www .e l s e v i e r . c o m / l o c a t e / b j i d
The
Brazilian
Journal
of
INFECTIOUS
DISEASES
Original
article
MRSA
from
Santa
Catarina
State,
Southern
Brazil:
intriguing
epidemiological
differences
compared
to
other
Brazilian
regions
Alessandro
C.O.
Silveira
a,b,∗,
Gabriela
R.
Cunha
a,
Juliana
Caierão
a,
Caio
M.
de
Cordova
b,
Pedro
A.
d’Azevedo
aaLaboratóriodeCocosGramPositivos,UniversidadeFederaldeCiênciasdaSaúdedePortoAlegre,PortoAlegre,RS,Brazil
bDepartamentodeCiênciasFarmacêuticas,Fundac¸ãoUniversidadeRegionaldeBlumenau,Blumenau,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30October2014 Accepted22April2015 Availableonline25June2015
Keywords:
Antimicrobialresistance Vancomycin
Oxacillin
a
b
s
t
r
a
c
t
Methicillin-resistantStaphylococcusaureus(MRSA)isoneofthemostfrequently isolated agentsinbothnosocomialandcommunitysettings.Itisaconstantchallengefor antibac-terialtherapy.Therefore,itbecomesessentialtounderstandtheepidemiologyofMRSA isolatesintheinstitutionand/orregiontoguideempiricaltherapy.Theobjectiveofthisstudy wastoevaluatetheepidemiologicalcharacteristicsofMRSAisolatesinthestateofSanta Catarina,Brazil,anddetermineifthereisaclonalspread.Weevaluated124clinicalisolates ofMRSAobtainedfromvariousanatomicalsitesfrompatientsinthestateofSantaCatarina inSouthernBrazil.Theantimicrobialsusceptibilityprofilewasevaluatedbydiskdiffusion andminimuminhibitoryconcentration(MIC)wasdeterminedbyEtestandbroth macrodi-lution.SCCmectypesweredeterminedbymultiplexPCRandtheclonalrelationshipamong isolateswasassessedbypulsedfieldgelelectrophoresis.Antimicrobialsthathave demon-stratedlowerratesofresistanceweretetracycline(20.2%),sulfamethoxazole–trimethoprim (20.2%)andchloramphenicol(12.9%).Wedidnotdetectanyresistancetoglycopeptides, daptomycin,linezolid,andtigecycline.SCCmectypeIIIwaspredominant(54%),followed bytypeII(21.8%),consistentwithotherBrazilianstudies.Twenty-sixcloneswereobserved grouping72(58%)isolatesandnoclonalrelationshipwasobservedbetweenourisolatesand themajorepidemicclonescirculatinginBrazil.AnintriguingdistinctMRSAepidemiology wasobservedinSantaCatarina,comparedtootherBrazilianregions.
©2015ElsevierEditoraLtda.Allrightsreserved.
Introduction
Staphylococcusaureusisamajoragentofcommunity-acquired infectionsandhealthcareassociatedinfections.Amulticenter
∗ Correspondingauthor.
E-mailaddress:[email protected](AlessandroC.O.Silveira).
studyamongBrazilianhospitalsduring2005–2008foundthat S.aureuswasthemainagentofbloodstreaminfections(20.2%) and infections of the skin and soft tissue (28.1%)and the second most common agentin pneumoniaofhospitalized
http://dx.doi.org/10.1016/j.bjid.2015.04.009
patients(24.9%).Oftheseinfections,approximately30%were resistanttomethicillin(MRSA).1
Staphylococcibecomeresistanttomethicillinbychanging transpeptidasesinthewall,calledpenicillin-bindingproteins (PBPs),andloseaffinityforall-lactamagents.This informa-tioniscontainedinthemecAgeneresponsibleforencoding analteredPBP(PBP2a).2,3
Until the early 1990s, MRSA isolates were restricted to hospitals.Currently,however,MRSAisnolongerexclusively associated with healthcare infections. During this period, increase in community-acquired MRSA (CA-MRSA) among patientswithoutassignableriskfactorsforacquiringMRSA wasobserved(i.e.,hadnodirectorindirectcontactwithhealth servicesthatcouldassociatetheMRSAinfectionwithhealth care).4
Sincethen,areversephenomenonbegantooccur: com-munity isolates, once characterized by the presence of a staphylococcalcassettechromosome(SCCmec)typeIV,began to be isolated in hospital settings and those types that were typically isolated in the hospital began to appear in outpatients.5,6
AstheepidemiologyofMRSAprovedtobedynamic,itis importanttogeneratedatatobetterunderstandtheevolution ofthisepidemiologicalbehaviorandtoassessitsimpacton clinicalsettings.7SantaCatarinaStatehasanintriguinglow prevalenceofMRSAcomparedtootherBrazilianStatesand understandthisepidemiologicaldynamicswouldbevaluable. Theobjectiveofthisstudywastoevaluatethe epidemio-logicalcharacteristicsofMRSAisolatesinthestateofSanta Catarina.
Methods
Bacterialsamples
Weused 124 clinical MRSA isolatesobtained from various anatomicalsitesfrompatientsattendedintwocities (Blume-nauandFlorianopolis),locatedintheStateofSantaCatarina, Southern Brazil. Samples were collected from November 2009 through February 2013. One isolate per patient was considered.Sampleswereselectedbyconvenience. Identifica-tionwasdoneusingstandardizedphenotypicmethodology8 and isolateswere maintained frozen(−20◦C) inskim milk
(DIFCO®)plus10%glycerol.
Antimicrobialsusceptibilitytesting
Antimicrobialsusceptibilitytestingwasperformedusingthe disk diffusion method, according to the recommendations and interpretative criteria of the Clinical and Laboratory Standards Institute9 and European Committee on Antimi-crobial Susceptibility Testing (to tygecycline only).10 The antimicrobialstestedweregentamicin(10g),ciprofloxacin (5g), erythromycin (15g), clindamycin (2g), trimetho-prim/sulfamethoxazole (1.25g/23.75g), chloramphenicol (30g), tetracycline (30g), teicoplanin (30g), tigecycline (10g),and linezolid(30g).MRSAwascharacterizedusing thecefoxitindisk(30g),andconfirmedbyPCRforthegene mecA.11Todetect-lactamaseproduction,weusednitrocefin
disk(BDBBLTMDrySlideTMNitrocefin),usingbacterial suspen-sionsinphysiologicalsaline.S.aureusATCC29213wasused asapositivecontrol,andS.aureusATCC25923wasusedasa negativecontrol.
MICdetermination
Vancomycin MICs were determined by macrodilution method9 and byEtest® (BioMérieux,Marcy l’Etoile,France) followingCLSIinterpretativecriteria9andthemanufacturer’s instructions, respectively. MICs for teicoplanin and dapto-mycin were determined by Etest®. S. aureus strains ATCC 29213(MSSA),ATCC43300(MRSA),ATCC700698(hVISA)and ATCC700699(VISA)wereusedforqualitycontrol.
MultiplexPCR
TheSCCmectypewas determined usingthe multiplexPCR methodaccordingtotheprotocoldevelopedbyZhangetal.12 Theamplicons thatwere formedhadthe followingsizes:I (613bp),II(398bp),III(280bp),IVa (776bp),IVb(493bp),IVc (200bp),IVd(881bp),andV(325bp).12,13
Forisolatespresentingphenotypicinducibleresistanceto clindamycin,ermgenewasassessedbyamultiplexPCR proto-col,describedelsewhere.14ThePCRproduct(610bpforermA and520bpforermC)wasanalyzedbyelectrophoresisthrough a1.5%agarosegel.14,15
Pulsed-fieldgelelectrophoresis(PFGE)
PFGEwasperformedaccordingtoMcDougaletal.16andPinto et al.17 The fragments were subjected to PFGE using 1% agarosegels(PulsedFieldCertifiedAgarose;Bio-Rad)in0.5×
Tris–borate–EDTAbufferwithaCHEF-DRIIIsystem(Bio-Rad). Gels were stained with 0.5g/mL ethidium bromide, visu-alizedunderUVlight,and photographedusing aGelDocTM XR System (Bio Rad). PFGE patterns were analyzed using Bionumericsversion6.1(AppliedMaths,Sint-Martens-Latem, Belgium)andclusteredbyUPGMA.Adendrogramwas gen-erated from a similarity matrix calculated using the Dice similaritycoefficientwithanoptimizationof0.5%anda tol-eranceof1%.PFGEclustersweredefinedasisolateswitha similarityof80%orhigheronthedendrogram.18SCCmec con-trolstrainswereincluded[typeI(NCTC10442);typeII(N315); typeIII(85/2082);typeIVa(CA05);typeIVb(8/6-3P);typeIVc (MR108);typeIVd(JSC4469)andtypeV(WIS)],aswellas iso-latesofthemaincirculatingepidemicclonesinLatinAmerica (BrazilianEpidemicClone,NewYork/Japan,USA300,USA400, Pediatric,OSPC,Cordobean,E-MRSA15,E-MRSA16).
Results
MIC Vancomycin
A
B
MIC TeicoplaninNumber of isolates Number of isolates
MIC (μg/mL) MIC (μg/mL)
60
50
40
30
20
10
0
10 20 30 35 40 50
45
25
15
0 5
0.5 0.75 1.0 1.5 2.0 3.0 0.19 0.25 0.38 0.5 0.75 1.0 1.5 2.0 3.0 4.0 6.0 8.0 12.0
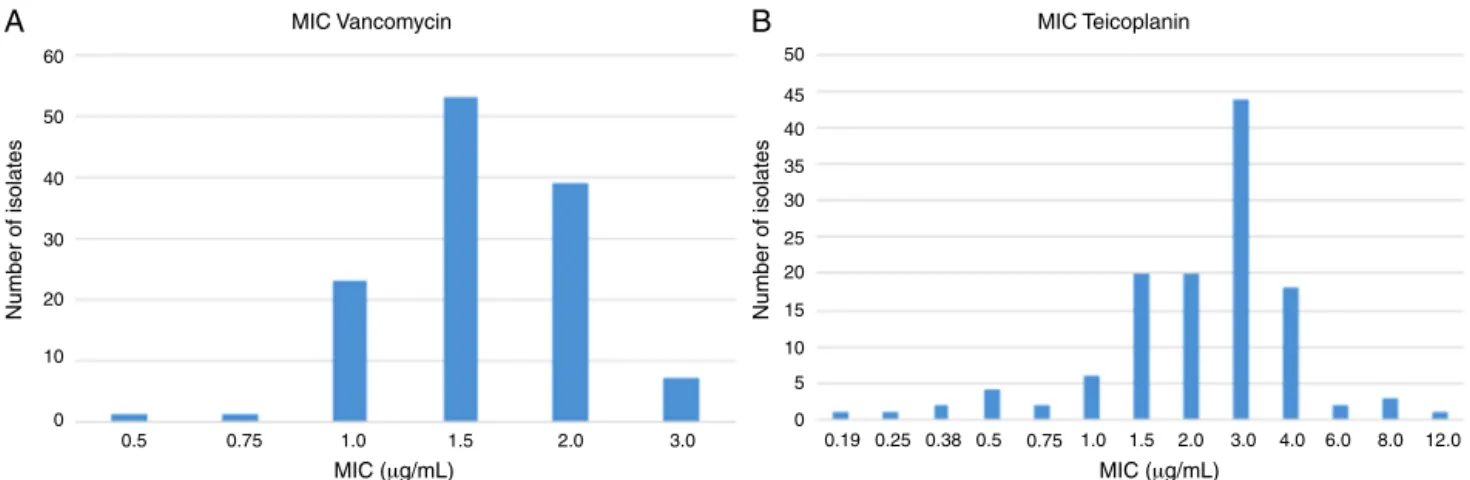
Fig.1–MICoftheglycopeptidesto124MRSAdeterminedbyEtest.In(A),thevaluesobtainedforvancomycin.Theseven isolateswithMICof3.0g/mLwereconsideredsusceptiblebecauseallMICswere≤2.0g/mLbymicrodilution.In(B),the resultsforteicoplanin.Oneisolate(MIC12g/mL)whentestedbymicrodilutionyieldedanMICof4.0g/mL(susceptible).
(13.7%)wereconsideredcommunityisolatesand107(86.3%) hospitalisolates.
MRSApresentedthefollowingresistancerates:amikacin (35.5%),gentamicin (33.1%),chloramphenicol (12.9%), tetra-cycline (20.2%), ciprofloxacin (79%), norfloxacin (72.6%), sulfamethoxazole–trimethoprim(20.2%), clindamycin(75%), and erythromycin (81.5%). Also, 93 strains (75%) showed productionof-lactamase.All isolates were susceptible to linezolidandtigecycline.
AllisolatesweresusceptibletovancomycinandMICsare presentedinFig.1.SevenisolatesshowedMICof3.0g/mLby Etest.BymacrodilutionthreeofthemshowedMICof1.0g/mL andfourhadMICof2.0g/mL.Etestalsooverestimated(above CLSIsusceptibilitybreakpoint)teicoplaninMICforoneisolate butmacrodilutiondefineditsMICas4g/mL(susceptibleby CLSIinterpretativecriteria).
Daptomycin,analternativetoglycopeptidesforthe treat-mentofinfectionscausedbyMRSA,showedMCIvalueswithin the susceptibility range (Fig. 2), even though four isolates presentedMICof1.0g/mL(upperlimitofsusceptibility cate-gory).
AlthoughpredominantSCCmecwastypeIII(54%,67/124), therewasaheterogeneousdistributionofSCCmectypes:type II(21.8%),typeIVa(10.5%),typeIVc(3.2%)andtypeIVb(2.4%). FiveisolatescarriedtypesIandIItogether.AmongCA-MRSA
MIC Daptomycin
Number of isolates
MIC (μg/mL)
0 5 10 20 30 40 45
35
25
15
0.125 0.19 0.25 0.38 0.5 0.75 1.0
Fig.2–MICsfordaptomycindeterminedbyEtest.All isolateswereconsideredsusceptible(MIC≤1.0g/mL).
(n=17),onlyfourshowedSCCmectypeIV:twoIVaandtwoIVb. Amongtheother13isolates,eighthadSCCmectypeIIIandfive hadtypeII.
Ofthe124isolates,23(18.5%)hadapositiveDtest:20(87%) had ermAgeneandthree(13%)carriedermC.Twelve(9.7%) isolatespresentedresistancetoerythromycinand suscepti-bilitytoclindamycin(negativeDtest)andhadnopositivePCR reaction.Fifty-six(45.1%)isolateshavehadconstitutive resis-tancemechanismandonly33(26.6%)weresusceptibletoboth antibiotics.
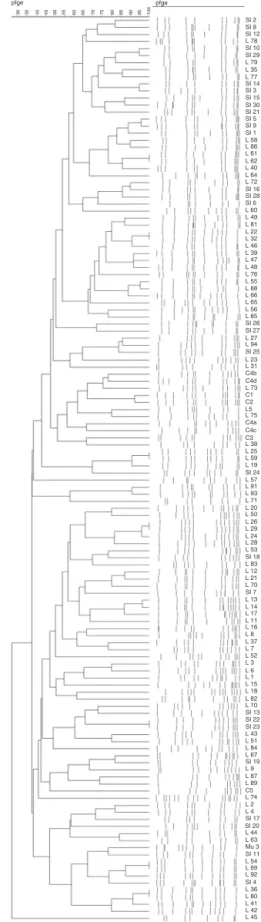
Twenty-sixclones(Fig.3)wereobserved,grouping72 iso-lates(withfivebeingthehighestnumberofisolatesperclone). Indeed, 52 isolates presented a unique pulsotype. Isolates belongingtoallclonescarriedSCCmectypeIII(Table1).
Discussion
The prevalence of MRSAin the state ofSanta Catarina is extremely lowandiscomparabletoratesfoundin Scandi-naviancountries.2,19,20Isolationratesareintherangeof4–8% forallisolatedS.aureusandtheseratesareevenlowerwhen onlynosocomialisolatesareconsidered(lessthan2%).Such lowoccurrenceofMRSAjustifiestheintriguinglownumberof MRSAincludedinthisstudy,asthetwomostpopulouscities ofSantaCatarinawereincluded.Inareportpublishedbythe WorldHealthOrganization(WHO),severalEuropeancountries havenationalsurveillancedatawithverylowratesofMRSA: Denmark(1.2%),Estonia(1.7%),Finland(2.8%),Iceland(2.8%), Netherlands(1.4%),Norway(0.3%)andSweden(0.8%).21These countriesmayhavesucceededinmaintaininglowMRSArates becauseofeffectivesearch-and-destroypoliciesand/or con-trolled antibioticoveruse.22 Ofnote, occurrenceofMRSAin Santa Catarina differsgreatly from other regions ofBrazil, whichhave,ingeneral,MRSAratesofaround29%.23,24Asfar asweknow,thosesearch-and-destroypoliciesarenot prac-ticedinSantaCatarinaand,surprisingly,MRSAisolationrates aresimilartothosefoundintheScandinaviancountries.
SI 2 pfge pfge SI 8 SI 12 SI 10 SI 29 SI 14 SI 3 SI 15 SI 30 SI 21 SI 5 SI 9 SI 1 SI 16 SI 28 SI 6 L 78 L 79 L 35 L 77 L 58 L 86 L 61 L 62 L 40 L 64 L 60 L 49 L 81 L 22 L 32 L 46 L 39 L 47 L 48 L 76 L 55 L 88 L 66 L 56 L 85 L 27 L 94 L 23 L 31 L 73 C1 C2 L5 L 75 C4b C4a C4c C3 L 38 L 25 L 59 L 19 L 57 L 91 L 93 L 71 L 20 L 50 L 26 L 29 L 24 L 28 L 53 L 83 L 12 L 21 L 70 L 13 L 14 L 17 L 11 L 16 L 8 L 37 L 7 L 52 L 3 L 6 L 1 L 15 L 18 L 82 L 10 L 43 L 51 L 84 L 67 L 9 C5 L 87 L 74 L 2 L 4 L 44 L 63 Mu 3 SI 11 SI 4 L 54 L 69 L 92 L 36 L 80 L 41 L 42 L 45 SI 17 SI 20 L 89 SI 19 SI 13 SI 22 SI 23 SI 7 SI 18 SI 24 C4d SI 26 SI 27 SI 25 L 65 L 72
Fig.3–DendrogramillustratingthePFGEpatternsof124 strainsandcontrols.Twenty-sixcloneswereobserved.
studieswithsimilarcharacteristics,whichdemonstratea pre-dominanceofbloodstreaminfections(39%)25orskinandsoft tissueinfections(61.5%).26
Compared tothe antimicrobialsurveillance in the mul-ticenter study SENTRY,1 resistance rates in this study were much lower: ciprofloxacin (91.4–79%), tetracycline (46.7–20.2%), trimethoprim–sulfamethoxazole (68.1–20.2%), clindamycin(87.9–75%)anderythromycin(94–81.5%).A pos-sible explanation for the large differences in rates of susceptibility could be due to the epidemiological profile. Cavalcante et al. proposed phenotypic markers associ-ated with SCCmec types. Resistance to tetracycline and trimethoprim–sulfamethoxazole may be associated with SCCmectypeIII,inwhich100%resistancewasfoundtoboth drugs.SCCmectypeIVhadabsolutesusceptibility,withonly 2%oftheisolatesresistanttotrimethoprim–sulfamethoxazole and100%susceptibilitytotetracycline.27Wefounda predom-inanceofSCCmectypeIII,whichjustifieswhytheresistance ratesinourstudywerelowerthanthosefoundintherestof Brazil.
Thepresenceof-lactamasemayresultinunusual phe-notypesknown asBORSA (BorderlineOxacillin ResistantS. aureus).Thesebacteria,despitelackingthemecAgene,may be resistant to oxacillin and are phenotypically character-ized asMRSA.28 They mayalsoberesponsible forelevated MICsofoxacillin.Aftertherapywith-lactams,these bacte-riamay inducethedevelopmentofvancomycinresistance, aphenotypecalled-lactamantibiotics-inducedvancomycin resistantS.aureus(BIVR).29
AllMRSAweresusceptibletovancomycin,teicoplaninand daptomycin.Althoughthephenotypeofresistancetothese drugs is uncommon.30 31.45% of the isolates showed MIC of2.0g/mLforvancomycin,whichmaysuggestthe devel-opmentofaphenomenonofanupwardtrendforMICsfor vancomycin,called“MICcreep”.31
TheisolatesdemonstratedhigherprevalenceofgeneermA thanermC.TheDtestprovedtobeamethodologycapableof detectingallisolateswithinducibleclindamycinresistance. Therefore,thetestiseasytoperform,inexpensiveandis clin-ically relevant becauseit reducesthe riskof inappropriate antibioticsuse.32
Inourstudy,therewasahighprevalenceofSCCmectypeIII (54%).In2010,astudyconductedattheHospitaldeClinicasde PortoAlegre(capitaloftheneighboringstateofRioGrandedo Sul),ahighprevalenceofSCCmectypeIIIwasdetected(49%),33 similartoourfindings.In2005,incontrasttothelocal epi-demiology,astudyconductedattheHospitaldeClinicasde SãoPaulofoundthat65%ofMRSAcarriedSCCmectypeIV.34
Notsurprising,ourisolatesdidnotpresentaclonal dis-semination,asbothcities(FlorianopolisandBlumenau)are separatedbyapproximately120kmandtheisolateswere col-lectedduringaperiodofthreeyears.
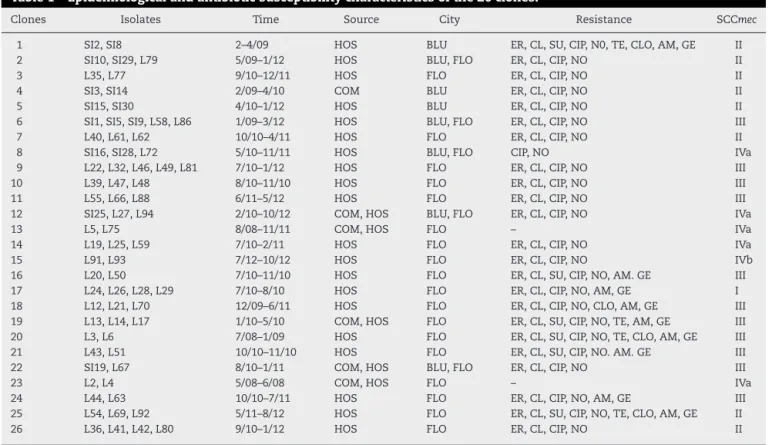
Table1–Epidemiologicalandantibioticsusceptibilitycharacteristicsofthe26clones.
Clones Isolates Time Source City Resistance SCCmec
1 SI2,SI8 2–4/09 HOS BLU ER,CL,SU,CIP,N0,TE,CLO,AM,GE II 2 SI10,SI29,L79 5/09–1/12 HOS BLU,FLO ER,CL,CIP,NO II
3 L35,L77 9/10–12/11 HOS FLO ER,CL,CIP,NO II
4 SI3,SI14 2/09–4/10 COM BLU ER,CL,CIP,NO II
5 SI15,SI30 4/10–1/12 HOS BLU ER,CL,CIP,NO II
6 SI1,SI5,SI9,L58,L86 1/09–3/12 HOS BLU,FLO ER,CL,CIP,NO III 7 L40,L61,L62 10/10–4/11 HOS FLO ER,CL,CIP,NO II 8 SI16,SI28,L72 5/10–11/11 HOS BLU,FLO CIP,NO IVa 9 L22,L32,L46,L49,L81 7/10–1/12 HOS FLO ER,CL,CIP,NO III 10 L39,L47,L48 8/10–11/10 HOS FLO ER,CL,CIP,NO III 11 L55,L66,L88 6/11–5/12 HOS FLO ER,CL,CIP,NO III 12 SI25,L27,L94 2/10–10/12 COM,HOS BLU,FLO ER,CL,CIP,NO IVa
13 L5,L75 8/08–11/11 COM,HOS FLO – IVa
14 L19,L25,L59 7/10–2/11 HOS FLO ER,CL,CIP,NO IVa
15 L91,L93 7/12–10/12 HOS FLO ER,CL,CIP,NO IVb
16 L20,L50 7/10–11/10 HOS FLO ER,CL,SU,CIP,NO,AM.GE III 17 L24,L26,L28,L29 7/10–8/10 HOS FLO ER,CL,CIP,NO,AM,GE I 18 L12,L21,L70 12/09–6/11 HOS FLO ER,CL,CIP,NO,CLO,AM,GE III 19 L13,L14,L17 1/10–5/10 COM,HOS FLO ER,CL,SU,CIP,NO,TE,AM,GE III 20 L3,L6 7/08–1/09 HOS FLO ER,CL,SU,CIP,NO,TE,CLO,AM,GE III 21 L43,L51 10/10–11/10 HOS FLO ER,CL,SU,CIP,NO.AM.GE III 22 SI19,L67 8/10–1/11 COM,HOS BLU,FLO ER,CL,CIP,NO III
23 L2,L4 5/08–6/08 COM,HOS FLO – IVa
24 L44,L63 10/10–7/11 HOS FLO ER,CL,CIP,NO,AM,GE III 25 L54,L69,L92 5/11–8/12 HOS FLO ER,CL,SU,CIP,NO,TE,CLO,AM,GE II 26 L36,L41,L42,L80 9/10–1/12 HOS FLO ER,CL,CIP,NO II
HOS,hospital;COM,community;BLU,blumenau;FLO,florianopolis;ER,erythromycin;CL,clindamycin;SU,trimethoprim/sulfamethoxazole; CIP,ciprofloxacin;NO,norfloxacin;TE;tetracycline;CLO,chloramphenicol;AM;amikacin;GE,gentamycin.
Conclusions
AlthoughweidentifiedtheSCCmecthatwerepresentand eval-uatedthepresenceofclones,thepresentstudydidnotprovide consistentscientificevidenceforthelowprevalenceofMRSA inSanta Catarina, whichwas very different from the data foundinotherBrazilianstatesandsomeEuropeancountries. We conclude that the MRSA epidemiological profile in SantaCatarinaissimilartothatfoundintherestofBrazil, withapredominanceofSCCmectypeIII,but theresistance rateswerelowerthanthosefoundintherestofBrazil.
A wide variety of complexes with clonal isolates were detected without evidence of clonal spread, and a small amountofhighgeneticdiversitywasfound.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorsthankCoordenac¸ãodeAperfeic¸oamentode Pes-soaldeNívelSuperior(CAPES),ConselhoNacionaldePesquisa e Desenvolvimento Tecnológico (CNPq) and Fundac¸ão de AmparoàPesquisadoRioGrandedoSul(FAPERGS)for finan-cialsupport.ThankstoLaboratórioSantaLuzia(CassiaZoccoli and Nina Tobouti) and Laboratório Santa Isabel (Reginaldo SimõesandMarceloMolinari)forgrantingclinicalsamples.
r
e
f
e
r
e
n
c
e
s
1.GalesAC,SaderHS,RibeiroJ,ZoccoliC,BarthA,PignatariAC. Antimicrobialsusceptibilityofgram-positivebacteriaisolated inBrazilianHospitalsParticipatingintheSENTRYProgram (2005–2008).BrazJInfectDis.2009;13:90–8.
2.OttoM.MRSAvirulenceandspread.CellMicrobiol. 2012;14:1513–21.
3.KoyamaN,InokoshiJ,TomodaH.Anti-infectiousagents againstMRSA.Molecules.2013;18:204–24.
4.HeroldBC,ImmergluckLC,MarananMC,etal.
Community-acquiredmethicillinresistantStaphylococcus aureusinchildrenwithnoidentifiedpredisposingrisk.JAMA. 1998;279:593–8.
5.FigueiredoAMS,FerreiraFA.Themultifacetedresourcesand microevolutionofthesuccessfulhumanandanimal pathogenmethicillin-resistantStaphylococcusaureus.Mem InstOswaldoCruz.2014;109:1–14.
6.ShoreAC,ColemanDC.Staphylococcalcassette
chromossomemec:recentsadvancesandnewinsights.IntJ MedMicrobiol.2013;303:350–9.
7.YamakiJ,LeeM,ShrinerKA,Wong-BeringerA.Canclinical andmolecularepidemiologicparametersguideempiric treatmentwithvancomycinformethicillin-resistant
Staphylococcusaureusinfections?DiagnMicrobiolInfectDis. 2011;70:124–30.
8.JorgensenJH,PfallerMA,CarrollKC,etal.Manualofclinical microbiology.11thed.Washington:ASMPress;2015.
10.EuropeanCommitteeonAntimicrobialSusceptibilityTesting (EUCAST).BreakpointtablesforinterpretationofMICsand zonediameters.Version3.0;2013.
11.VannuffelP,GigiJ,EzzedineH,etal.Specificdetectionof methicilinresistantStaphylococcusspeciesbymultiplexPCR.J ClinMicrobiol.1998;33:2864–7.
12.ZhangK,McClureJA,ElsayedS,LouieT,ConlyJM.Novel multiplexPCRassayforcharacterizationandconcomitant subtypingofstaphylococcalcassettechromosomemectypesI toVinmethicillin-resistantStaphylococcusaureus.JClin Microbiol.2003;43:5026–33.
13.OliveiraDC,LencastreH.MultiplexPCRstrategyforrapid identificationofstructuraltypesandvariantsofthemec
elementinmethicillin-resistantStaphylococcusaureus. AntimicrobAgentsChemother.2002;46:2155–61.
14.KhanSA,NawazMS,KhanAA,CernigliaCE.Simultaneous detectionoferythromycin-resistantmethylasegenesermA andermCfromStaphylococcusspp.Bymultiplex-PCR.MolCell Probes.1999;13:381–7.
15.LinaG,QuagliaA,ReverdyME,LeclercqR,VandeneschF, EtienneJ.Distributionofgenesencodingresistanceto macrolides,lincosamides,andstreptograminsamong Staphylococci.AntimicrobAgentsChemother.1999;43: 1062–6.
16.McDougalLK,StewardCD,KillgoreGE,ChaitramJM, McCallisterSK,TenoverFC.Pulsed-fieldgelelectrophoresis typingofoxacillin-resistantStaphylococcusaureusisolates fromtheUnitedStates:establishinganationaldatabase.J ClinMicrobiol.2003;41:5113–20.
17.PintoTCA,SouzaARV,DPinaSECM,etal.Optochin-Resistant
Streptococcuspneumoniae:PhenotypicandMolecular CharacterizationofIsolatesfromBrazilwithDescriptionof FiveNovelMutationsintheatpCGene.JClinMicrobiol. 2013;51:3242–9.
18.TenoverFC,ArbeitRD,GoeringRV,etal.Interpreting chromosomalDNArestrictionpatternsproducedby pulsed-fieldgelelectrophoresis:criteriaforbacterialstrain typing.JClinMicrobiol.1995;33:2233–9.
19.FariaNA,OliveiraDC,WesthH,etal.Epidemiologyof emergingmethicillin-resistantStaphylococcusaureus(MRSA) inDenmark:anationwidestudyinacountrywithlow prevalenceofMRSAinfection.JClinMicrobiol. 2005;43:1836–42.
20.ElstromP,KacelnikO,BruunT,IversenB,HaugeSH, AavitslandP.Meticillin-resistantStaphylococcusaureusin Norway,alow-incidencecountry,2006–2010.JHospInfect. 2012;80:36–40.
21.WorldHealthOrganization.Antimicrobialresistance–global reportonsurveillance.WorldHealthOrganization;2014.
22.OttoM.Community-associatedMRSA:whatmakesthem special?IntJMedMicrobiol.2013;303:324–30.
23.JonesRN,Guzman-BlancoM,GalesAC,etal.Susceptibility ratesinLatinAmericanNations:ReportfromaRegional ResistanceSurveillanceProgram(2011).BrazJInfectDis. 2013;17:672–81.
24.ToledoPV,ArendL,PilonettoM,etal.Surveillanceprogram formultidrugresistantbacteriainhealthcareassociated infections–acityperspectiveatSouthBrazil.JHospInfect. 2012;80:351–3.
25.KuoSC,ChiangMC,LeeWS,etal.Comparisonof
microbiologicalandclinicalcharacteristicsbasedonSCCmec
typinginpatientswithcommunity-onsetmeticillin-resistant
Staphylococcusaureus(MRSA)bacteraemia.IntJAntimicrob Agents.2011;39:22–6.
26.HuangH,FlynnNM,KingJH,MonchaudC,MoritaM,Cohen SH.Comparisonsofcommunity-associated
methicillin-resistantStaphylococcusaureus(MRSA)and hospital-associatedMRSAinfectionsinsacramento, California.JClinMicrobiol.2006;44:2423–7.
27.CavalcanteFS,SchuenkFP,CabocloRMF,FerreiraDC,Nouér SA,SantosKRN.Tetracyclineand
trimethoprim/sulfamethoxazoleatclinicallaboratory:can theyhelptocharacterizeStaphylococcusaureuscarrying differentSCCmectypes?RevSocBrasMedTrop.2013;46:100–2.
28.MaalejSM,RhimiFM,FinesM,MnifB,LeclercqR,Hammami A.Analysisofborderlineoxacillin-resistantStaphylococcus aureus(BORSA)strainsisolatedinTunisia.JClinMicrobiol. 2012;50:3345–8.
29.HanakiH,CuiL,DantsujiYI,etal.Antibioticsusceptibility surveyofblood–borneMRSAisolatesinJapanfrom2008 through2011.JInfectChemother.2014;20:527–34.
30.AppelbaumPC.Microbiologyofantibioticresistancein
Staphylococcusaureus.ClinInfectDis.2007;45:S165–70.
31.HowdenPH,DaviesJK,JohnsonPDR,StinearTP,GraysonML. ReducedvancomycinsusceptibilityinStaphylococcusaureus, includingvancomycin-intermediateandheterogeneous vancomycin-intermediatestrains:resistancemechanisms, laboratorydetection,andclinicalimplications.ClinMicrobiol Rev.2010;23:99–109.
32.FiebelkornKR,CrawfordSA,McelmeelML,JorgensenJH. Practicaldiskdiffusionmethodfordetectionofinducible clindamycinresistanceinStaphylococcusaureusand coagulase-negativeStaphylococci.JClinMicrobiol. 2003;41:4740–4.
33.ReiterKC,MachadoABMP,FreitasALP,BarthAL.High prevalenceofmethicillin-resistantStaphylococcusaureuswith SCCmectypeIIIincysticfibrosispatientsinsouthern,Brazil. RevSocBrasMedTrop.2010;43:377–81.
34.TrindadePA,PachecoRL,CostaSF,etal.PrevalenceofSCCmec
TypeIVinnosocomialbloodstreamisolatesof