)82(
COPYRIGHT © 2014 BY THE ARCHIVES OF BONE AND JOINT SURGERY
Arch Bone Joint Surg. 2014;2(1): 82-83. http://abjs.mums.ac.ir
the online version of this article abjs.mums.ac.ir
To the Editor
Mardani-Kivi et al presented results about a triple
blinded randomized controlled trial with gabapentin in patients that underwent anterior cruciate ligament (ACL) reconstruction (1). In their manuscript, the introduction section is very illustrative about the subject. With respect to methodology, it is well known that the physical diagnosis of ACL injury is particularly difficult in several patients, and partial ACL tears are also difficult to diagnose on physical examination. In this particular case, how did the authors obtain the diagnosis of ACL in the patients? Likewise, ACL reconstruction can be delayed several weeks or months until the swelling has decreased and there is an appropriate range of motion. For this reason, I want to ask: was the cause of the ACL injury homogeneous in all patients?; was the time delay of the surgery the same for everyone; and was the type of damage the same for all participants?
Meperidine is an opioid with analgesic effects. The American Pain Society and the Institute for Safe Medication Practice (ISMP) do not recommend meperidine use as pain relieving medication or they recommend it only in very special cases and with many precautions during its administration (2, 3). What was the rationale of the authors choosing meperidine as analgesic drug? In this same sense, authors did not indicate in their manuscript whether meperidine was administered by oral, intramuscular or intravenous pathways or patient-controlled analgesia. The time schedule of meperidine administration was not indicate in the manuscript; was meperidine administered q4h or q6h? How many doses were received by patients?
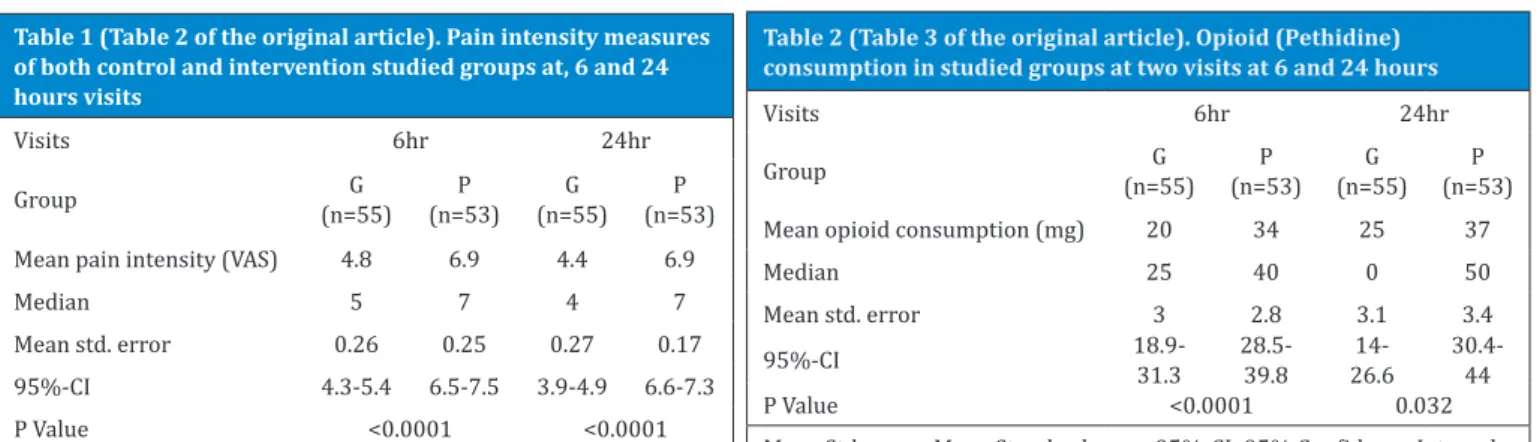
I think it was a mistake to publish the demographic data of all patients (n=114). You had to eliminate the patients deleted in the presentation of the demographic characteristics of the patients (n=108), that is more correct. Table 2 and 3 were poorly prepared. Table 2 has missing data about the results at 24 hours in the placebo group. Table 3 does not specify the meaning of the values (milligrams or administration times or what the units were?)(Table 1, 2).
Finally, pre-emptive analgesia is defined as the treatment that is initiated before and is operational during the surgical procedure in order to reduce the physiological consequences of nociceptive transmission provoked by the procedure (4). Do authors have any idea or hypothesis about the possible mechanism of gabapentin to produce pre-emptive analgesia in your patients? Are the injury and the surgical technique
employed in your study candidate to pre-emptive analgesia? Was the meperidine utilization in your study the better option to get pre-emptive analgesia?
Mario I. Ortiz MD
Luis C. Romero-Quezada MD
A�rea Académica de Medicina del Instituto de Ciencias de la Salud de la Universidad Autónoma del Estado de Hidalgo, Pachuca, Hidalgo, Mexico
LETTER TO THE EDITOR
Analgesic Effect of Gabapentin on
Post-Operative Pain After Arthroscopic Anterior
Cruciate Ligament Reconstruction
References
1. Mardani-Kivi M, Karimi Mobarakeh M, Keyhani S, Hashemi Motlagh K, Saheb Ekhtiari KH. Is Gabapen
-tin Effective on Pain Management after Arthroscopic Anterior Cruciate Ligament Reconstruction? A Tri
-ple Blinded Randomized Controlled Trial. Arch Bone Joint Surg. 2013; 1: 18-22.
2. The Institute for Safe Medication Practices Canada (ISMP Canada). ISMP Canada Safety Bulletin. Meperi
-dine (Demerol®): Issues in Medication Safety. 2004; 4(8).
3. American Pain Society. Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain, 5th ed. American Pain Society. Glenview, Illinois; 2003. 4. Dahl JB, Møiniche S. Pre-emptive analgesia. Br Med
Bull. 2004; 71: 13-27.
In Reply
Dr. Ortiz and Dr. Romero-Quezada evaluated our study precisely and authors are grateful for their great survey on our article. There were some questions and concerns that we are going to answer. We wish it could help others to come up with better ideas and conclusions.
THE ARCHIVES OF BONE AND JOINT SURGERY. ABJS.MUMS.AC.IR VOLUME 2. NUMBER 1. MARCH 2014
)83(
LETTER TO THE EDITOR
almost positive in all cases. 2nd- ACL injury does not conflict with the patient’s routine and social activity and giving way are usually negative and Lachman test can be negative, 1+ and in the most severe condition 2+ positive. Partial ACL tear may be reported in MRI, however authors believe these cases do not benefit from a surgical intervention, and conservative treatment should be performed.
2. Although most of our patients were suffered from sports trauma, mechanisms of ACL tears were not the same in all patients. The duration between traumas to surgeries in all patients enrolled in this study were at least 6 weeks which were included the proceeding from acute trauma phase to performing physical therapy and accomplishing full range of motion pre-operatively. Since the present study was not about surgical technique and pre or post rehab protocols and programs, authors avoided such additional issues.
3. About Pethidine issue, this drug is the main protocol one in our hospital to provide analgesics for post-operative pain, so authors routinely decided to utilize the pethidine as analgesics such as recent relative article (2). We used the pethidine intravenously and by patient’s demand; if a patients requested for pain killers, we provided him/her with 0.5 mg-per-Kg pethidine which was injected intravenously. The time and amount of requested pethidine for every patient were different and patient-dependent and were registered in the medical file for further evaluations.
4. Since randomization was performed prior to surgery, all eligible cases were first randomized in the intervention or control groups. So to our knowledge, primary demographic characteristics were better to contain all eligible case rather than those who remained in the trial. If we would demonstrated the data, as you had commented, one may object that the data is not complete and how can someone be sure about the randomization, so we prefer to put all the data.
5. The criticism about table 2 is correct. The table we have sent to the journal has been probably mis-typed during the publishing process. The original table is attached to the end of this manuscript. Your comment about the table 3 is correct again; it is the mean pethidine consumption during the first 6 and 24 hour
(in milligrams).
6. The main purpose of this study is to apply another agent to decrease the opioid consumption after arthroscopic surgeries such as recent works (3, 4). It was the main reason of utilizing Gabapentin as an adjuvant to the pethidine to evaluate whether it could facilitate the decrease of opioid consumption and its complication.
Finally authors wanted to show their appreciations to Dr. Ortiz and Dr. Romero-Quezada for their precise and meticulous comments.
References
1. Wiertsema SH, van Hooff HJ, Migchelsen LA, Steultjens MP. Reliability of the KT1000 arthrometer and the Lachman test in patients with an ACL rup
-ture. Knee. 2008;15(2):107-10.
2. Bang SR, Yu SK, Kim TH. Can gabapentin help reduce postoperative pain in arthroscopic rotator cuff re
-pair? A prospective, randomized, double-blind study. Arthroscopy. 2010;26(9):106-11.
3. Clarke H, Kirkham KR, Orser BA, Katznelson R, Mit
-sakakis N, Ko R, et al. Gabapentin reduces preop
-erative anxiety and pain catastrophizing in highly anxious patients prior to major surgery: a blinded randomized placebo-controlled trial. Can J Anaesth. 2013;60(5):432-43.
4. Mathiesen O, Moiniche S, Dahl JB. Gabapentin and postoperative pain: a qualitative and quantitative systematic review, with focus on procedure. BMC An
-esthesiol. 2007;7:6. Mohsen Mardani-Kivi MD
Orthopedic Department, Guilan Road Trauma Research Center, Guilan University of Medical Sciences, Rasht, Iran
Table 2 (Table 3 of the original article). Opioid (Pethidine) consumption in studied groups at two visits at 6 and 24 hours
Visits 6hr 24hr
Group (n=55)G (n=53) P (n=55) G (n=53) P
Mean opioid consumption (mg) 20 34 25 37
Median 25 40 0 50
Mean std. error 3 2.8 3.1 3.4
95%-CI 18.9-31.3 28.5-39.8 26.614- 30.4-44
P Value <0.0001 0.032
Mean Std. error: Mean Standard error, 95%-CI: 95% Confidence Interval Table 1 (Table 2 of the original article). Pain intensity measures
of both control and intervention studied groups at, 6 and 24 hours visits
Visits 6hr 24hr
Group (n=55) G (n=53) P (n=55) G (n=53) P
Mean pain intensity (VAS) 4.8 6.9 4.4 6.9
Median 5 7 4 7
Mean std. error 0.26 0.25 0.27 0.17
95%-CI 4.3-5.4 6.5-7.5 3.9-4.9 6.6-7.3
P Value <0.0001 <0.0001