Mortality among HIV-Infected Patients in Resource Limited Settings: A Case Controlled Analysis of Inpatients at a Community Care Center
Texto
Imagem
Documentos relacionados
After this study, minimally invasive mitral valve surgery, which had been limited to patients who had had no previous surgical intervention, started to be performed in patients
It should be considered that decrease the intraocular pressure has to be done in a controlled fashion in older patients under oral anticoagulant therapy and that had undergone
Objective : Because patients hospitalized in intensive care units are at risk for poor nutrition, and nutritional therapy is not always started at an appropriate time, the
over-all demand for medical care in a community can be determined through planning at the local level_ it is possible that the local authorities of both the Ministry of Health and
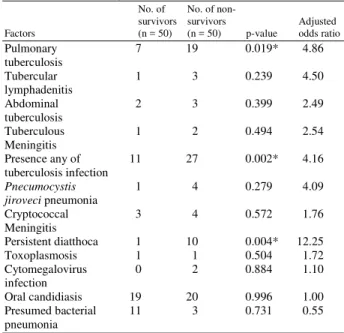
Defining the relative impact of specific HIV associated conditions on mortality during early ART will assist efforts to reduce the excess mortality associated with this period of
The effective bedside availability of the set of elements that comprise neonatal intensive care is also something that has not yet been achieved at all neonatal centers in the
isolation had been observed in the HIV-infected than in HIV-uninfected women, colonization and VVC showed similar frequency in both groups, indicating that HAART appears to
Considering that the immune reconstitution achieved by HAART has not been clearly established in pediatric HIV-1-infected patients and that influenza virus vaccine is recommended
