As a way to improve public health, the Indonesian government has installed primary health care facilities, Puskesmas, around the country. Future cast and energy projections are used to validate the financial viability of the facility and to estimate the amount of funding required. She believes that laws and policies provide guidelines for and practical implementation of solutions to problems, and always successfully assesses the viability of options.
Introduction
Project Context
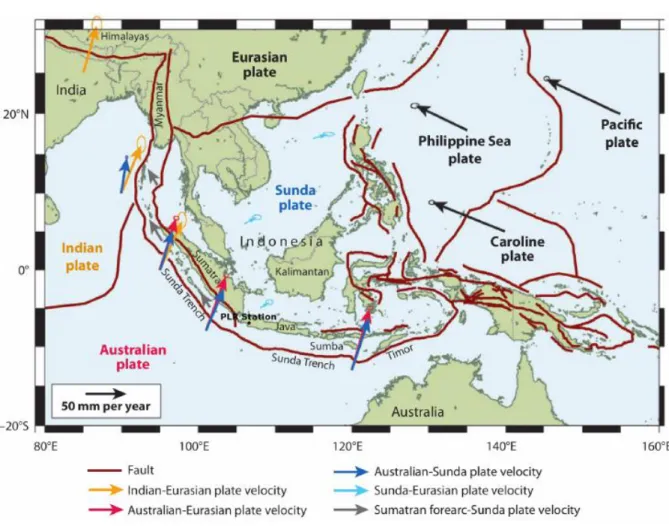
Electricity demand in the province of Bali is currently supplied by the power system in Java through a 150 kV submarine cable transmission network with a capacity of 200 MW. Mini-grids on smaller islands are usually based more on large diesel generators such as those in Batam, Bintan, Lombok and Sumba. Furthermore, even with mini-grids, there are also communities without access to electricity within these islands.
Challenges in Rural Healthcare in Indonesia
Due to the poor network connectivity between the islands and the increased frequency of extreme weather events that hinder the operation of regional networks, constant access to electricity from many regions is limited. Some communities are able to rent small diesel generators, while others still do not have such access. Although it is clear that many modern interventions cannot be performed without electricity, few studies suggest or provide comprehensive explanation or evidence of the links between access to electricity in healthcare facilities and actual health outcomes of treatment.
Impact and Ramifications of the Challenges
Project Backgrounds
Overall Initiatives of the Project
To reduce the discontinuity between development aid and the community, the project directly addresses local health needs by considering the government and current state-run healthcare institutions as the main actors. Therefore, to get ahead of the unreliable power system of Indonesia's local healthcare facilities, we designed a model where a healthcare facility is fully powered by renewable energy, with additional space for public healthcare to provide a clean cooking solution to the local community. As the government and local healthcare facility take initial initiatives to launch the project, they will contribute to improving public health not only by increasing the reliability of the facility's electrical system, but also by reducing mortality from traditional significantly reduce cooking on biomass.
Previous Cases of Reference
The CHP system provided electricity and heat to the medical facility for more than four days after the storm, without reliable grid power. To meet the electrification target, a 1.6kW solar power plant has been installed at the health facility to meet the on-site electricity needs. In addition, the health facility installed a 2.6 kW solar cell to supply clean water to the village.
Community-Based Healthcare Facilities in Indonesia – Puskesmas
In particular, the South Oaks Medical Center campus on Long Island operated on a CHP system for five days when grid power was unavailable. Most recently, the South Oaks Health Care Facility operated off the grid for 15 days, providing all necessary heat and electricity to the 300,000 square foot facility (Health Care Without Harm, 2013). This array powers a pump that pumps water down the hill to a reservoir at the health facility, and the water is then distributed to the community through a pipeline (USAID).
Power Purchase Agreement
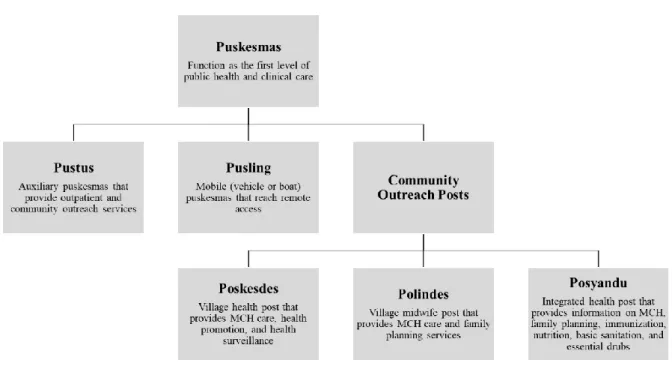
The Puskesmas act as a hub for the implementation of the primary health care delivery strategy with elements of lower level health care, as shown in Figure 3. While the establishment of the Puskesmas network has increased geographic access to primary health care, resource mobilization for the fragmented islands remains a challenge. In this project, we therefore want to provide a comprehensive plan for the provision of general health insurance, starting with the Puskesmas.
Our project solution is to expand the PPA concept in Indonesia to allow certain state health facilities to supply their own electricity and make supply contracts to individual consumers for humanitarian purposes. There are some empirical cases in North America and Europe where healthcare institutions themselves become partners in PPAs that enable on-site energy production. In such cases, energy companies or other investors pay to build and operate a CHP, wind or solar installation at the healthcare facility (WHO, 2014).
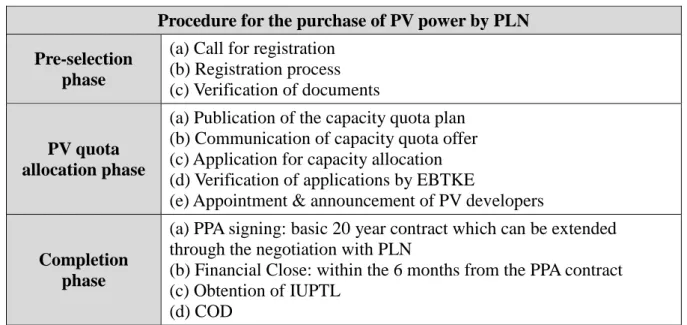
Since the purpose of this project is to improve public health, such a humanitarian initiative may provide sufficient justification for the health facilities to have an independent PPA. Furthermore, the recent proposed solar purchase agreement from PLN in Table 1 validates the feasibility of the project. Under the goal of securing 5,000 MW of solar power generation capacity, the Indonesian government planned to issue gradual solar power project orders and announced a new MEMR Regulation No. 19 of 2016 specifying the required solar power generation capacity and the price to be paid for the electricity supplied.
The selection of PV developers differed from before in that not only energy sellers but any business entity in Indonesia could bid for the capacity quota offer on the first-come-first-served online registration.
Target Setting
Project Overview and Stages
The goal of our project is to propose a new reference model that drives and enhances rural healthcare with renewable energy. We draw up a master plan for transitioning the electricity mix of rural healthcare facilities from diesel to renewable energy. In this section, each stage is described in detail in terms of demand, supply and mix of electricity sources.
Launching Solar Photovoltaics as Substitutional Source of Energy
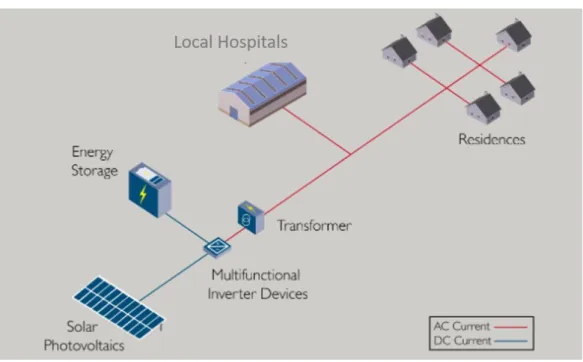
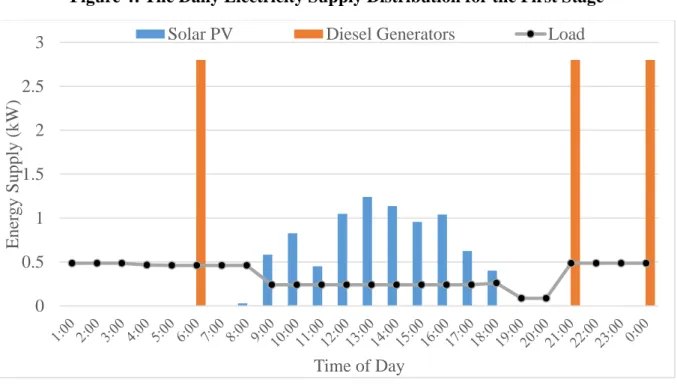
A virtual scenario of the combined power supply set is shown in the figure below. The solar PV will be generated mainly during the day and stored using the Energy Storage System (ESS) to meet the electricity demand in the late night hours.
Introducing Combined Heat and Power System as On-Site Power Generation
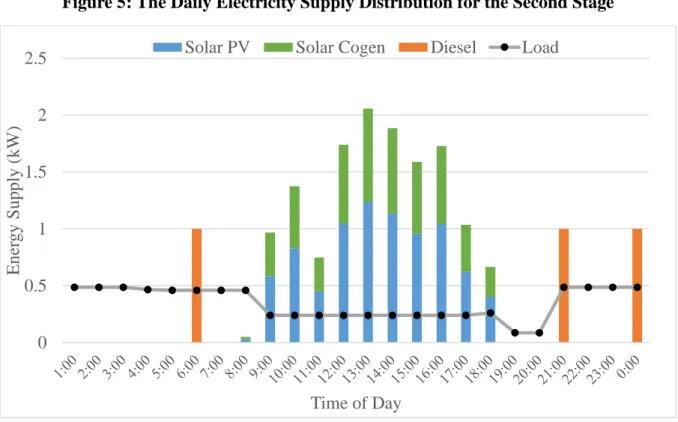
Here, solar energy, in combination with the 3kW solar system, produces around 82% of the health centre's total energy needs. On the other hand, diesel generators will be used to power the remaining 18% of energy needs. As was done in the previous step, we assume that diesel generators are used 3 times a day and produce 1 kWh per day. each, 3 kWh per day.
Advancing Puskesmas into an Inclusive Public Health Space
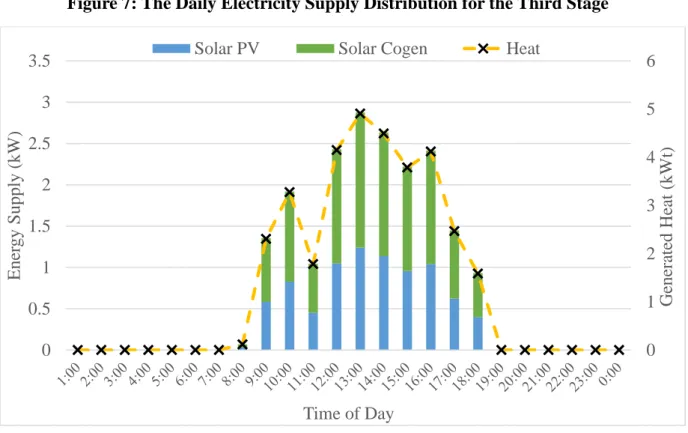
With every kilowatt produced by solar cogeneration plants comes 3 kWh of side-produced heat. The heat energy produced every hour is shown by the yellow dashed lines in Figure 7. All this heat could be sent to the communal kitchen, where it would be used to heat the electric stoves.
The average monthly energy consumption for rural households in Southeast Asia is believed to be 56.73 kWh (Foysal, 2012). If we assume that 50% of this energy is used for cooking (Lloyd & Cowan kWh of heat energy will be needed each day to provide the daily energy for cooking purposes. 33 kWh of the heat generated by the solar cogeneration plants energy easily supplies enough energy to feed 36 households.
Households in Indonesia prefer to build their own stoves rather than buy them, and usually have more than one. Therefore, those for the community kitchen in Puskesmas are estimated to be the highest cost. Despite the high initial costs associated with installing stoves, we can expect a significant reduction in health costs as the death rate associated with biomass cooking will be reduced.
Powering Remote Households with Mini-Grids
Summary of Project Milestones
Verification of the Project
Key Datapoints
In subsequent years and phases, combined heat and electricity generators, including solar photovoltaics, are being installed instead of pure solar PV units. To take advantage of the combined heat and power system for cogeneration, new CHP units are installed at the beginning of the 2nd and 3rd phases of the project. Based on the reference (Mundada, 2016), the cost for a CHP unit is calculated as $7,950, as the sum of the values of solar PV costs, battery costs and.
The annual operating costs are estimated to be double the operating costs of solar panels and reach $545.01. In the project's year 3 (stage 2), 2 cogeneration plants will be installed and in the project's year 6 (stage 3), 2 additional cogeneration plants will be installed. In project year 9 (phase 4), 6 additional cogeneration units are installed to bring the total number of cogeneration units to 10. b) The price of electricity in Indonesia.
PLN is an Indonesian state-owned company that has a monopoly on electricity distribution in Indonesia and generates most of the country's electricity. The cost of electricity supply in the target area is estimated to be one third of this average cost using government subsidies, taking into account the area's capacity and income level. Taking a look at recent mini-grid projects around the world in Table 8 provides an approximate reference of mini-grid capital expenditures (CAPEX).
In conclusion, the total cost of the mini-grids for the project is USD 21,118.9 with project unit multipliers.

Projection of Future Cash and Energy Flows
Conclusion
Increasing access to electricity for the rural community could therefore be the way to improve public health. Our master plan envisages the integration of renewable energy into the operation of the healthcare facility, with combined power generation from solar PV and solar cogeneration plants. The final milestone for the project is the construction of a mini-grid that connects households to provide electricity.
We introduced a full validation for each phase of the project roadmap to prove the robustness and rigor of the proposal. While the financial cost at the start of the project is distributed in external funding and subsidy from the government and multilateral non-governmental organizations, such initiatives are vital to the achievement of the long-term goal of advancing public health and will be offset by increasing surpluses of energy production that is already shown in the projection, and sales from it. In this paper, we explained how building an out-of-network health care facility can benefit public health and local community development, with the financial rationale for the project.
The project has huge implications for the power supply of isolated islands that suffer from the frequent power outages. The successful implementation of the project will build a healthy rural community and move forward in tackling the global health crisis. Retrieved from https://www.wpowerproducts.com/power-generation- resources/diesel-fuel-consumption-chart/2016/bgl.pdf.
Retrieved from https://improvingphc.org/indonesia-puskesmas-and-road-equity-and-access Prinsloo, G., & Dobson, R.