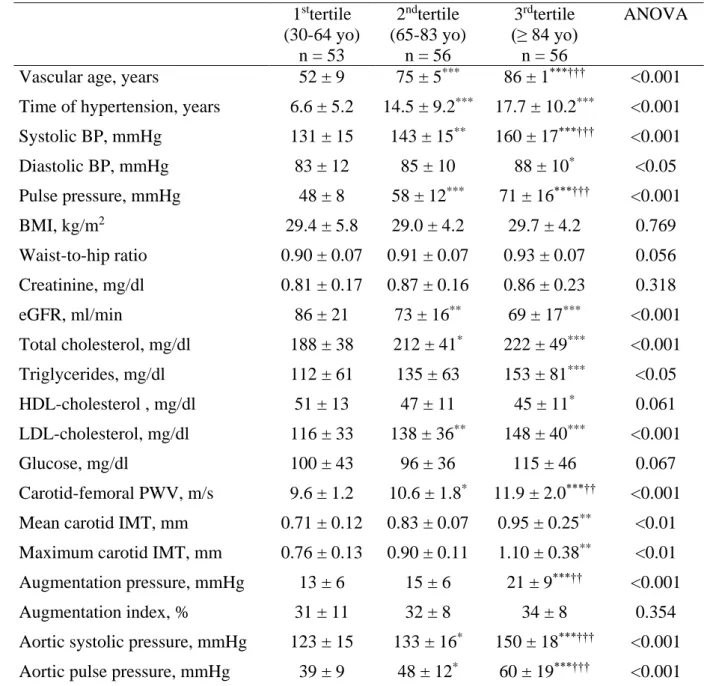
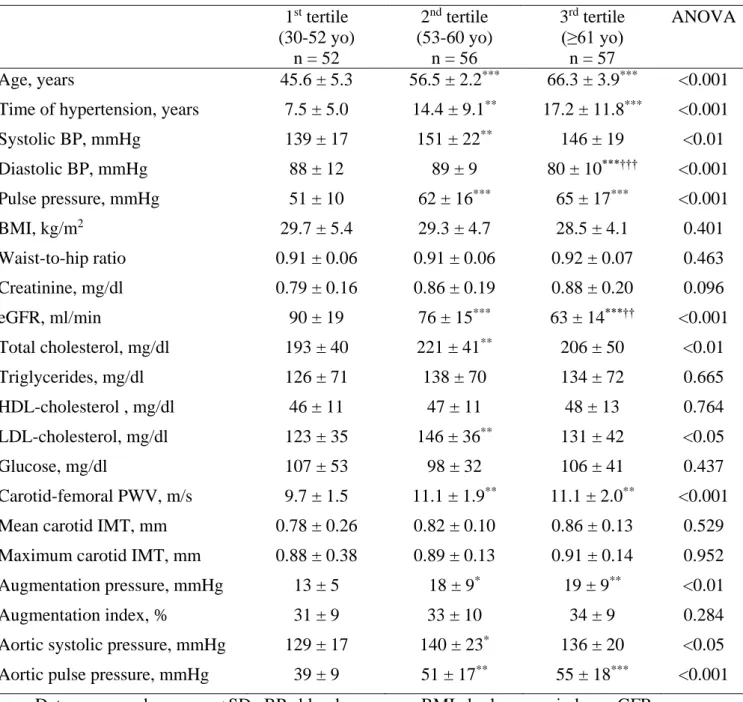
Vascular age was thus formulated according to the general cardiovascular risk score based on the Framingham Heart Study[1]. Afterwards, patients were divided according to tertiles of vascular age estimated by the Framingham risk score. Systolic blood pressure and pulse pressure were progressively higher in groups with higher vascular age.
Likewise, AP, aortic systolic blood pressure and aortic pulse pressure were significantly higher in the groups with increased vascular age (Table 2). In addition, aortic systolic pressure was significantly correlated with vascular age but not with chronological age (Figure 2). Mean chronological and vascular age when patients were divided by aortic systolic blood pressure (Ao SBP; left superior), by pulse wave velocity (PWV; right superior), by mean carotid intima media thickness (cIMT; left inferior), and by maximum carotid intima media thickness (Max cIMT; right inferior).
A moderate correlation of carotid IMT with chronological age was observed, but was stronger with vascular age. The current concept of vascular age evolved with a greater incorporation of the Framingham risk score, which attempted to represent vascular aging in a patient with various cardiovascular risk factors. Our results showed that diastolic blood pressure was progressively lower with advancing chronological age, while pulse pressure increased progressively with advancing tertile of vascular age.
This difference was based on systolic blood pressure behavior, which was similar in the chronological age groups but higher in the advanced vascular age groups. In fact, replacing vascular age with chronological age could increase the Framingham risk score and arterial stiffness was considered a good predictor of increased vascular age [24]. In the current study, both mean and maximum carotid IMT were higher in older groups only when patients were divided by vascular age.
Vascular age: integration of carotid intima-media thickness measurements with global coronary risk assessment. Clin Cardiol 2004;. The thickness of the intima-media of the carotid artery determined the vascular age and the Framingham Risk Score.Crit Pathw Cardiol 2011;.
DISCUSSÃO